


1Department of Plastic and Reconstructive Surgery, San Gallicano Dermatological Institute, IRCCS, and 2Department of Maxillofacial Surgery, San Camillo-Forlanini Hospital, Rome, Italy
Skin malignancies of the head and neck inflict significant structural, functional, and cosmetic burdens upon those affected. We retrospectively addressed electrochemotherapy anti-tumour efficacy in head and neck skin cancer patients who were not suitable for standard treatments. Scars’ physical characteristics and aesthetics were evaluated using validated scar assessment scales. Among 33 treated patients, 82% experienced a complete tumour response while 18% experienced a partial response. At a median time period of 7 months, 96% of the evaluated scars came close to resembling the normal surrounding skin showing excellent results in terms of restoration to original condition with no deformity and/or distortion and in terms of preservation of functionality, such as oral competence and eye protection. Electrochemotherapy is an effective local anticancer procedure for cutaneous tumours. In the treatment of skin malignancies of the head and neck, especially in non-surgical cases, in the elderly and in patients declining surgery, electrochemotherapy may represent a valid alternative to standard management.
Key words: electrochemotherapy; head and neck skin cancer; quality of life; aesthetics; cosmetic outcome; scar assessment scale.
Accepted Oct 14, 2019; E-published Oct 14, 2019
Acta Derm Venereol
Corr: Antonio Bonadies. Department of Plastic and Reconstructive Surgery, San Gallicano Dermatological Institute, IRCCS, Via Elio Chianesi, 53, IT-00144 Rome, Italy. E-mail: antonio.bonadies@ifo.gov.it
The main goal of skin cancer treatments is to eradicate the tumour with the safest method providing an aesthetically and functionally pleasant outcome. Electrochemotherapy is a minimal-invasive local tumour ablation procedure for cutaneous metastases. This study found that in head and neck skin cancer patients treated with electrochemotherapy, after tumour clearance and wound healing, most of the assessed scars showed physical and aesthetic characteristics very similar to those of normal surrounding area. These results suggest that in the management of head and neck skin cancer, electrochemotherapy may represent a valid alternative to traditional techniques when such techniques are not suitable.
Skin malignancies (SM) of the head and neck (HN) area inflict significant structural, functional, and cosmetic burdens upon those affected. Surgical excision is the most common method of treatment for SM of the HN. The main objectives of anticancer treatments are the total removal of the tumour and patient survival, yet the patient’s func-tionality and self-esteem preservation are becoming such that they are starting to be considered as essential goals.
Electrochemotherapy (ECT) is a safe, well established, local tumour ablation procedure that is effective on solid tumours (1, 2). It combines the local application of electric pulses (electropermeabilization) and low dosage chemotherapy in order to facilitate the delivery into the tumour cell of otherwise non-permeant anticancer drugs thus leading to a dramatic increase in local cytotoxicity (3). ECT has proven highly effective for the treatment of cutaneous and subcutaneous tumours, regardless of their histological origin (4, 5). ECT also has an effect on the control of bleeding due to metastatic tumour deposits and mass-related symptoms (6).
An increasing number of studies have provided evidence for the efficacy of ECT in various types of skin tumours located in the head and neck region. Treatment with ECT is suitable in advanced primary or recurrent or metastatic basal cell carcinoma (BCC), squamous cell carcinoma and in cutaneous metastases of melanoma of the head and neck. (7–9). It is effective in previously irradiated areas where chemo-radiation protocols can be inapplicable (10, 11). Because of its selectivity towards dividing tumour cells, when treating safety margins to decrease the risk of recurrence, it spares normal healthy tissue that surround the tumour and preserves organ functions (12, 13). This is particularly important in BCC with ill-defined borders and when treating skin tumours of central facial areas where extensive surgery can be disfiguring and where there is a high risk of recurrence after excision (14–16). Moreover in the local management of extensive metastatic cutaneous melanoma lesions, the application of repeated sessions of ECT can help to avoid the administration of invasive and/or systemic, more debilitating treatments especially in frail elderly patients with comorbidities (17) and allows, in selected cases, for combinations with immunotherapy protocols (18, 19).
Our 10-year experience in the management of melanoma and non-melanoma skin cancer with ECT, has allowed us to identify thoroughly-selected HN patients who could benefit from ECT with respect to the cosmetic aspect and patients’ functioning as opposed to an invasive, less favourable surgical treatment.
The objective of our retrospective study was to address ECT antitumor efficacy and organ preservation along with the achievement of an acceptable aesthetic outcome in the management of SM in the HN area.
Patient selection
This study was retrospective. All procedures performed in this study were approved and in accordance with the ethical standards on human experimentation of the institutional and/or national research committee and with the Helsinki declaration of 1975, as revised in 1983. Informed consent was obtained from all individual participants included in the study. Patient selection was based on the European Standard Operating Procedures on Electrochemotherapy (ESOPE) guidelines. Patients had a life expectancy longer than 6 months and measurable cutaneous or mucosal tumour lesions. Eligible patients were all patients affected by recurrent, metastatic or primary cancer of the HN area, who were not suitable for surgery or other standard therapies because of their poor general condition, age, comorbidities or predicted negative outcome of invasive, radical surgical intervention with a high risk of major intra-postoperative complications (functional impairments and/or poor cosmetic results, risk of prolonged anaesthesia, massive bleeding). The histological characteristics of the different subtypes of tumour were assessed. Exclusion criteria included clinically manifested arrhythmia or an in-place pacemaker, interstitial lung fibrosis, epilepsy, an active infection, a known allergy to bleomycin, kidney failure or previous treatment with bleomycin at the maximum cumulative dosage.
Electrochemotherapy procedure
In all cases, the treatment was performed according to the ESOPE guidelines (3), under general anaesthesia. Briefly, bleomycin (Nippon-Kayaku, Sanofi-Aventis) was administrated intravenously at the dose of 15,000 UI/m2. Electric pulses were applied to the tumour area 8 to 28 min after the bleomycin injection to allow for the homogeneous distribution of the injected drug into the tumour. Electric pulses (8 pulses of 100 ms duration) were delivered using a square wave pulse generator (Cliniporator, IGEA spa, Carpi, Italy).
Response evaluation
The tumour volume of target lesions was calculated and locoregional response to treatment was evaluated two months after treatment. In accordance with the Response Evaluation Criteria in Solid Tumours (RECIST version 1.0), modified to include the response of only the treated cutaneous lesions, a maximum of 7 cutaneous lesions per patient were registered as target lesions, as in previous studies (3, 7). The longest diameter of the tumours was measured and recorded, and photographs were taken at the time of treatment and during subsequent follow-up visits.
Postoperative evaluation
Patients had follow-up visits at one-week intervals during the first 6 weeks and thereafter at monthly intervals. Adverse events and side-effects were rated according to the CTCAE, version 4.02.
Aesthetic and scar clinical assessment
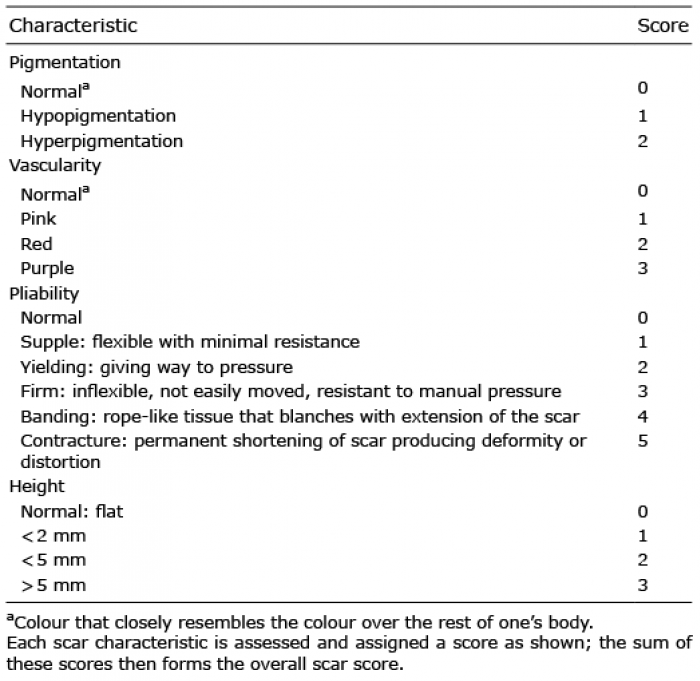
Post ECT evaluation of wound healing and scars’ appearance were assessed independently by 3 observers (one plastic surgeon and two research associates), using the Vancouver Scar Scale (VSS) (20) and the Manchester Scar Scale (21) in complete response patients by photographic analysis (22). The MSS also includes a Visual Analogue Scale of 0–100 (Excellent–Poor) which describes the overall cosmetic scar appearance, evaluated by an external observer (Tables I and II).
Table I. The Vancouver Scar Scale
Table II. The Manchester Scar Scale
Statistical analysis
Categorical variables have been reported as frequency number and percentages. Continuous variables have been expressed in terms of median value and range (minimum and maximum). For survival analysis. Kaplan Meier analysis was applied and local progression free survival was defined for all patients as the time between the first ECT session and local progression of the nodules inside the treated area. Kaplan Meier test was used to assess 1-year survival with 95% confidence interval. Chi-square test was performed to estimate statistically significant difference between percentage values in different population subgroups. p-value < 0.05 was considered significant.
Internal consistency was defined as “the homogeneity of a set of categories and the degree to which they all share the same characteristics.” It was assessed by using Cronbach’s alpha statistics which considered values ≥ 0.70 to be acceptable (23).
Study cohort
From May 2008 to December 2017, 312 patients with cutaneous melanoma metastases and non-melanoma tumours underwent ECT at the Plastic Surgery Department of the San Gallicano Dermatologic Institute in Rome. Among all patients treated, 33 were retrospectively included in our study, because the tumours were located in the HN area, in regions of relevant aesthetic and functional impact; in these patients first line treatments such as surgery and radiotherapy were ill-advised due to their being too invasive and/or destructive (Table III). Descriptive demographic data of the included patients are shown in Table IV. Twelve patients (36%) had one single lesion on their HN area, whilst 21 (64%) were treated for multiple lesions around their face, scalp, and neck. For this reason, in some cases, different regions of the HN were treated on the same patient. The distribution of the tumour nodules according to the different anatomical HN sub-sites is reported in Fig. 1.
Table III. Study cohort
Table IV. Patients’ characteristics and treatment details
Fig. 1. Distribution of the treated tumour nodules according to the different head and neck sub-anatomical areas.
Overall, 17 patients (52%) received more than one ECT session to treat the disease in order to obtain the best result. Treatment details and reasons for re-treatment are reported in Table IV. Median time between first and second treatment was 7.3 months (range 2.1–36.1). Median time between the second and the third treatment was 6.2 months (range 3.0–25.8).
Toxicity
In 8 patients (24%), during the first 30 days after ECT treatment, a necrotic area appeared and spontaneously resolved itself 1–2 months following treatment. Six patients (18%) suffered an oedema in the treated area during the first two weeks after treatment. All side effects were easily managed and resolved themselves naturally.
Response to treatment
All patients responded to treatment. After two months following ECT treatment, 27 patients (82%) showed a complete response (CR) while 6 patients (18%) showed a partial response (PR). Response rates according to tumour histological type are reported in Table V. When considering the 12 patients with a single lesion, a CR rate of 100% was achieved whereas in patients with multiple lesions (21 patients), a CR rate of 71% and a PR rate of 29% were obtained
Local control of the disease was maintained for a median time of 9.5 months (range 0.3–52.7 months). The local progression-free survival curve is shown in Fig. 2. One-year local progression-free survival was 82% (C.I.95% 64–100%) (Table V).
Table V. Efficacy summary (n = 33) and tumour control
Fig. 2. Local control on electroporated tumours over time. Kaplan–Meier local progression-free survival.
Aesthetic outcome
The aesthetic result was evaluated on photographic records and assed by 3 independent observers using VSS and MSS in 26 complete response patients. One complete response patient was not evaluable using the scar scales. Values are reported in Table VI. The VSS total scores show that 25 out of 26 patients achieved a score of 4 or less (mean total score 1.6), indicating scars that almost resemble normal skin (Fig. 3a). MSS outcomes strengthened the VSS results showing a score of 10 or less (mean total score 7.7) in most patients (25/26) confirming how the scars are nearly comparable with normal skin (Fig. 3b). The VAS used along with the MSS well-represented the satisfying maturation process of the evaluated skin scars showing a score of 36 or less (mean total score 22) in 22 out of 26 patients (85%) (Fig. 3c).
Internal consistency
The internal consistency was acceptable for the VSS and the MSS with Cronbach’s alpha values of 0.74 and 0.75, respectively.
Table VI. Scar scales’ results. Evaluated patients n = 26
Fig. 3. Aesthetic outcome of 26/27 patients with complete response. One complete response patient was not evaluable using the scar scales. (A) Graph illustrating the Vancouver Scar Scale total score for each patient. (B) Graph illustrating the Manchester Scar Scale total score for each patient. (C) Graph illustrating the Visual Analog Scale score for each patient.
ECT represents a novel therapeutic alternative to surgical resection and/or radiotherapy in unresectable HN skin cancer (7). In this study, we present the results obtained in our series (n = 33) of malignant melanoma metastases and non-melanoma skin cancers of the HN area treated with ECT. Our findings confirm that ECT provides a degree of local control in the HN cancer in accordance with previous experiences (7, 8,12–16). ECT achieved an overall response in all patients with a complete response rate of 82%, a low toxicity profile and no severe side effects. All treatments were performed with a short operating time and were well-tolerated with minimal hospitalization, low grade systemic (fever, exhaustion) and local side effects (oedema, erythema, pigmentation, pain). Deep ulceration was occasionally observed but always managed at home by the patient until healing. Around 50% of patients underwent a single ECT session achieving a CR and of those who underwent multiple sessions, more than half were retreated for new locoregional lesions outside the treated area or for new distant lesions at the limbs or in the trunk area.
Recent studies have shown 100% CR in patients after ECT classical Kaposi sarcoma (KS) of the limbs (24–26). Facial KS, however, is radiosensitive and can be well controlled with low-dose radiotherapy. The subset of 6 patients, 4 with classical KS and 2 patients with HIV-associated KS, in our study prove in principle that ECT represents an effective alternative to treat facial KS. All treated lesions achieved a CR. ECT was well tolerated: two patients suffered from oedema in the treated area (lower and upper eyelids) during the first two weeks after treatment, but no additional local or systemic toxicities were observed.
The secondary aim of the present study was to assess the cosmetic outcome in patients with skin malignancies of the HN area following ECT treatment. Our cohort comes from a specific selection of patients carried out in a plastic surgery department that is specialized in the treatment of skin tumours. In accordance with protocol and standard procedure, the selected patients underwent ECT because they were affected with advanced primary or recurrent or metastatic cutaneous lesions which were ineligible for systemic therapies, or untreatable with surgery due to the patients’ co-morbidities or to disease-associated characteristics such as a high number of lesions and/or their location. As for patients with multiple lesions, several necessary surgical interventions would have resulted in heavy scarring.
To date, this is the first investigation to measure physical and aesthetic characteristics of the skin post ECT treatment. Skin tissue repair after invasive surgical or non-surgical procedures can result in a broad spectrum of skin conditions ranging from normality, resembling, i.e., the rest of one’s body, to a variety of abnormal and pathological scars. In our work, we have decided to evaluate thickness, contour, vascularity, pigmentation and pliability because they are all crucial factors for the maintenance of mechanical and physiological functionality leading, in the case of alteration, to disabling problems such as loss of motion and to cosmetic defects, for example scar distortion and shiny skin surfaces. Therefore, in 26 complete response patients, after the wounds had healed, at a median time of 7 months (range 4–16) following ECT of the treated skin area, formerly occupied by the tumour, was evaluated using two widely used rating scales for scars: VSS and MSS (20–22, 27, 28). First of all, in assessing head and neck post ECT skin scars by using subjective methods, both VSS and MSS had acceptable internal consistency. This indicated that both VSS and MSS presented a good degree of feasibility as a scar assessment tool for clinical follow-up in the skin scar evaluation of our cohort of patients. The reliability of VSS for skin scars following ECT (0.74) was similar to facial skin graft scars as previously reported (0.76) (29). Altogether, our results revealed that most of the assessed scars were considered very similar to the surrounding skin. The mean VSS total score achieved per patient was 1.6 (Table VI) with normal to moderate vascularity, good pliability (scar elasticity) without banding or contracture, no to mildly-decreased pigmentation and with height (scar thickness) sometimes slightly above the skin surface. MSS was developed to assess scars from surgical excision and focuses on the scar’s cosmetic appearance. The MSS findings confirmed our VSS outcomes; the mean total score obtained was 7.7 associated in most patients with a matte-like appearance, a perfect to slightly mismatched colour, a good relationship with the surrounding skin with a flush or slightly proud contour and a normal to just palpable texture (Table VI). In our experience, with specific regards to the most difficult aesthetic units of the face area such as the eyelids and the palpebral fissure, the auricle, the nasal ala and the lower lip, ECT has produced surprisingly excellent results in terms of restoration to original condition (restitutio ad integrum), with no deformity or distortion and in terms of preservation of functionality like oral competence and eye protection (Fig. 4).
Fig. 4. (A) Squamous cellular carcinoma in a patient treated with ECT; cutaneous lesion of the left auricle at baseline (left); large scab observed 15 days after ECT treatment (center); complete response of the treated lesion. The patient was disease-free at the last clinical examination 6 months after treatment with a positive functional and cosmetic outcome (right). (B) Young, HIV+, Kaposi sarcoma patient treated with ECT; Kaposi sarcoma lesion of the right lower eyelid at baseline (left); swollen area with oedema 15 days after treatment (centre); complete response of the treated lesion showing a positive functional and cosmetic outcome at 6 months after ECT (right). (C) Squamous cellular carcinoma in an elderly patient treated with ECT; extensive lesion involving most of the lower lip at baseline (left); large scab observed 15 days after ECT treatment (center); complete response of the treated lesion. The patient was disease-free at the last clinical examination 12 months after treatment with a positive functional and cosmetic outcome (right).
Interestingly, the age of the patients in our cohort is heterogeneous, some of the patients at the time of ECT were elderly suffering from comorbidities therefore un-able to undergo a long and risky surgical operation while others, much younger and with less sever comorbidities, valued aesthetics and had poor acceptance of possible surgical destructive outcomes. Compatible with this last observation Martin and colleagues (30) reported that patients with localized resectable BCC particularly appreciate cure and cosmetic outcome and consider less important the treatment procedure indicating that participants are willing to accept different surgical and non-surgical approaches in order to optimize chances of cure and favorable appearance.
In conclusion, a growing amount of data, now including our study, is showing that ECT is an effective local treatment for cutaneous cancer of any histological origin. Our new findings seem to suggest that in the management of HN skin malignancies, ECT allows for an acceptable aesthetic and functional result to be achieved and may be considered a valid alternative to traditional surgical techniques when such techniques are not suitable. The present investigation has a number of limitations, it was carried out in a single centre, the patient cohort was small, and the study was conducted as a single-arm non-comparative investigation with a short follow-up time. In order to define the recurrence rate after ECT on non-resectable HN skin tumours, a longer observation period, e.g. 5 years, is required. These data will eventually help optimizing the indication for ECT in the treatment armamentarium against aggressive and/or non-resectable HN skin cancer. Nevertheless, our results are promising and should encourage the planning of future randomized trials with a head to head comparison to standard treatments to further establish the role of ECT in HN cancer.


 Click to show fullsize
Click to show fullsize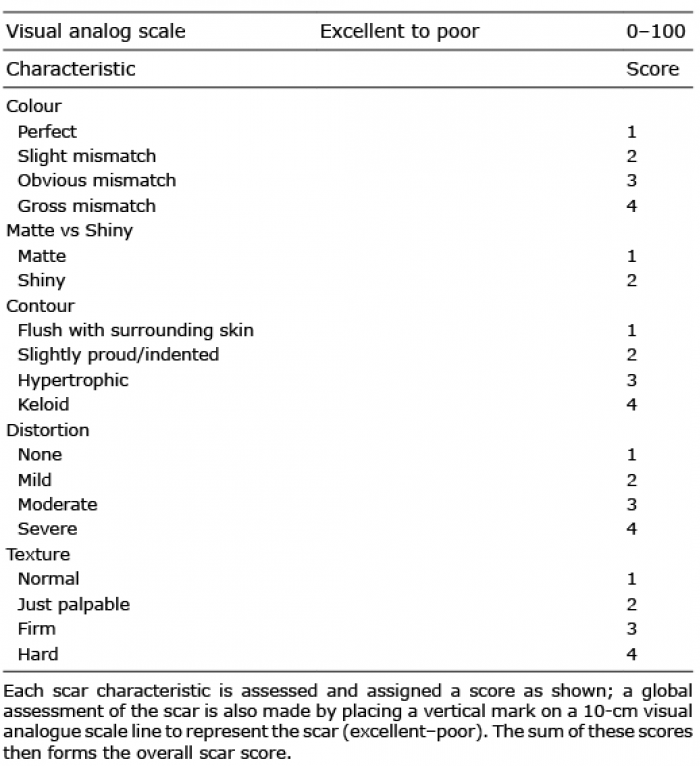 Click to show fullsize
Click to show fullsize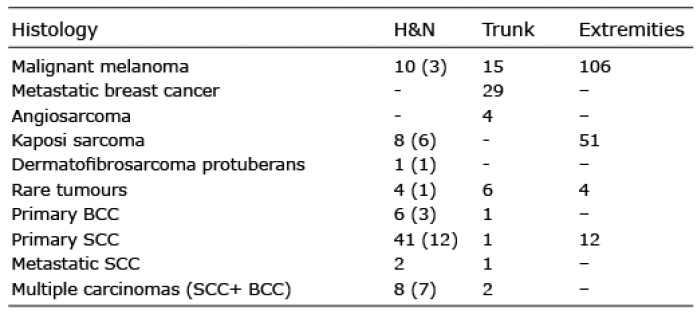 Click to show fullsize
Click to show fullsize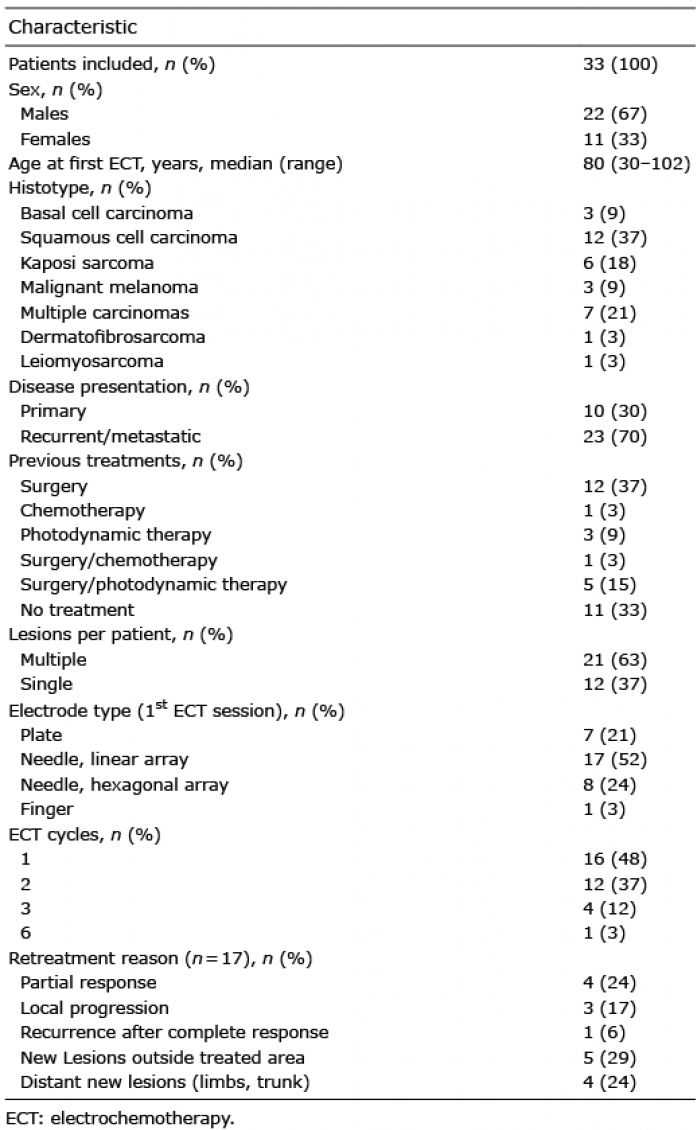 Click to show fullsize
Click to show fullsize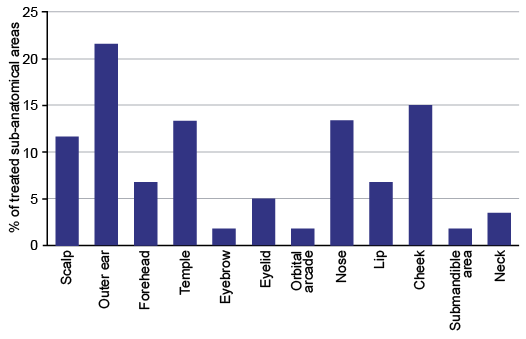 Click to show fullsize
Click to show fullsize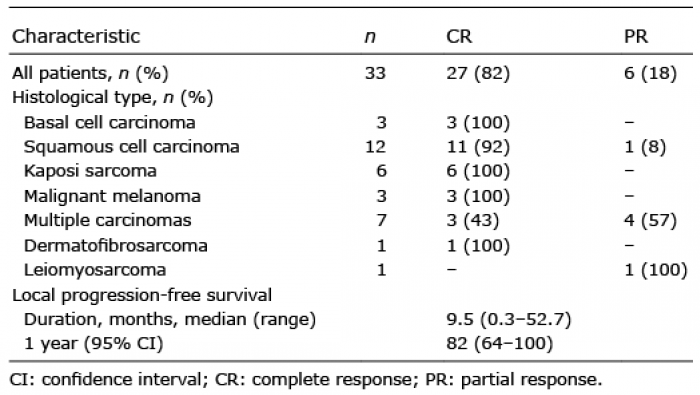 Click to show fullsize
Click to show fullsize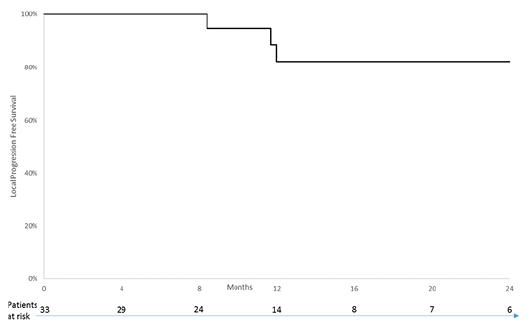 Click to show fullsize
Click to show fullsize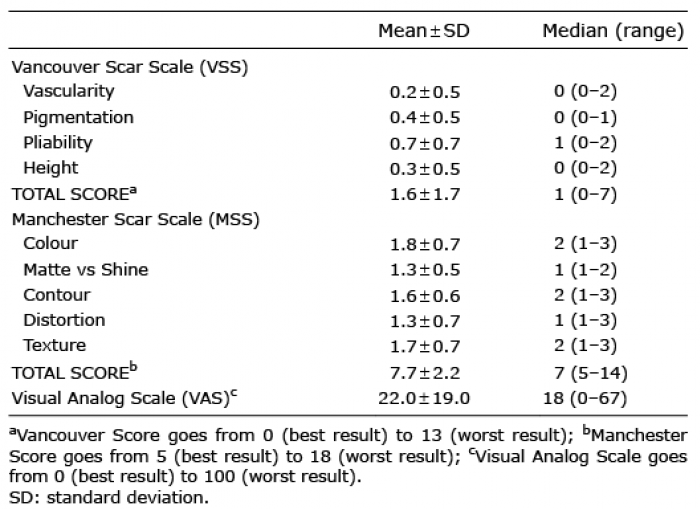 Click to show fullsize
Click to show fullsize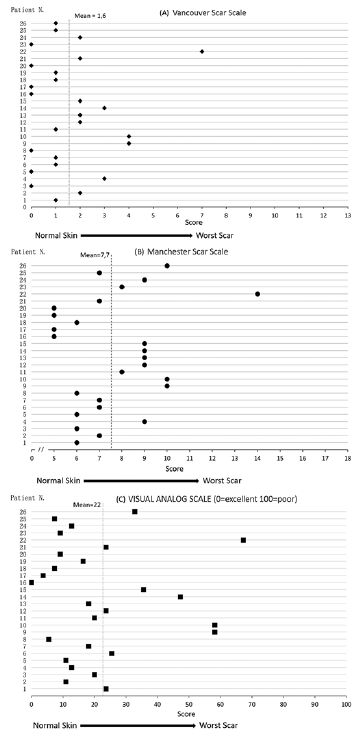 Click to show fullsize
Click to show fullsize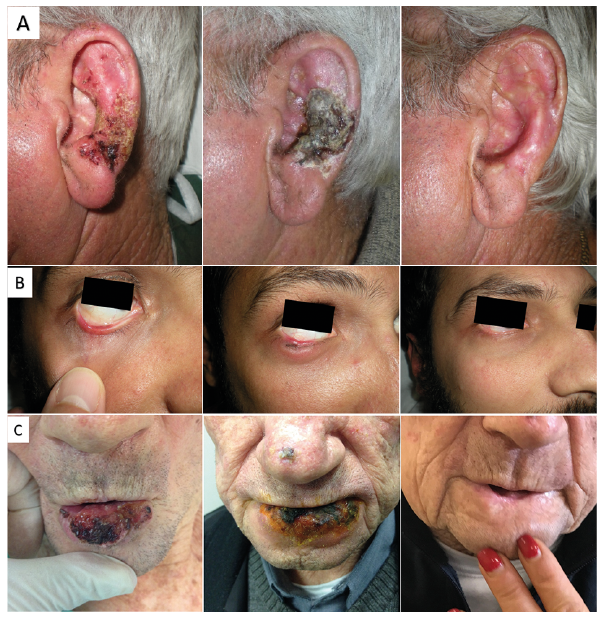 Click to show fullsize
Click to show fullsize