


1Department of Internal Medicine, Chris Hani Baragwanath Academic Hospital, Faculty of Health Sciences, 2Department of Chemical Pathology, National Health Laboratory Service and Faculty of Health Sciences, 3Department of Dermatology, Faculty of Health Sciences, and 4Department of Radiology, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
As part of a larger cross-sectional, case-control study on cardiometabolic diseases in psoriasis this study investigated the association of visceral fat and serum adipokines with psoriasis and cardiometabolic diseases. A total of 103 patients with psoriasis and 98 controls, matched for body mass index, ethnicity and sex, were recruited over 15 months. Abdominal visceral fat was measured by computerized tomo-graphy. Logistic regression analysis revealed that visceral fat was associated with psoriasis (odds ratio (95% confidence interval): 1.56 (1.15, 2.11)), hyper-triglyceridaemia (1.67 (1.22, 2.28)), low high-density lipoprotein (1.63 (1.19, 2.22)) and type 2 diabetes (1.77 (1.24, 2.54)), (p < 0.005 for all). These respective associations were linked to serum interleukin-6, adiponectin, tumour necrosis factor and insulin resistance. Psoriasis was associated with type 2 diabetes (7.94 (2.64, 23.9)), independent of visceral fat. These data suggest that visceral fat and its mediators play a key role in psoriasis-associated cardiometabolic diseases. Psoriasis itself is associated with an increased risk of type 2 diabetes.
Key words: psoriasis; cardiometabolic disease; cardiovascular disease; visceral fat; adipokines; metabolic syndrome.
Accepted Oct 2, 2019; E-published Oct 3, 2019
Acta Derm Venereol 2020; 100: XX–XX.
Corr: Nasrin Goolam Mahyoodeen, Department of Internal Medicine, Chris Hani Baragwanath Academic Hospital, PO Box Bertsham 2013, Johannesburg, South Africa. E-mail: mahyoodeen@yahoo.com
Abdominal obesity is common in patients with psoriasis. This study examined the relationship of abdominal fat, measured by computed tomography, in relation to metabolic diseases in a cohort of 103 patients with psoriasis and 98 control subjects. The results showed that increased visceral fat and related hormones were associated with an increased risk of psoriasis, type 2 diabetes and abnormal levels of lipids. Psoriasis was a risk factor for type 2 diabetes independent of abdominal fat. These findings show the importance of abdominal fat as a risk factor for psoriasis and metabolic diseases.
There is strong epidemiological evidence demonstrating that patients with psoriasis have an increased risk of cardiometabolic diseases (CMDs) (1–3). In particular, psoriasis has been shown to be associated with obesity (4), particularly abdominal obesity (5), type 2 diabetes (T2D), hypertension, coronary artery disease and decreased life expectancy (6). The pathological basis for the link between psoriasis and CMDs is not fully understood. One hypothesis is that the chronic inflammatory state of psoriasis triggers a “psoriatic march”, whereby the pro-inflammatory milieu leads to insulin resistance and endothelial cell dysfunction, predisposing to CMDs (7). Chronic inflammation predisposes to accelerated atherosclerosis and other CMDs (8) via pro-inflammatory mediators and activated immune cells. Obesity has been shown to be associated with low-grade chronic inflammation (9). Adipocytes of visceral fat are immunologically active and secrete mainly pro-inflammatory adipokines, including leptin, visfatin, and resistin (10). Adiponectin, in contrast, has been shown to improve insulin sensitivity and have anti-inflammatory properties (11). Other pro-inflammatory factors that are produced mainly by macrophages within visceral fat include tumour necrosis factor (TNF), interleukin (IL)-1, and IL-6, all of which have been shown to directly or indirectly affect endothelial cell function and insulin sensitivity (12).
Patients with psoriasis have high levels of inflammatory markers, with C-reactive protein (CRP) (13), leptin (14) and TNF serum concentrations being significantly higher than in controls, whilst adiponectin levels are lower (14). While previous studies have separately shown an increased prevalence of CMDs (1), adipokine dysregulation (15) and increased visceral fat in psoriasis (16), to date no studies have assessed these relationships in a single cohort. The aim of the present study was therefore to determine whether psoriasis is associated with increased visceral adiposity and inflammation and whether visceral adipose tissue mediates the relationship between psoriasis and CMDs.
This was a cross-sectional case-control study of consenting adult psoriasis patients, 18 years and older, including those with psoriatic arthritis (PsA) recruited from the Dermatology and Rheumatology clinics at 3 academic hospitals in Johannesburg, South Africa from January 2015 to September 2016. The diagnosis of psoriasis and/or PsA was made by a dermatologist and/or rheumatologist. Exclusion criteria were human immunodeficiency virus infection, inflammatory arthritis due to another cause, and pregnancy. Control subjects had no known chronic inflammatory disorder and were matched with the patient group for geographical area of residence, sex, ethnicity, and body mass index (BMI). The study was approved by the University of the Witwatersrand Human Research Ethics Committee (M1403100).
Socio-demographic and clinical data collection
Clinical data were collected from hospital records, patient interviews and clinical examination, and included the presence of PsA, severity of psoriasis, and therapy used for psoriasis treatment. The severity of cutaneous involvement was assessed using the Psoriasis Area and Severity Index (PASI) score (17). Four types of anti-psoriatic therapy were recorded: topical therapy, oral metho-trexate, oral acitretin and other immunosuppressive agents, i.e. cyclosporine and leflunomide.
Ethnicity (black African, Asian-Indian, Caucasian, mixed ancestry) was assigned based on self-reporting by study participants. Socio-economic status (SES) was assessed using a locally validated questionnaire based on an individual’s access to a defined list of 12 household items (18). A score of 10 or more was categorized as high SES. Smoking status was categorized as either current/ex-smoker or never smoked. Education level was classified as to whether or not a participant had graduated from high school.
Blood pressure, anthropometric and body fat measurements
Blood pressure (mmHg) was measured with the subject seated. A minimum of 2 readings were taken 10 min apart and the mean of the readings was recorded. Weight, in kg, was measured in subjects with light clothing, without shoes. It was used together with height, measured to the nearest cm, to calculate the BMI. Waist circumference was measured at the mid-point of the upper border of the iliac crest and the lower border of the last rib using a soft tape measure. Hip circumference was measured around the widest portion of the buttocks. Subcutaneous and visceral fat were measured using a multidetector CT scan (Brilliance 16, Philips, the Netherlands). Non-contrast axial images were obtained at the level of the L4/L5 intervertebral space. Sixteen 3-mm contiguous slices were obtained at 3-mm increments (KVP 120, mAs 250, FOV 350 mm, matrix 512 × 512). These images were analysed using the open-source image analysis software Osirix (Osirix Foundation, Geneva, Switzerland). Using multiplanar reformatting, 7 slices were selected immediately below the L4 pedicle to the level of the L4/L5 disc for measurements of visceral and subcutaneous fat (19).
Laboratory investigations
Venous blood samples were obtained at the time of clinical examination after an overnight fast. Plasma glucose and serum lipids (total cholesterol, triglycerides and high-density lipoprotein (HDL) cholesterol), were measured using enzymatic methods on the ADVIA 1800 Chemistry Systems Analyser (Siemens Healthcare Diagnostics, Tarrytown, NY, USA). Low-density lipoprotein (LDL) cholesterol was calculated using the Friedewald formula (20). High-sensitivity C-reactive protein (hsCRP) and insulin were measured using a chemiluminescence-based assay on the ARCHITECT c8000 System (Abbott, Lake Forest, IL, USA). The homeostasis model assessment (HOMA) method was used to calculate insulin resistance (18). Leptin (Biovendor Research and Diagnostic Products, Czech Republic), TNF (Quantikine R&D Systems, Abingdon, UK), adiponectin (Quantikine R&D Systems), and IL-6 (Quantikine R&D Systems) were measured using immunoassays.
Diagnosis of cardiometabolic diseases
Subjects were defined as having the metabolic syndrome (MetS) using the 2009 harmonized guidelines (21). Patients with pre-existing T2D and hypertension were identified based on self-reporting by the patient and a review of clinical records. Newly diagnosed diabetes was defined as a fasting plasma glucose >7 mmol/l (22). Newly diagnosed hypertension was defined as per the harmonized guidelines (21). Raised total and LDL cholesterol were each defined according to the South African dyslipidaemia guideline consensus statement (23).
Statistical methods
All analyses were performed using Statistica version 13.2 (StatSoft, Tulsa, OK, USA). The sample size was calculated on the basis of a minimum effect size (r2) of 0.15, with 80% power at the 5% significance level and a maximum of 11 predictor variables per regression model. This gives a final sample size of 122 subjects. Full data was collected on 149 subjects, including CT measures. Descriptive statistics are presented as mean ± standard deviation (SD) or median and interquartile range (IQR) for continuous variables with normal or skewed distribution, respectively, and as proportions (%) for categorical variables. Categorical variables were compared across groups using the χ2 test. Skewed data were log transformed to normality before being analysed using parametric statistical tests. The Students unpaired t-test was applied to compare continuous variables between groups. Univariate regression analyses (Table SI) were performed for each of these outcome variables against those study variables for which data from the literature suggests a scientifically plausible association. Variables with a p < 0.20 in the univariate analysis were included in the multivariable model. Multivariable logistic regression was used to determine independent the risk factors/predictors for psoriasis and cardiometabolic disorders of MetS, T2D, hypertension, hypertriglyceridaemia, hypercholesterolaemia, high LDL and low HDL cholesterol. Backward, stepwise removal of non-significant variables was performed until only those with p < 0.05 remained in the model. Multicollinearity was assessed using the variance inflation factor (VIF) and variables with a VIF > 5.0 were excluded from the model. Particular attention was given to multivariable models in which visceral fat and/or psoriasis were included in the initial model. In those models where either variable did not continue through to the final model, forward regression analysis was performed to determine which variable was responsible for attenuating their effect on the particular outcome variable. The variables chosen for addition to the forward regression model were any of those included in the initial multivariable model and particularly those that continued through to the final model. Variables were chosen based on scientific plausibility.
Clinical, socio-demographic, biochemical and anthropo-metric characteristics of patients and controls
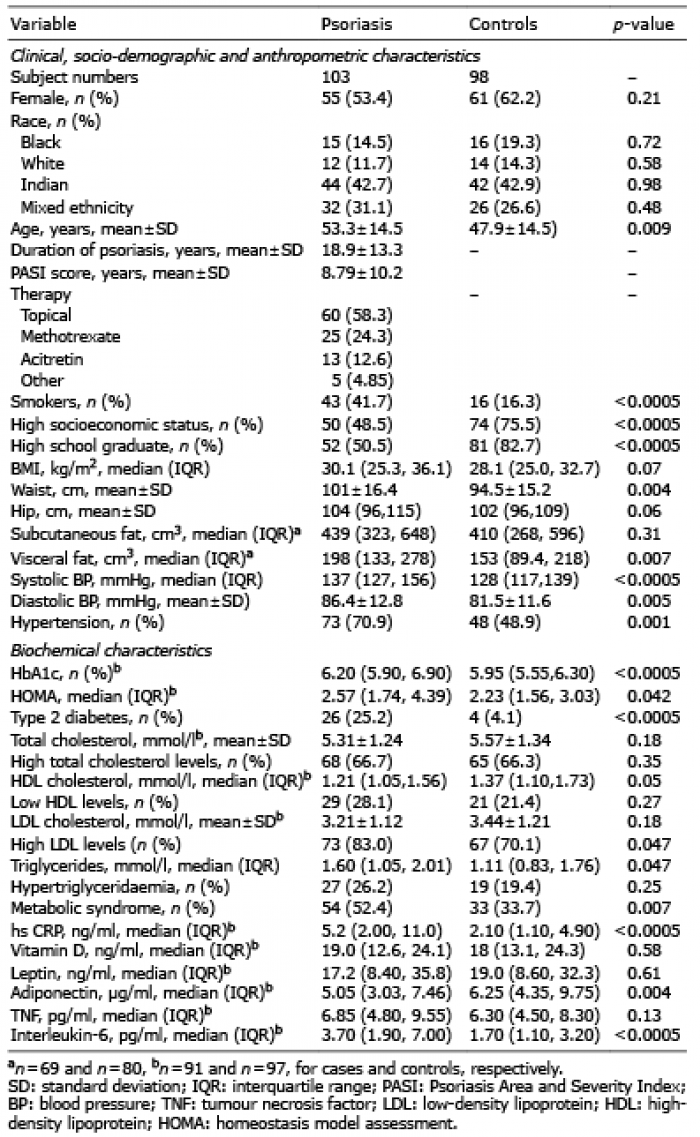
Table I summarizes the clinical, socio-demographic, biochemical and anthropometric characteristics of the patient and control groups. The mean (SD) disease duration of psoriasis was 18.9 (13.3) years, and 28 (27.1%) of psoriasis patients had PsA. The mean waist circumference was significantly higher in the psoriasis compared with control group (p = 0.004), but BMI was not significantly different. The psoriasis group had a significantly higher visceral fat volume compared with the control group (p = 0.007), but no difference was observed with respect to subcutaneous fat volume. Hypertension was more prevalent in the psoriasis group (p = 0.001) (Table I).
With reference to the metabolic variables and adi-pokine levels, HbA1c (p < 0.0001), HOMA, (p = 0.042), triglycerides (p = 0.047), hsCRP (p < 0.0001) and IL-6 (p < 0.0001) were all higher in the psoriasis group, whilst adiponectin (p = 0.004) was lower (Table I). The prevalence of T2D (p < 0.0005), high LDL cholesterol levels (p = 0.047) and MetS (p = 0.007) were significantly higher in the psoriasis group. Sub-group analysis showed no differences in prevalence of cardiometabolic diseases between treatment groups.
Table I. Clinical, socio-demographic, anthropometric and biochemical characteristics
Association of psoriasis and visceral fat with cardiometa-bolic diseases
In the univariate logistic regression analysis, psoriasis was a significant risk factor for MetS (p = 0.008), T2D (p = 0.0002) and hypertension (p = 0.002) and marginally for high LDL cholesterol (p = 0.05), but not so for any of the other measures of dyslipidaemia (Table II). Visceral fat was a significant risk factor for psoriasis (p = 0.004), MetS (p < 0.0001), T2D (p = 0.002), hypertension (p < 0.0001), hyper-triglyceridaemia (p = 0.001) and low HDL cholesterol levels (p = 0.002).
Table II. Associations of psoriasis with risk of cardiometabolic diseases and visceral fat with risk of cardiometabolic diseases and psoriasis
Multivariable logistic regression analysis (Table III) showed that lower education level (p = 0.0001), smoking (p < 0.0001) and IL-6 (p < 0.0001) were predictors of psoriasis (Table III, model 1). Psoriasis was a significant predictor of T2D (p = 0.002), as were age (p = 0.025) and HOMA (p < 0.0001) (model 2). The predictors of MetS (model 3) were low SES (p = 0.026), HOMA (p = 0.002), TNF (p = 0.008) and visceral fat (p = 0.003). The only variable associated with hypertension risk (model 4) was visceral fat (p < 0.0001). Low adiponectin levels, age and hip circumference were associated with hypertriglyceridaemia (p = 0.011, 0.041 and 0.035, respectively; model 5). Predictors of low HDL cholesterol levels (model 6) were hip circumference (p = 0.009), low adiponectin (p = 0.0008) and TNF levels (p = 0.01). The only predictor of high cholesterol levels (model 7) was age (p = 0.003). Age (p < 0.0001) and Indian ethnicity (p = 0.008) were associated with a higher risk of high LDL cholesterol (model 8). In order to determine the effect of PsA on CMD risk, models 2 to 8 were repeated with psoriasis replaced by coding for psoriasis only and PsA. The only model affected was that for T2D (model 2) where both psoriasis only and PsA remained in the final model with odds ratios (ORs) (95% confidence intervals; CI) of 7.60 (1.86, 31.1), p = 0.004 and 8.88 (1.90, 41.4), p = 0.005, respectively. Age and HOMA remained in the final model with ORs very similar to those shown in Table III.
Table III. Significant predictors of psoriasis and cardiometabolic diseases
There were several univariate analyses in which either visceral fat or psoriasis were significantly associated with the outcome variable, but did not remain significant in the multivariable model. These models were further analysed using forward regression analyses to determine which independent variable was responsible for attenuating the effect of psoriasis or visceral fat on the respective outcome variable. Thus, for psoriasis, visceral fat was significant in a univariate (Table II), but not a multivariate, model (Table III). Forward regression analysis demonstrated that IL-6 rendered the relationship between visceral fat and psoriasis non-significant (p = 0.06) (Table IV). Psoriasis was associated with MetS in a univariate (p = 0.008), but not a multivariable regression model, and this was found to be due to visceral fat, which weakened the relationship between psoriasis and MetS to non-significance (p = 0.325). Similarly, visceral fat was significantly associated with T2D in the univariate, but not in the multivariate model, and forward regression analysis showed that HOMA attenuated the association between visceral fat and T2D to non-significance (p = 0.192). The loss of the significant association of psoriasis with hypertension in the univariate model (p = 0.002) was shown to be due to visceral fat, which renders the association non-significant (p = 0.23) (Table IV). Visceral fat was a predictor of hypertriglyceridaemia (p = 0.001), low HDL (p = 0.002) and high LDL (p = 0.003) cholesterol levels in the univariate models, but did not remain significant in the multivariate models (Table IV). These relationships were attenuated to non-significance by age and adiponectin (p = 0.20), TNF (p = 0.13) and age (p = 0.16), respectively, in the forward regression analyses (Table IV).
Table IV. Variables that attenuate association of psoriasis with cardiometabolic diseases, and visceral fat with cardiometabolic diseases and psoriasis
This case-control study, in which clinical and metabolic parameters, body fat distribution and biomarkers of inflammation were measured simultaneously in a single cohort of patients with psoriasis, found that visceral fat was an independent predictor of psoriasis and that the effect of visceral fat was mediated by the pro-inflammatory cytokine IL-6. A recent study has shown evidence to suggest a causal relationship between a high BMI and psoriasis risk (24). It has also been demonstrated that visceral fat was increased in patients with psoriasis (16), and circulating IL-6 levels have been found to be elevated in psoriasis in 2 previous studies (25, 26). The mechanism by which IL-6 may contribute to the aetiology of psoriasis is not fully understood; however, it has been proposed that it may cause increased mitogenesis at the site of psoriatic skin lesions (26).
Adipokine dysregulation and the resulting inflammatory state is a central mechanism whereby visceral fat may mediate the development of various CMDs (10). The current study supports this hypothesis by demonstrating that the association of visceral fat with high triglyceride is mediated through adiponectin, whilst the association with low HDL cholesterol levels is mediated by both adiponectin and TNF. These relationships are supported by studies demonstrating that visceral fat correlates negatively with adiponectin (11), but positively with TNF levels (11), and studies showing that adiponectin is associated with lower triglyceride, but higher HDL cholesterol levels (27), whilst TNF is associated with lower HDL cholesterol levels (27). Visceral fat is also known to be associated with insulin resistance (28). This relationship was observed in the current study, with visceral fat identified as a risk factor for T2D via its effects on insulin sensitivity. This possible aetiological pathway for T2D has been reported in previous studies (29).
Psoriasis is associated with increased levels of CMDs (1). The present study also demonstrates this, and further shows that both psoriasis and PsA are independent risk factors for T2D, with none of the study variables acting as significant mediators. Previous studies have also demonstrated that T2D is more prevalent in psoriasis (30) and PsA (31, 32) compared with control subjects. Further studies are required to determine the factors that may mediate the relationship of psoriasis and PsA with T2D.
The results of the current study also show that the relationship of psoriasis with hypertension (see Table II) may be due to confounding from visceral fat (Fig. 1). Thus, in a multiple regression model for hypertension, psoriasis was not a significant risk factor for hypertension (see Table III) and forward regression analyses demonstrated that this was due to attenuation of the association of psoriasis with hypertension by visceral fat (see Table IV). These data can be interpreted either as showing that psoriasis causes visceral adiposity, which in turn leads to higher blood pressure, or that the relationship between psoriasis and hypertension is due to confounding from visceral fat. The latter hypothesis is scientifically more plausible. A similar argument can be made for the relationship observed between psoriasis and MetS (see Tables II–IV). These are important findings, as they suggest that in studies demonstrating a relationship of psoriasis with hypertension or MetS, this is not an aetiological association, but is purely a result of confounding from visceral adiposity. It is interesting to note that, in a recent meta-analysis of studies on the association of psoriasis with MetS (33) or hypertension (34), none of the studies had adjusted for visceral adiposity.
Fig. 1. Theoretical linkage between study variables based on data from multivariable regression models (outcome variables in green, input variables in blue and visceral fat in purple). Visceral fat is shown to play a central role, being linked to psoriasis via interleukin (IL)-6 and to increased triglyceride and decreased high-density lipoprotein (HDL) levels via adiponectin and tumour necrosis factor (TNF) and to type 2 diabetes via insulin resistance. Psoriasis is a risk factor for type 2 diabetes, but its relationship with high blood pressure (broken arrow) may be due to confounding from visceral fat. Ageing is associated with higher levels of low-density lipoprotein (LDL) cholesterol and total cholesterol, with Indian ethnicity also linked to higher levels of LDL cholesterol.
Triglyceride, but none of the cholesterol-related lipid species, was higher in subjects with psoriasis. Other studies have shown more atherogenic lipid profiles in those with psoriasis (35). However, in the current study, visceral fat was more strongly associated with lipid levels than was psoriasis, and these relationships were mediated through adiponectin and TNF. It is therefore possible that, in studies where psoriasis has been shown to be a risk factor for dyslipidaemia, this effect may be due to confounding from visceral fat.
Smoking and a lower education level were both associated with a higher risk of psoriasis. A high prevalence of smoking in patients with psoriasis has been observed previously (36) and in a meta-analysis the OR for psoriasis was 1.78 (95% CI 1.53–2.06) in smokers compared with non-smokers (37). Smoking may increase the risk of psoriasis by increasing oxidative stress and via nicotine, which induces the production of pro-inflammatory cytokines (38). In a cross-sectional study of 903 patients performed in France, lower education was associated with psoriasis (39) and results from a large cohort study in the USA produced similar findings (36).
This study involved the measurement of a large number of highly relevant variables, which, for the first time, allowed us to interrogate the relationships between psoriasis, visceral adiposity, adipokines and CMDs. This allowed us to develop possible mechanistic pathways for how psoriasis may lead to higher risk of CMDs, and to suggest aetiological pathways for psoriasis (see Fig. 1). Such analyses will allow future studies to take a more directed approach for determining the true aetiology of psoriasis-associated CMDs.
This study has some limitations. First, we were unable to match patients and controls for age; however, age was included in all multivariable regression models for dependent variables that correlated with age at p < 0.20 in the initial univariate model. Secondly, we were not able to assess the influence of specific drugs, such as methotrexate and acitretin, on cardiometabolic parameters (40) because of the small sample sizes. Finally, the conclusions of the current study are tempered by the cross-sectional study design and the use of multivariable regression models, which only allowed us to determine associations between variables, but do not necessarily implicate causative relationships.
In conclusion, this study demonstrates a possible role for visceral adiposity in the causation of psoriasis. It also shows that adipokines may be the mechanism through which visceral fat increases the risk of psoriasis and related CMDs. In addition, many of the CMDs that are known to be highly prevalent in subjects with psoriasis may be caused by visceral adiposity rather than by psoriasis itself. The exception is type 2 diabetes, which is strongly and independently associated with psoriasis. Future mechanistic studies should now focus on these possible aetiological pathways to determine the true molecular processes involved in the development of psoriasis-associated CMDs.
The authors would like to thank the National Health Laboratory Services and Lancet Laboratories for performing all biochemical tests, the Departments of Radiology at Charlotte Maxeke Academic Hospital and Helen Joseph Hospital for performing all CT scans, as well as all study participants.
NGM received grants from the Carnegie Corporation of New York, NY, USA (Grant Number: B 8749.RO1) the National Research Foundation (Thuthuka) and from the Astra Zeneca Research Trust. MT received a grant from the Medical Research Council (self-initiated research grant). The funding bodies had no role in the design of the study and collection, analysis, and interpretation of data, or in writing the manuscript.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize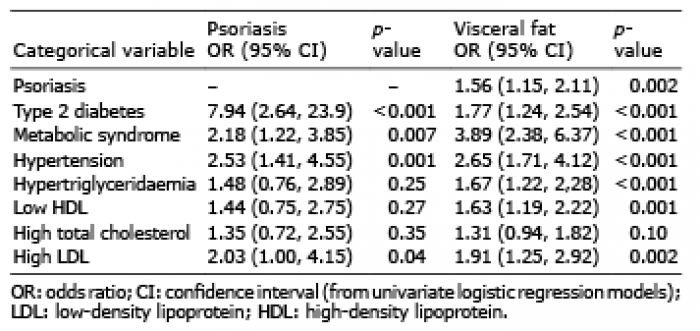 Click to show fullsize
Click to show fullsize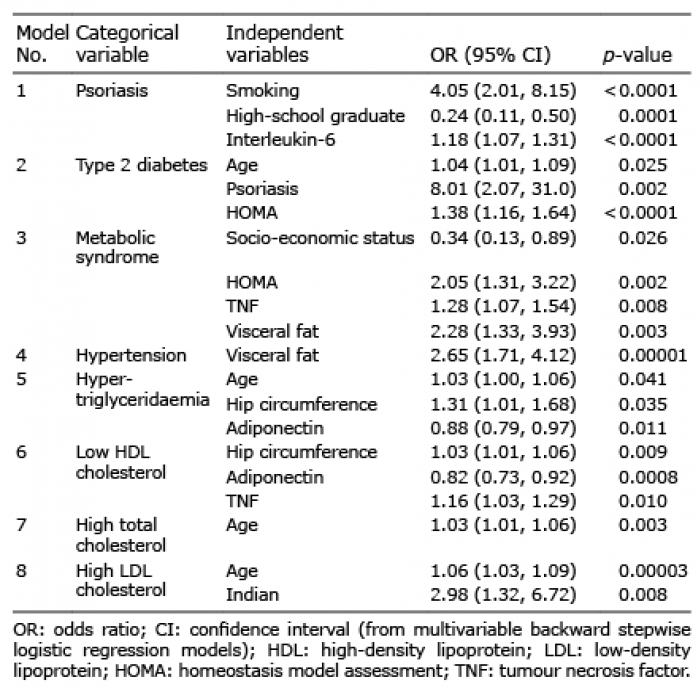 Click to show fullsize
Click to show fullsize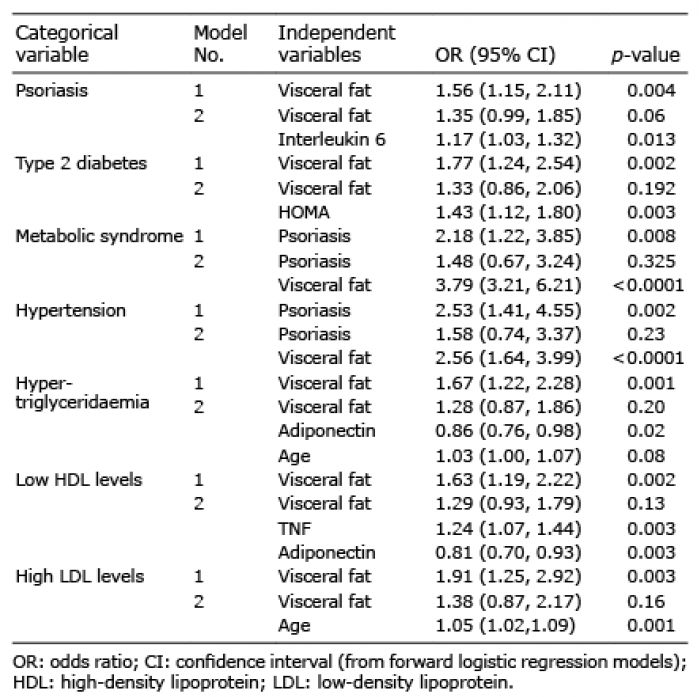 Click to show fullsize
Click to show fullsize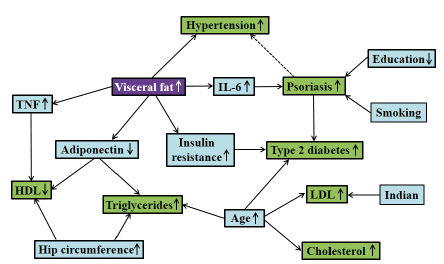 Click to show fullsize
Click to show fullsize