


1Dermatology Department, and 2Anatomopathology Department, Saint-Louis Hospital, 1 avenue Claude Vellefaux, 75745 Paris cedex 10, France. *E-mail: jean-david.bouaziz@aphp.fr
Accepted Oct 3, 2019; E-published Oct 3, 2019
Systemic lupus erythematosus (SLE) is a prototypic autoimmune disease characterized by heterogeneous clinical and serological manifestations that may affect any organ (1). Cutaneous lupus erythematosus (CLE) is an autoimmune disorder occurring independently of or as a manifestation of SLE, including acute cutaneous lupus erythematosus, subacute cutaneous lupus, and chronic cutaneous lupus erythematosus (discoid lupus erythematosus, lupus erythematosus profundus, chilblain cutaneous lupus, and lupus tumidus) (2). The prevalence of vasculitis in SLE is reported to be between 11% and 36%, with a diverse clinical spectrum due to inflammatory involvement of vessels of all sizes (3). Pseudo-erysipelas (PE) is a cutaneous manifestation seen in periodic fever syndromes, presenting as erythematous and swollen extremities. We report the case of a man who developed a PE concomitant with an acute SLE flare.
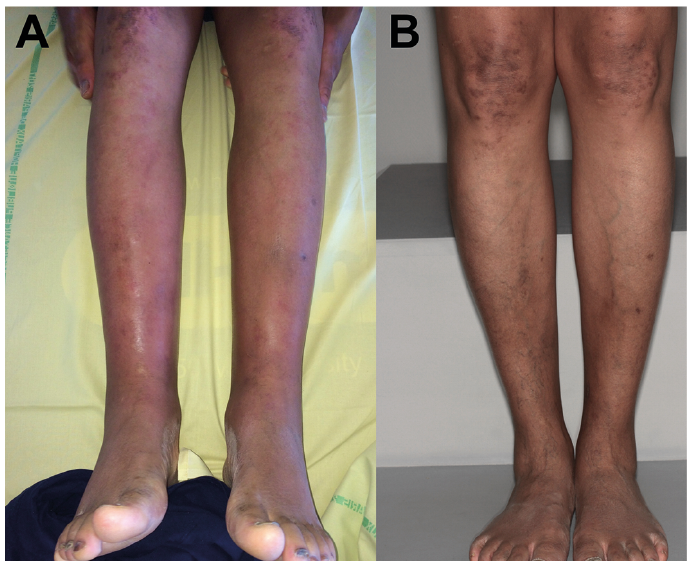
A 42-year-old Guyanese man, diagnosed 12 years ago with cutaneous, articular and cardiac SLE, who was not currently undergoing treatment, presented with a 38.5°C fever and symmetrical, painful swelling and thickening of both legs (Fig. 1A), associated with infiltrated erythematosus annular lesions of the trunk, back and face, and atrophic hyperpigmented keratotic lesions of the face, ears and elbows. Routine biological tests revealed anaemia (10.3 g/dl), neutropenia (1.01 × 109 G/l), lymphopenia (1.05 ×109 G/l), and negative CRP (3 mg/l, normal range < 5 mg/l). Immunological tests revealed positivity for anti-nuclear antibodies (1/1,600), anti-RNP, anti-Sm, anti-SSA, and anti-P ribosomes. The C3 and C4 complement levels were normal. Urine tests revealed proteinuria (1.3 g/day). A deep biopsy taken from the left leg showed a dermo-hypodermal lymphocytic infiltrate. It involved and surrounded the walls of small and medium-sized vessels with fibrin deposits in some of them (Fig. 2). Two other biopsies taken from the back and the left arm showed dermal lymphocytic infiltrates with interface dermatitis and mucin deposits in favour of lupus erythematosus. Renal biopsy showed class II and V lupus nephritis. Treatment with hydroxychloroquine and 3-day intravenous injections of 500 mg of methylprednisolone was started, followed by oral prednisone 1 mg/kg/day for one month, which was associated with the complete remission of the skin lesions and systemic symptoms (Fig. 1B). Methotrexate (20 mg) once a week was started as a background treatment for SLE. Progressive tapering of steroids was performed with favourable clinical evolution during the 6-month follow-up.
Fig. 1. Symmetrical, painful, swelling and thickening of both legs (A). Complete remission after steroid treatment (B).
Fig. 2. Dermo-hypodermal lymphocytic infiltrate surrounding the walls of small and medium-sized vessels with fibrin deposits in some of them.
The originality of this case comes from the association of PE and the SLE flare. This is, to the best of our knowledge, the first case of this atypical cutaneous manifestation in a patient with SLE. There have been several reports of soft-tissue pneumococcal infections in SLE patients (4). The histologic features and a complete response to corticosteroid treatment do not suggest an infectious cause in our case. A previous patient with SLE and oedematous soft tissue involvement of the legs has already been reported (5). In the previously reported case, the occurrence of the swellings did not correlate with lupus activity, and the histology showed mild superficial dermal perivascular infiltrate but no vasculitis.
The differential diagnosis of “erysipelas-like” lesions may be familial Mediterranean fever (FMF), tumour necrosis factor receptor-associated periodic syndrome, Shulman fasciitis at its initial inflammatory stage, and inflammatory lipodermatosclerosis.
The histology of PE in FMF reveals a predominant polymorphonuclear infiltrate with pronounced dermal oedema. In FMF, histological findings show a nonspecific perivascular inflammatory infiltrate. Skin vasculitis is commonly described in SLE with various clinical presentations: palpable purpura, cutaneous infarction, livedo reticularis, papulonodular lesions, erythematous plaques, panniculitis, splinter haemorrhages, and superficial ulcerations (3, 6, 7). We describe an original case of lupus vasculitis presenting as PE. A deep skin histology in patients with erysipelas manifestations in the setting of SLE that do not respond to antibiotic treatment should be discussed.


 Click to show fullsize
Click to show fullsize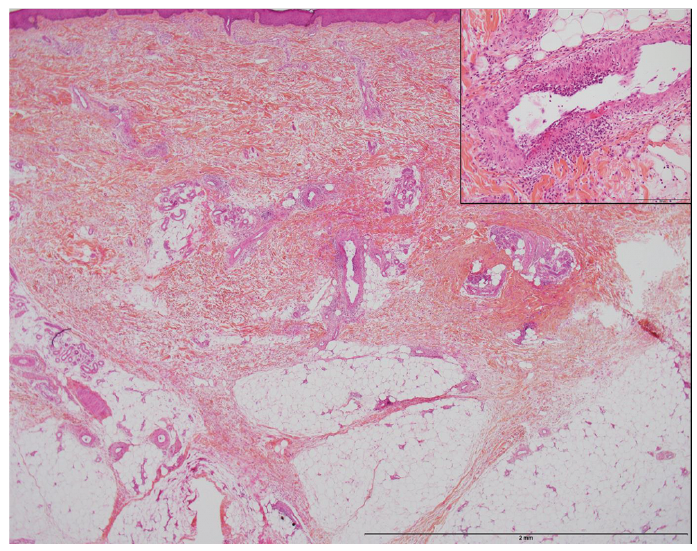 Click to show fullsize
Click to show fullsize