


1Department of Dermatology, and 2Department of Laboratory Medicine, Hualien Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, and Tzu Chi University, Hualien, Taiwan. *E-mail: md.hong@msa.hinet.net
Accepted Sep 18, 2019; E-published Sep 18, 2019
Purpureocillium lilacinum, previously known as Paecilomyces lilacinus, is a saprophytic and filamentous mould that exists in soil, decaying food, and paper. It can produce conidia and spores in human tissue, but it seldom results in infectious disease because of its low virulence (1, 2). Nonetheless, P. lilacinus has become an emerging pathogen in both immunocompromised and immunocompetent hosts recently (3–5). A chronic recalcitrant cutaneous ulcer induced by P. lilacinum is rare, and there is no consensus regarding its treatment. Treatment response to traditional antifungal agents, such as amphotericin B, fluconazole, griseofulvin, and echinocandins, was poor. Newer triazoles, including voriconazole and posaconazole, have lower minimum inhibitory concentration (MIC) in vitro. Previously reported patients with cutaneous infection treated with voriconazole responded well. However, only one patient was treated with posaconazole for 4 weeks but was lost to follow-up (3, 6). Herein, we describe a rare case of recurrent cutaneous P. lilacinum infection in a patient with Evans’ syndrome who was successfully treated with oral posaconazole and surgical debridement.
A male farmer in his 40s presented with painful papules on his right arm for a month and ulcerations on his left shin for 6 months. The lesions started as asymptomatic small erythematous papules that slowly progressed to painful ulcers surrounded by purpuric papules. The patient stated that he did not experience any trauma or have insect bites. He had a history of Evans’ syndrome and was treated with oral eltrombopag (50 mg/day) and prednisolone (10 mg/day) for more than 10 years. Azathioprine, mycophenolate, and dapsone were also given when acute exacerbation occurred. These lesions had a poor response to amoxicillin/clavulanic acid, levofloxacin, and fluconazole.
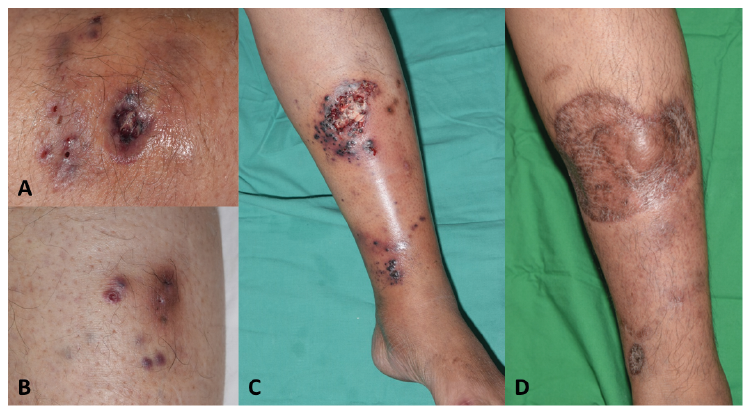
The physical examination revealed a 1.5-cm necrotic ulcer with several satellite, purpuric papules, and sinus tract and pus formation on the patient’s right arm (Fig. 1A). Several 0.5-cm ulcerative and purpuric papules were found on his left shin (Fig. 1B). Subsequently, an incisional biopsy was performed.
The histopathologic examination showed diffuse suppurative and granulomatous inflammation extending from the dermis to the subcutis layer without vasculitis or caseous necrosis. Non-pigmented spores and septate hyphae with a positive periodic acid-Schiff stain were found (Fig. 2A, B). Results of the tissue culture showed a woolly colony with a faint lilac colour in the centre and white colour in the peripheral area (Fig. 2C). Slide cultures revealed septate branching hyaline hyphae with elongated, tapering phialides and chain-like conidiophores (Fig. 2D). Cutaneous hyalohyphomycosis caused by Purpureocillium infection was diagnosed, based on findings from the mycological examinations and fungal culture. Genotypic identification of the clinical isolate by sequencing the internal transcribed spacer (ITS) region of the ribosomal RNA gene (7) confirmed P. lilacinum infection. The nucleotide sequence identity of the region was 100% P. lilacinum and matched the ribosomal RNA gene sequence deposited in the National Center for Biotechnology Information (GenBank: MK713625.1).
Oral voriconazole (400 mg daily) was given for 12 weeks, and his wounds healed completely. However, a recurrent deep necrotic ulcer surrounded by haemorrhagic bullae and papules developed on the same site on his left shin 5 months later after discontinuing voriconazole (Fig. 1C). Results of the biopsy and culture showed that the patient had recurrent P. lilacinum hyalohyphomycosis. The susceptibility test showed that the minimum inhibitory concentration (MIC) values for voriconazole and posaconazole were 0.5 mg/l and 1 mg/l. Then voriconazole was switched to oral posaconazole (300 mg daily) for 11 weeks, and surgical debridement followed by split-thickness skin grafting was performed. No recurrence was noted for more than 2 years (Fig. 1D).
Fig. 1. Photographs of the patient’s clinical course. A) A necrotic ulcer with peripheral sinus tract formation on the right forearm. B) Several brownish to violaceous papules and sinus tracts on the left anterior shin. C) A huge necrotic ulcer with peripheral haemorrhagic vesicles and bullae has developed after discontinuation of voriconazole for 5 months. D) Ulcers and bullae are resolved after posaconazole treatment (300 mg/day) for 11 weeks and surgical debridement with split-thickness skin grafting.
Fig. 2. Microscopic finding, fungal colony morphology, and slide culture. A) Multiple hyaline spores and branching hyphae with septa are found (haematoxylin and eosin stain, original magnification ×400). B) Grocott’s methenamine silver stain highlights the spores and hyphae (original magnification ×400). C) The fungal colony has a woolly surface with a faint lilac colour in the centre and white colour in the peripheral area (original magnification ×200). D) Long branching hyphae with septa, tapering phialides, and chain-like conidiophores are found.
P. lilacinum can invade multiple human organs and cause various infections. Oculomycosis accounted for the most cases (51.3%), and it led to cutaneous and subcutaneous infections (35.3%). The prevalence of cutaneous infection is still unknown. Forty-two cases were reported from 1977 to 2004 (1). It can be transmitted by both direct inoculation and hematogenous dissemination. Outbreaks induced by contaminated skin cream have been reported (8). The predisposing factors of the infection are malignancy, bone marrow transplantation, long-term glucocorticoid use, and other immunosuppressed conditions (1, 6, 8). Cutaneous infection rarely results in mortality, and the aetiology of death could not be attributed to fungal infection in such cases (1).
The clinical manifestation of P. lilacinum cutaneous infection can vary from small erythematous papules to plaques with central umbilication to haemorrhagic vesicle or ulceration (1, 4, 6, 8–11). Cellulitis-like lesions or subcutaneous nodules have been also reported (8). Some lesions may be asymptomatic. Lower extremities were affected more frequently in one series of patients due to traumatic insults (8). Thus, skin biopsy with a tissue culture is the gold standard method for diagnosis. In histopathological examinations, P. lilacinus infection usually revealed suppurative and granulomatous inflammation with septate and branching hyaline hyphae, also known as hyalohyphomycosis (4). Fungal elements can be found within the granuloma and even in the stratum corneum (8). Cultivation of P. lilacinum from lesions is still the gold standard for making the diagnosis. It can grow on routine fungal culture media, and its growth has been characterised by violaceous colonies with a woolly surface (8, 6, 10). Additionally, it has been characterised by septate, branching hyaline hyphae, and phialides tapering at its distal end and as chain-like conidiophores in slide cultures (4). Genotypic identification could provide an accurate and timely fungal identification.
P. lilacinum infection must be diagnosed correctly and timely because it is resistant to conventional antifungal agents, including amphotericin B, terbinafine, griseofulvin, ketoconazole, and echinocandins. Newer triazoles, such as voriconazole, posaconazole, and ravuconazole, had a lower MIC in vitro (3). Rimawi et al. (6) reviewed 6 published cases of cutaneous P. lilacinum infection from 2000 to 2012. Those patients were cured by voriconazole in combination with or without surgery. However, their reviews might have reporting bias, and the role of surgery was not clarified. Rimawi et al. suggested that individualised assessments were required for surgical interventions. A patient with cutaneous P. lilacinum infection treated with oral posaconazole showed remarkable improvement at week 4, but the patient was lost to follow-up (9). In our case, the patient did not have any recurrence for 2 years. However, the low MIC levels of voriconazole and posaconazole in the current isolate did not correlate with the clinical response. Voriconazole and posaconazole have different pharmacokinetic properties, metabolic pathways, and drug-drug interactions. Apparently, the outcome is affected by not only MIC level but also the factors above. We suggest that posaconazole should be considered as an alternative treatment if voriconazole fails, and surgical intervention should be considered in patients with prolonged and recalcitrant ulcers.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize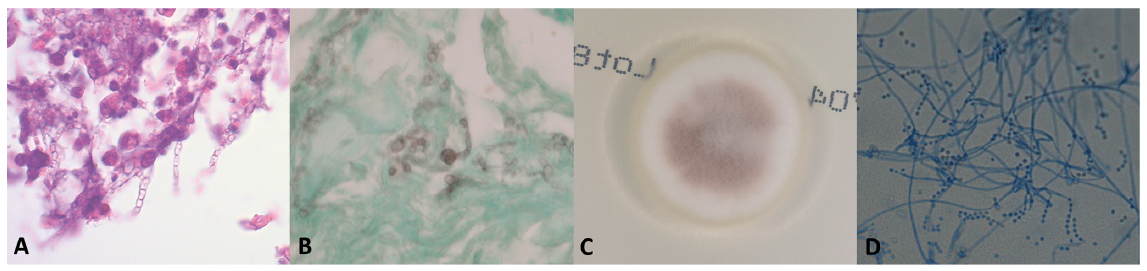 Click to show fullsize
Click to show fullsize