


Department of Dermatology, Venereology and Allergology, Wroclaw Medical University, PL-50-368 Wroclaw, Poland. E-mail: jacek.szepietowski@umed.wroc.pl
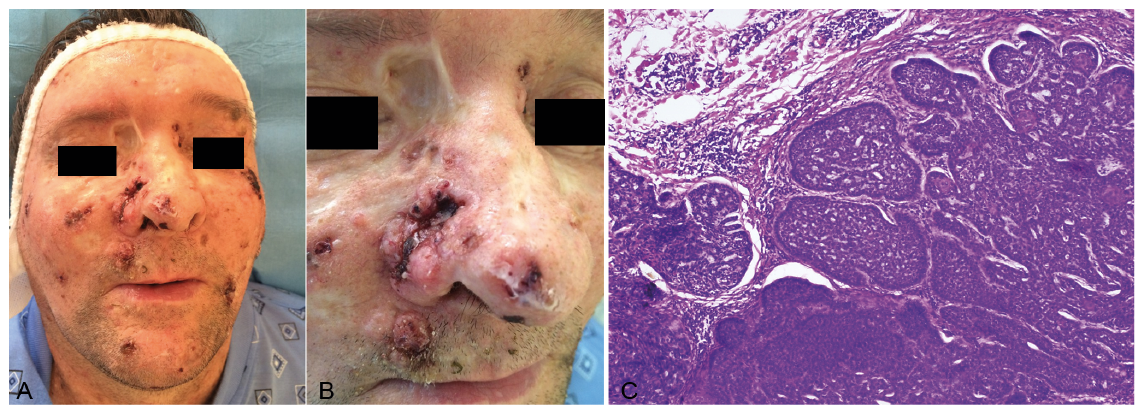
A 55-year-old, incapacitated patient was referred to the dermatosurgical unit because of multiple skin lesions. On admission, he presented with a large ulcerative lesion on both sides of the nose with pigmented and pearly boundaries. The presence of multiple small lesions on the scalp, face, neck and upper trunk was noted. The patient also presented pitted depressions on his hands, macrocephaly, high arched eyebrows, and multiple scars from previous surgeries. Closer examination revealed bitemporal flattening, frontal prominence, broad nasal bridge, highly arched palate, and dental deformations. Radiography revealed cortial and subcortical cerebral atrophy and cerebellar atrophy. The patient was additionally diagnosed with dementia, mixed polyneuropathy and motor disability. His parents confirmed no such similar cases in their family.
The first symptoms of the disease probably appeared at the age of 6 years, 2 years after a car accident in which he seemed not to suffer any serious injuries, pain or damage. His parents then started observing gradually more disturbing symptoms (“he slept more, he did not want to play with his friends, there was a noticeable delayed development compared to other children”). The car accident in the medical history probably led the neurologist to suggest the diagnosis of post-traumatic encephalitis. The boy completed 6 classes of elementary school and began studying in a special school, but there was a constant slow regression, both intellectual and motor. The patient’s mother first noticed skin lesions on the patient’s back when he was approximately 12 years old. The first skin lesion was treated in our unit when the patient was 50 years old and had already become incapacitated.
After the first surgical procedure the patient was admitted for repeat procedures approximately every 3 months. During the previous few months the number of skin lesions had increased rapidly (Fig. 1A, B). When first admitted to the surgical ward he presented with moderate intellectual disability; however, at the age of 55 years he presented with an IQ of 20–34 and a significant degree of intellectual disability.
Histological examination of 3 biopsy specimens showed well-defined collections of basophilic basaloid cells, with peripheral palisades and adjacent stromal retraction with gap formations (Fig. 1C).
What is your diagnosis? See next page for answer.
Fig. 1. (A) Multiple tumours on the face. (B) Ulceration on the nose. (C) Histological features of basal cell carcinoma (haematoxylin and eosin; H&E ×100).
Acta Derm Venereol 2020; 100: XX–XX.
Diagnosis: Gorlin–Goltz syndrome (The 5th phacomatosis, multiple basal cell carcinoma syndrome, basal cell naevus syndrome)
The patient was diagnosed as having Gorlin–Goltz syndrome (GGS) (firstly reported in 1894 by Gorlin and Goltz) with numerous basal cell carcinomas (BCCs) and falx cerebri calcifications, mandibular keratocystic odontogenic tumours (KOT) confirmed on histology, pitted depression on the hands and ectopic calcifications, which are among the major criteria, and macrocephaly, hypertelorism, and presence of skeletal and radiological abnormalities, which are among the minor criteria, at the age of 50 years. The clinical, radiological and histopathological findings met criteria for diagnosis of GGS (Table I).
Basal cell naevus syndrome (BCNS) represents a series of multi-organ abnormalities known to be the consequence of mutations in the sonic hedgehog signalling pathway. The syndrome’s gene has been mapped to chromosome 9q23.1–q31, a tumour suppressor gene. The mutations are inherited with a very different expression, approximately 35–50% of the patients show a de novo mutation with negative family history.
The prevalence is 1:60,000, with an equal frequency in women and men (1). Overall, the classical triad is composed of multiple BCCs, KOT and bifid ribs. Clinical and radiological diagnostic criteria were proposed by Evans et al. (2) and modified by Kimonis et al. (3) (Table I). The BCNS is diagnosed based on meeting either 2 major criteria, or 1 major and 2 minor criteria. The treatment of multiple BCCs includes conventional surgery, Mohs micrographic surgery, cryotherapy, laser ablation, photodynamic therapy, imiquimod 5% cream, 5-fluorouracil cream, and the sonic hedgehog pathway inhibitor vismodegib (4).
When first admitted to the surgical ward with an uncounted number of BCC, the patient was already retired. Most patients develop multiple BCCs in adolescence, which should raise the suspicion of GGS. Due to difficulties in communication connected with significant intellectual disability, we do not know when the first skin plaques appeared. There is also a possibility that, because of the coincidental car accident, an erroneous cause of developing encephalitis was diagnosed, which delayed correct diagnosis.
In a patient with BCC, when surgery is deemed the first line of treatment, the goal should be to excise the entire lesion while sparing healthy tissue and, when needed, to use reconstructive surgery in order to maintain form and function. Therapy with vismodegib (4) may be an alternative to frequent, repetitive, and scarring surgical procedures but, due to financial reasons, use of this drug is limited in some countries.
In addition to treating existing BCC lesions, an important aspect of the management of GGS is the prevention of new lesions. Patients with GGS should be counselled regarding excessive sun exposure and the use of protective sunglasses, clothing and high-factor sunscreens. Clinicians should be aware that patients with GGS face difficulties, not only due to the manifestations of their syndrome, but also because of the treatment, which may result in cosmetic and/or func-tional deficits. Clear communication should exist between the different physicians managing different aspects of the patient’s complex and challenging disease.
Table I. Diagnostic criteria for Gorlin–Goltz syndrome in the current patient (based on Kimonis et al. (1))
The authors acknowledge Dr Zdzis?aw Wo?niak from the Department of Pathology of Wroclaw Medical University for his help in histopathological analysis and providing a histopathological illustration.


 Click to show fullsize
Click to show fullsize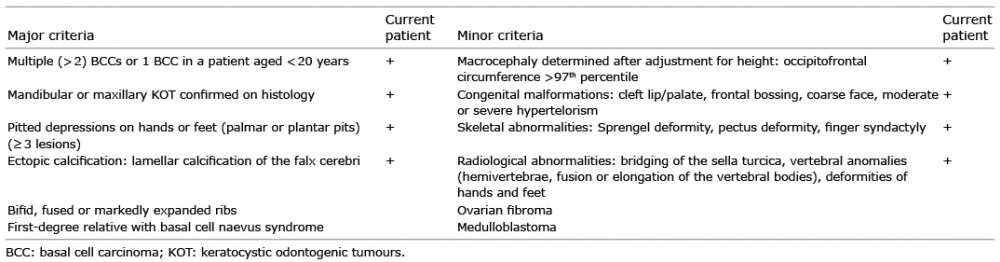 Click to show fullsize
Click to show fullsize