


1Department of Dermatology and 4Institute of Human Genetics, University Hospital Magdeburg, University of Magdeburg, Magdeburg, Germany, 2S-Biomedic NV, Beerse, Belgium, 3Department of Biomedicine, Aarhus University, Aarhus, Denmark, and 5Department of Health and Experimental Science, Pompeu Fabra University, Barcelona, Spain
#These authors contributed equally to this paper.
Imbalance in skin microflora, particularly related to certain Cutibacterium acnes strains, may trigger acne. Application of non-acne-causing strains to the skin may modulate the skin microbiome and thereby lead to a reduction in acne. This pilot study evaluates the safety and efficacy of microbiome modulation on acne-prone skin. The study had 2 phases: active induction (5% benzoyl peroxide gel, 7 days) and interventional C. acnes strains treatment (5 weeks). Patients were randomized to either topical skin formulations PT1 (2 strains of C. acnes Single Locus Sequence Typing [SLST] type C3 and K8, 50% each) or PT2 (4 strains of C. acnes SLST type C3 [55%], K8 [5%], A5 [30%] and F4 [10%]). Safety and efficacy was evaluated in 14 patients (PT1=8/14, PT2=6/14). Skin microbiome composition shifted towards study formulations. No untoward adverse events, visible irritation, or significant flare-up were observed. Non-inflamed lesions and skin pH were reduced. Comedone counts improved clinically with no deterioration in inflammatory lesions.
Key words: acne vulgaris; microbiome; skin.
Accepted Sep 25, 2019; E-published Sep 25, 2019
Acta Derm Venereol 2020; XX: XX–XX.
Corr: Bernhard Pätzold, S-Biomedic, Turnhoutsweg 30, BE-2340 Beerse, Belgium. E-mail: Bernhard.Paetzold@sbiomedic.com
This open-label, pilot study enrolled men and women (18–23 years) with acne vulgaris. In 14 enrolled patients, skin microbiome composition shifted towards study formulations. No untoward tolerability, visible irritation, or significant flare-ups were observed. Non-inflamed lesions and skin pH were reduced. Modulation of Cutibacterium acnes towards the non-acne causing strains on the skin of patients with acne was safe. C. acnes was formerly thought to be the cardinal cause of acne; however, recently some, but not all, strains of C. acnes were found to be responsible. This microbiome modulation approach as therapy requires validation in future clinical studies.
Acne vulgaris originates in the pilosebaceous unit of the skin. Increased and modified sebum production, disturbance of follicular keratinocyte differentiation and release of inflammatory mediators are the primary driving forces of acne (1). The second step in the pathogenic cascade is colonization of this unit by Propionibacterium acnes, now known as Cutibacterium acnes, a commensal bacteria, followed by additional triggering of inflammation (2, 3). The last decade has not witnessed many therapeutic innovations for acne, nevertheless, newer insights into the pathogenesis of acne is the backbone of current innovations in this field (4).
C. acnes is accepted as a trigger for acne, but recent studies utilizing the latest molecular methods reveal that imbalance between the varied microorganisms of the skin microflora and different strains of C. acnes may explain its role in the disease in greater detail, while leaving the question of cause or consequence unanswered (5–7). Studies have also reported that certain strains of C. acnes may trigger endoplasmic reticulum stress (and subsequent apoptosis) that could be attributed to trans-10, cis-12 conjugated linoleic acid produced by linoleic isomerase expressed by these strains (8, 9). Such stress is potentially caused by the activation of lipid mediators (via peroxisome proliferators-activated receptors activation) and contributes to the pathogenesis of acne (9, 10). This led to the hypothesis that replacing the C. acnes strains related to the inflammatory process (high production of linoleic isomerase) on the acne skin with those strains that are not associated (low linoleic isomerase production) with inflammation, might reduce the degree of acne. Moreover, such therapy may help in avoiding the topical and systemic adverse events identified with the currently used therapies, often leading to reduced adherence (11, 12).
To address this hypothesis, a proof-of-principle study was conducted in healthy participants in different acne-prone skin areas to demonstrate that new strains of the resident skin microbiota can be successfully transferred to a recipient. The results of this study demonstrate that the composition of the skin microbiome could be modified at the C. acnes strain level within a few days and no major safety events were identified (13). Of note, in microbiome modulation studies unlike traditional studies, the endpoint is not the reduction in the microbial load, but a shift towards the beneficial microbial strains and the resultant reduction in the disease (such as acne). The aim of the current pilot study was to gather further evidence on the feasibility, safety and efficacy of direct microbiome modulation by transferring beneficial C. acnes strains in patients with acne-prone skin.
This open-label, pilot study was approved by the ethics committee of the University of Magdeburg, all patients provided written consent and precautions applicable to dermatological studies were followed (German Clinical Trials Registry number: DRKS00015717). Men and women (18–23 years) with mild-to-moderate acne vulgaris, based on Leeds acne grading system (Leeds score between 1.5 and 4), who were otherwise healthy were included in this study. The Leeds acne grading system assesses the severity of acne using Leeds scores ranging from grade 1 (least severe) to 12 (most severe) (14). In this study, patients with maximum grade 4 (can be described as moderate) were included. Patients with more severe acne (higher Leeds score) were not included. Most patients reported that they have had acne since puberty (mean starting age 14.6 years). Patients who had non-acne-related irritated facial skin (desquamation, dryness), skin conditions, such as atopic dermatitis or eczema, or were being treated with peeling and other adjunctive therapies were excluded from the study.
The study comprised 2 phases: an active induction phase with 5% benzoyl peroxide gel (BPO, 7 days) and an interventional microbiome treatment phase (5 weeks). In the first phase BPO is used for significant depletion of the skin microflora. After clearing the ecological niche, the new C. acnes strains were applied in phase 2 to colonize the skin. On day 1, post-enrollment, facial skin of the patients was evaluated based on lesion count, along with the analysis of microbiome and pH measurements. Patients were provided with an over-the-counter skin cleanser (Quick & Clean Waschgel and Augen Make-Up Entferner, 150 ml Tube, Bebe) for use during the entire trial (to replace their daily cleanser) and BPO (Akneroxid Gel 50 mg/g, Almirall Hermal GmbH, Hamburg) for once daily application during the induction phase for down-regulation of the facial microbiota in the first 7 days. Otherwise the patients were encouraged not to change any of their daily habits concerning physical activity and nutrition. In addition, the patients were provided with a diary to record daily activities that may affect facial skin (general health conditions, concomitant drug intake sunbathing, excessive sports, etc.) and a short questionnaire to document their perception about their skin.
On day 7 (start of first treatment phase), the facial skin parameters were re-assessed using pH and analysis of the skin microbiome. Patients were then randomized to 1 of the 2 topical skin formulations probiotic topical 1 (PT1: 2 strains of C. acnes Single Locus Sequence Typing [SLST] type C3 and K8, 50% each) or probiotic topical 2 (PT2: 4 strains of C. acnes SLST type C3 [55%], K8 [5%], A5 [30%] and F4 [10%]) each with a combined total concentration of 106 colony forming units/g. Each application was provided as single use and contained 1 g gel. The strain mixtures were chosen either to reflect a natural mixture of strains or an equal mix of the strains. The facial skin microbiome of healthy individuals is usually dominated by strains that are from the clade 1A-1. An earlier study observed that mixtures of strains can have synergistic effects on the engraftment of the applied bacteria. Therefore, strains from different parts of the evolutionary tree were included in our probiotic mixtures. The rationale for the strain selection was low production of linoleic acid isomerase determined by the produced amount of the conjugated linoleic acid (15), thereby suppressing inflammation.
All of the strains were cultivated to exponential phase, harvested and later stabilized in a gel formulation for application. Bacteria were grown in a 500 ml basic medium (20 g/l yeast extract, 5 g/l NaCl and 30 g/l dextrose) at 37°C. As an inoculum 10 ml of an optical density (OD) 0.4 pre-culture grown in reinforced clostridial medium and reinforced clostridial agar (RCM) media was used. Cells were harvested after 3 days in the exponential phase and washed twice in a 0.25% peptone solution and normalized to an OD of 1. The normalized cultures were then mixed in the respective ratios. The final solutions were thickened with hydroxyethyl-cellulose 250 HX and left to rest for 1 h before being aliquoted. Each aliquot was 1 ml gel (pH=6.7) stored in an enteral syringe for single-use topical application. The aliquots with the gel containing the live bacteria were stored at –80°C for long-term storage. Each week patients would receive a fresh package of aliquots for use. Stability data on the long-term (Fig. S1) and short-term storage (Fig. S2) is provided. Colony forming unit counts were performed on RCM agar plate and serial dilution of the sample. The formulations were to be applied twice daily throughout the treatment phase (5 weeks) and fresh formulations were provided for application every week. Skin analyses were repeated on day 28 (parameters similar to day 7). At the end of treatment, on day 42, the skin was reassessed (same parameters as baseline). Safety was assessed at every visit by visual evaluation of the redness, irritation or any other skin problems (desquamation, itching or lesion deterioration). The blinding of the formulations was carried out by the study staff.
The facial skin microbiome of the patients was sampled by rubbing a sterile swab over the skin for 30 s to collect the micro-organisms. For sample collection, patients were instructed not to use the formulations in the morning and not to wash their faces for up to 3 h before the visit. This was done to ensure that a sufficient time interval was maintained from formulation application to sample collection. The sample collected at day 1 (upon randomization) was the baseline sample and all the other samples were compared with this baseline. Epicentre swabs were used in combination with the Extract-N-Amp kit (Sigma Aldrich Prod No. XNAP2) and samples were processed as described by Flores et al. (16). Subsequently, to identify the specific strains that increased with respect to the baseline sample, the SLST region and the 16S rRNA v3-v4 (17, 18) were amplified and sequenced on MiSeq v3 chemistry with 2*300 bp paired reads. The v3-v4 primers were preferred as they help to estimate better the non-C. acnes species on the skin compared with the v1-v3 primers (underestimation of the C. acnes population was acceptable) (18). The total number of operational taxonomic units (OTUs) were detected using the software Mothur (University of Michigan, Ann Arbor, MI, USA). The SLST amplification and analysis was performed as described previously (13).
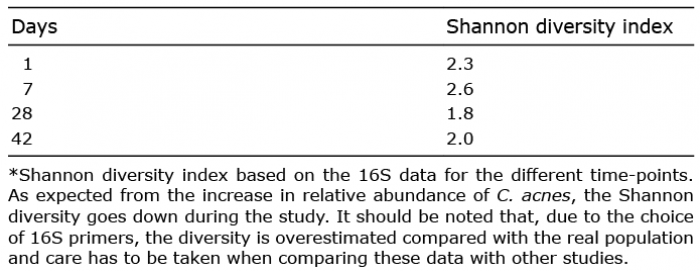
For the diversity analysis of C. acnes strains, Shannon diversity index by means of 16S rRNA at different time-points was used. This gives an indication of the genetic diversity of strains within the bacterial community. Safety parameters were assessed by a board-certified dermatologist at every visit. The dermatologist also assessed lesion counts by counting the inflamed and non-inflamed lesions on the face of the patients and reviewed the patient diaries. The skin pH was measured with a skin pH-meter PH 905 (Courage Khazaka). A descriptive analysis was performed for all continuous variables and data are presented as number, mean and standard deviation (SD). p-values (Wilcoxon rank test) were also calculated for the efficacy parameters.
In this study, conducted at the Department of Dermatology in Magdeburg (September to November 2016), a total of 8 patients were randomized to formulation PT1 (age, mean (SD) 19.6 (1.5) years) and 6 to the formulation PT2 (age 20 (2) years). All patients had a mean Leeds score < 3.1 (mild to moderate disease) at the end of the study.
The 16S rDNA analysis of the overall composition of bacterial species demonstrated an initial decrease of C. acnes after application of BPO (day 7), followed by an increase after application of the topical skin formulation for 2 weeks (day 21). At the end of the treatment (day 42) the overall C. acnes proportion was higher compared with baseline and day 7 (day 1=37.5%, day 7=32.4%, day 21=57.7%, day 42=50.9%); however, this was slightly lower compared with day 21. This demonstrates that the relative abundance of C. acnes nearly doubled in 21 days. The Shannon diversity index increased after the disinfection period and subsequently decreased again (Table I). Similar patterns have been observed from microbiome studies on deodorants and antiperspirants on the axillary bacterial community (19).
Table I. Shannon diversity index*
For assessing change in C. acnes strain composition in the microbiome samples from baseline, an SLST was used. In the 16S analysis a total of 663 OTUs were detected. Commonly found strains were dominant in most samples on day 1. A shift in the composition of the skin microbiome to the mixed strains present in both the topical formulations was observed (Fig. 1). There were no untoward safety or tolerability events observed during the study. The patients did not have any visible signs of irritation or significant flare-up and no adverse events were communicated by the patients or observed by the study team.
Fig. 1. Skin microbiome-shift in relative abundance of C. acnes strain. (a) Strain level shift. PT1: probiotic topical 1; PT2: probiotic topical 2. (b) Overall shift (>3% shift).
A significant reduction in non-inflamed lesions (open and closed comedones) was observed with both the topical formulations (Table II). The number of inflamed lesions (papules and pustules) did not change significantly with respect to the baseline. Although a trend of a decrease in skin pH was observed, this was not statistically significant (Table II, Fig. 2).
Table II. Safety and efficacy parameters
Fig. 2. Skin pH of the patients throughout the study. Data are presented as median ± interquartile range.
This pilot study demonstrated the feasibility and safety of direct microbiome modulation by transferring beneficial C. acnes strains to patients with acne-prone skin. This study generates further evidence to support recent findings, which suggests that the community composition of C. acnes might be more relevant in acne compared with the C. acnes count (20).
In multiple studies, faecal microbiota transplantation (FMT) has been used successfully as therapy for displacing certain pathogenic bacteria, including C. difficile, K. pneumoniae, and vancomycin-resistant Enterococcus (21). For preparing the patients for an FMT, microbiota depletion is required, and the most commonly used methods include non-absorbable antibiotics, systemic antibiotics or antibiotic-free osmotic cleanses (21). Similarly, for preparing the acne patients for skin microbiome modulation, BPO has been used in the current study for significant depletion of the skin microflora. Previously, a study has revealed that the non-inflamed lesion count nearly doubled 4 weeks after completion of long-term BPO treatment (3 months) (11); however, in the current study it was observed that the non-inflamed lesion count was reduced significantly at 6 weeks post-BPO treatment; therefore, this effect could be attributed to the PT1 or PT2 formulations. This finding is particularly important since the non-inflamed lesions, i.e. microcomedones dominant in preadolescent acne, are the origin of the inflamed lesions. In this study, carefully selected strains from the C. acnes phylotypes IA-1 and II were used. While multiple studies have previously identified phylotype II as “health”-associated, there is no clear consensus on the IA clade (2, 6, 22). Likewise, more sophisticated whole-genome sequencing metagenomics did not contribute to a mechanistic understanding of the bacteria host interaction beyond previous knowledge. A clear consensus on the biomarker for a causative role of C. acnes strains in acne has not yet been established. In fact, in some aspects the clade IA-1 strain seems less immunogenic than phylotypes IA-II strains (23). Our findings support the view that a simple classification of pathogenicity based on the phylotype level, while convenient, is not adequate for the complex relationship between the bacteria and the host. In fact, recent studies found positive traits of C. acnes on the host supporting a potential symbiotic relationship (24, 25). These findings highlight that further research is necessary to fully understand the positive and negative role of C. acnes in skin homeostasis.
In this pilot study, due to the small sample size, short treatment duration, and lack of control/placebo group, no definitive conclusions can be made on the efficacy of the formulations. Nevertheless, transplantation of the beneficial strains of C. acnes did not lead to deterioration of the acne lesions and clinical improvements were observed in this pilot study in particular, in comedone counts when comparing end-of-treatment with the baseline assessments. There could be some evidence that the modulation of strains may interfere with the follicular cast environment leading to the observed reduction in comedone formation. Further clinical investigations of stability, efficacy, and safety of direct microbiome modulation with these first-in-class products in the patient with acne are warranted.
Sonia Philipose, PhD, and Varkha Agrawal, PhD, provided writing assistance and Sangita Patil, PhD, ISMPP CMPP® (SIRO Clinpharm Pvt. Ltd, India), provided additional editorial support for this manuscript. Dr Paul Soons provided expert review during the development of the manuscript. The authors also thank the study participants, without whom this study would never have been accomplished, and the investigators for their participation in this study.
This study was supported by funding from by an “EGO Gruendungstransfer” grant from government of Saxony Anhalt in collaboration with the European Regional Development Fund (ERDF/EFRE).
Conflicts of interest: MG, JPL, BP are employees of S-Biomedic and may hold stock or stock options. BP and JPL were employees of the University Clinic of Madgeburg at the time of the study.


 Click to show fullsize
Click to show fullsize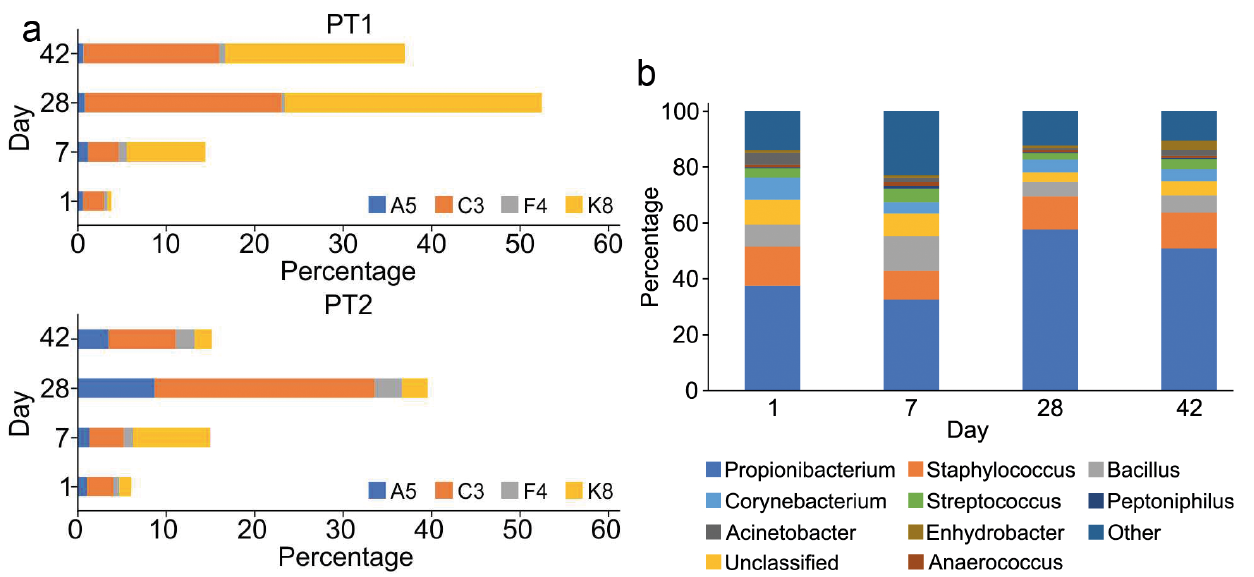 Click to show fullsize
Click to show fullsize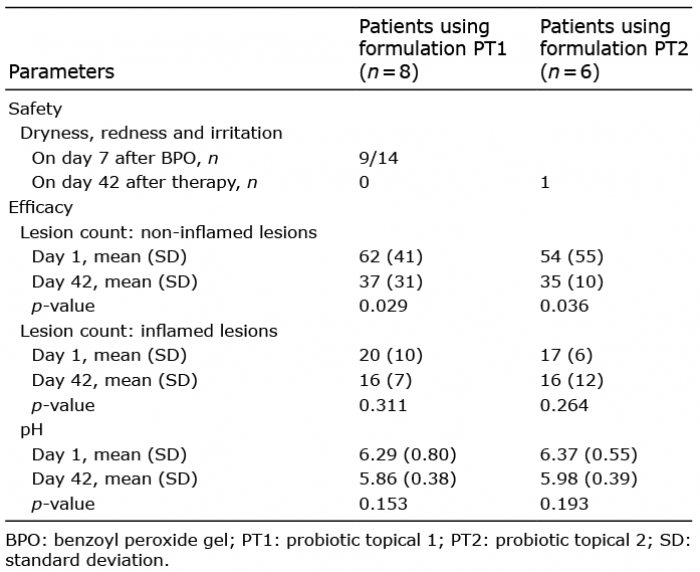 Click to show fullsize
Click to show fullsize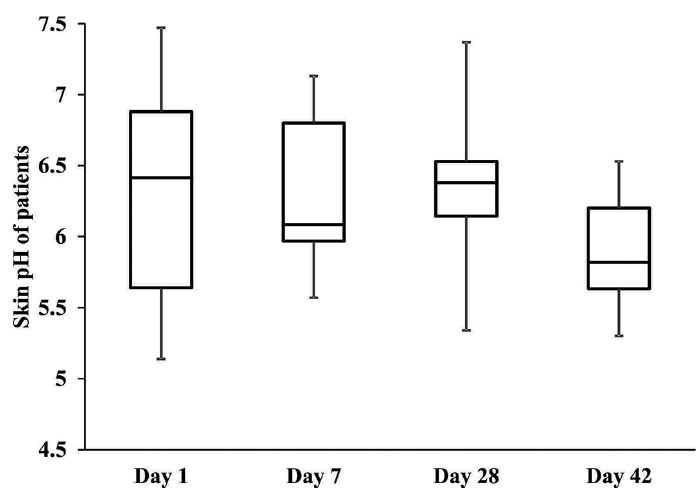 Click to show fullsize
Click to show fullsize