


1Department of Dermatology, Venereology and Allergology, University Medical Center, Ruprecht-Karls-University Heidelberg, Heidelberg, 2Dermatopathology, Bodensee, Friedrichshafen, Germany, 3Sikl’s Department of Pathology, Medical Faculty in Pilsen, Charles University in Prague, Pilsen, Czech Republic, 4Department of Dermatology, University Hospital of the Paracelsus Medical University Salzburg, Salzburg, Austria, and 5Center for Dermatopathology Freiburg, Freiburg, Germany
To shed more light on the pathogenesis of sebaceous carcinoma, we analysed the expression of proteins related to angiogenesis in 18 ocular and 22 extraocular sebaceous carcinomas using a broad panel of immunohistochemical markers. To quantify the expression of D2-40, vascular endothelial growth factor, vascular endothelial growth factor receptor-2 and -3, we calculated a quantification score by considering the percentage of positive tumour cells (0=0%, 1=up to 1%, 2=2–10%, 3=11–50%, and 4=>50%) in relation to the staining intensity (0=negative, 1=low, 2=medium, and 3=strong). Additionally, lymphatic microvessel density in the D2-40 stained sections was counted. Vascular endothelial growth factor receptor-3 (quantification score 9.42 ± 2.94) was significantly more strongly expressed than vascular endothelial growth factor receptor-2 (quantification score 2.15 ± 2.42, p < 0.001). Furthermore, epidermal vascular endothelial growth factor expression was negatively correlated with the intratumoural lymphatic vessel density, and the ratio of small lymphatics to large lymphatics was much higher in intratumoural tissue than in paratumoural tissue and in intraindividual control tissue, suggesting a lymphangiogenetic potential of sebaceous carcinoma.
Key words: angiogenesis; lymphatic vessels; sebaceous carcinoma.
Accepted Oct 14, 2019; E-published Oct 14, 2019
Acta Derm Venereol
Corr: Ferdinand Toberer, Department of Dermatology, Venereology and Allergology, University Medical Center, Ruprecht-Karls-University, Im Neuenheimer Feld 440, DE-69120 Heidelberg, Germany. E-mail: ferdinand.toberer@med.uni-heidelberg.de
Sebaceous carcinoma represents a rare cutaneous tumour that may arise ocular and extraocular. We analysed the expression of proteins related to angiogenesis in 18 ocular and 22 extraocular sebaceous carcinomas using a broad panel of immunohistochemical markers including D2-40, vascular endothelial growth factor (VEGF), VEGFR-2 and VEGFR-3. We found an increased intratumoural ratio of small lymphatics to large lymphatics and a negative correlation between epidermal VEGF expression and the intratumoural density of lymphatics underlining the hypothesis that sebaceous carcinoma may induce new lymphatic vessels. Additionally, VEGFR-3 expression was significantly higher than VEGFR-2 expression in both ocular and extraocular tumours.
Sebaceous carcinoma (SC) represents a rare cutaneous adnexal neoplasm that may arise as ocular or extraocular SC (1). Extraocular SC is rare (25% of reported cases) and mostly affects the head and neck (2). According to a review including 1,349 cases of SC, the median age at diagnosis was 73 years, and a slight male predominance (54% men and 46% women) was noted (3). Both ocular and extraocular SC have the capability for regional and distant metastases (4). The tendency for regional metastases is increased in ocular SC. Nevertheless, the cancer-specific mortality rates are similar among all anatomic locations (4). Although surgery is the treatment of choice for local disease, radiation and systemic chemotherapy are options for recurrent and metastatic disease (4).
SC may arise in the context of Muir-Torre syndrome (MTS) or in association with prior irradiation, immuno-suppression and familial retinoblastoma (4). Nonetheless, the pathogenesis of SC is not yet completely understood. Mutational inactivation of p53 may be pathogenetically relevant in MTS-associated SC and sporadic cases (5, 6). Immunohistochemical analyses have demonstrated that proteins involved in angiogenesis, cell proliferation and inflammation, such as epidermal growth factor receptor (7) and vascular endothelial growth factor receptor (VEGFR) (8), are overexpressed in SC and may play a role in its pathogenesis.
To the best of our knowledge, this is the first study analysing the expression of proteins related to angiogenesis in ocular and extraocular SC using a broad panel of immunohistochemical markers, including D2-40 (podoplanin), vascular endothelial growth factor (VEGF), VEGFR-2 (KDR) and VEGFR-3 (FLT4). These proteins may not only contribute to the pathogenesis of SC but also act as potential therapeutic targets.
Specimens
A total of 40 SC cases, including 18 ocular (female/male: 9/9) and 22 extraocular (female/male: 14/8) cases, were analysed by immunohistochemistry. The mean ± standard deviation (SD) age of patients with ocular SC was 84 ± 1.41 years (range 49–96 years), and the mean ± SD age of patients with extraocular SC was 71 ± 9.19 years (range 33–100 years).
Immunohistochemistry
Details regarding each individual antibody, clone, source, dilution and pretreatment are summarized in Table I. To evaluate the expression of D2-40, VEGF, VEGFR-2 and VEGFR-3 in the SC specimens, a quantification score (QS) was calculated by multiplying the relative proportion of positive tumour cells (levels of positivity: 0 = 0%, 1 = up to 1%, 2 = 2–10%, 3 = 11–50%, and 4 = > 50%) by the value of the staining intensity (level of intensity: 0 = negative, 1 = low, 2 = medium, and 3 = strong). If several ranks of intensity were present in one specimen, the single products were added together for a sum score. The specimens were studied in a “blinded” setting (i.e., without knowledge of the diagnosis, section number, or clinical data).
Additionally, epidermal VEGF expression was evaluated by measuring the staining intensity (level of intensity: 0 = negative, 1 = low, 2 = medium, and 3 = strong) of VEGF in epidermal keratinocytes.
To provide an estimate on the extent of lymphangiogenesis in SC, we counted lymphatic microvessel density (LMVD) in the D2-40 stained sections as previously described in detail (9). In short, LMVD was counted in high-power fields (HPF) (micro-scopic objective 40, here: 1.96 mm2). The lymphatic vessels were grouped by diameter: < 10 μm, 10 to 25 μm, and > 25 μm. For this grouping, the shortest transverse axis of each vessel section was assessed under a measuring ocular field. LMVD was calculated relative to the number of investigated HPF in 3 different areas of interest in each sample: intratumoural, paratumoural (upper horizontal dermal lymphatic plexus superficial to and on both sides of the SC), and intraindividual control tissue (ICT), which was defined as extratumoural areas at a distance of at least 5 mm from the tumour tissue. Only specimens that contained enough extratumoural tissue were included in this analysis.
Table I. Antibodies
Statistical methods
The statistical analysis was performed using the SPSS statistical package, version 24.0 (SPSS Inc., Chicago, Illinois, USA). Significant differences in the expression of the different proteins were calculated using the Mann-Whitney U test. p-values < 0.05 were considered statistically significant. For descriptive analyses, the data were presented as box plots with medians, interquartile ranges, and ranges. For the correlation between the different protein expression scores and the expression scores and clinical data (age and sex), Kendall’s tau correlation coefficient and Spearman’s rank correlation coefficient were calculated.
Ocular versus extraocular sebaceous carcinoma
The expression of all the analysed proteins and the LMVD were assessed separately for both subgroups (ocular versus extraocular SC) and compared between the two subgroups.
Lymphatic microvessel density
We found no significant differences in the mean ± SD LMVD of small lymphatics (< 10 μm) comparing intratumoural (8.2 ± 3.83), paratumoural (9.06 ± 6.46), and ICT (7.23 ± 4.39) areas (all p > 0.221). The ratio of the small lymphatics to the larger lymphatics was significantly increased within the tumours (1.04 ± 0.66) compared with the paratumoural (0.47 ± 0.23; p < 0.001) and ICT areas (0.36 ± 0.1; p < 0.001). The comparison of small lymphatics in paratumoural tissue versus ICT revealed no significant differences (p = 0.078).
Vascular endothelial growth factor expression
VEGF was expressed in 52.5% (21/40) of the analysed SC samples. Tumoural VEGF expression was rather low to moderate. Epidermal VEGF expression was rated as strong (score: 3) in 81% of the investigated specimens. Interestingly, the epidermis directly above the tumour tended to show higher VEGF expression than the epidermis located at the periphery of the tumour (Fig. 1a).
Fig. 1. Vascular endothelial growth factor (VEGF), D2-40, vascular endothelial growth factor receptor (VEGFR)-2 and VEGFR-3 expression in sebaceous carcinoma. a) Sample showing strong VEGF expression in all epidermal cell layers of the epidermis overlying the carcinoma. Note that VEGF expression is restricted to the uppermost cell layer in the paratumoural epidermis. Tumour cells lack VEGF production in this case. (VEGF staining, original magnification x 25). b) Section showing focal, moderate D2-40 positivity of tumour cells and strong D2-40 expression in lymphatic vessels (D2-40 staining, original magnification x 50). c) Specimen showing that VEGFR-2 expression is restricted to the intratumoural vasculature, whereas the tumour cells lack VEGFR-2 expression (VEGFR-2 staining, original magnification x 50). d) Section revealing strong tumoural VEGFR-3 expression (VEGFR-3 staining, original magnification x 50).
Tumoural VEGF expression showed no significant difference between the two groups of ocular and extraocular SC (p = 0.054). In contrast, the mean ± SD epidermal VEGF expression was significantly stronger in extraocular SC (2.86 ± 0.63) as compared with ocular SC (2.13 ± 1.18; p = 0.01) (Fig. 2).
Fig. 2. Expression scores of vascular endothelial growth factor (VEGF), VEGF epidermal, vascular endothelial growth factor receptor (VEGFR)-2, VEGFR-3 and D2-40 in ocular and extraocular sebaceous carcinoma. *p < 0.05.
Vascular endothelial growth factor receptor-2 and -3 expression
VEGFR-2 positivity was found in 52.5% (21/40) of the specimens with a low to moderate intensity of expression. In comparison, VEGFR-3 was expressed in all analysed SC specimens and at much stronger intensities. In total, 47.5% (19/40) samples showed an expression score of ≥ 12. When using the Mann-Whitney U test, the mean ± SD VEGFR-3 expression (9.42 ± 2.94) was significantly stronger than VEGFR-2 expression (2.15 ± 2.42; p < 0.001) in all analysed SC specimens without subgroup stratification.
When comparing the ocular versus extraocular VEGFR-2 expression, the mean ± SD expression was significantly stronger in ocular SC (3.22 ± 2.66) as compared with extraocular SC (1.27 ± 1.83; p = 0.01) (Fig. 2). VEGFR-3 expression showed no significant difference between ocular SC (10.05 ± 2.73) and extraocular SC (8.90 ± 3.06; p = 0.21) (Fig. 2). Interestingly, in ocular SC, the mean ± SD expression of VEGFR-3 (10.05 ± 2.73) was significantly stronger than VEGFR-2 expression (3.22 ± 2.66; p < 0.005). A similar difference was also observed in extraocular SC. Again, VEGFR-3 expression (8.90 ± 3.06) was significantly stronger than VEGFR-2 expression (1.27 ± 1.83; p < 0.005).
D2-40 expression
In total, 77.5% (31/40) of the analysed SC were D2-40 positive. D2-40 expression was low to moderate in the majority of the tumours. The mean ± SD D2-40 expression was not significantly different between ocular SC (3.27 ± 2.96) and extraocular SC (5.45 ± 4.35; p = 0.06) (Fig. 2).
Statistical correlation analyses
Protein expression levels. Tumoural VEGF and VEGFR-2 expression were positively correlated using Kendall’s tau correlation (correlation coefficient: 0.354, p < 0.05) and Spearman’s rank correlation (correlation coefficient: 0.424, p < 0.05). No other proteins showed a significantly correlated expression level.
Protein expression levels and LMVD. Interestingly, epidermal VEGF expression showed a significantly negative correlation with the intratumoural LMVD of all vessel subgroups using Kendall’s tau correlation (correlation coefficient: small vessels: –0.464, p < 0.005, medium vessels: –0.458, p < 0.005, and large vessels: –0.361, p < 0.05) and Spearman’s rank correlation (correlation coefficient: small vessels: –0.541, p < 0.005, medium vessels: –0.589, p < 0.005, and large vessels: –0.418, p < 0.05). The LMVD of the paratumoural and control tissue was not significantly correlated with epidermal VEGF expression. Furthermore, LMVD was not significantly correlated with VEGF, VEGFR-2 or VEGFR-3 expression.
Protein expression levels and clinical data. None of the expression levels of the proteins was significantly correlated with patient age or sex.
Proteins related to angiogenesis, cell proliferation and inflammation are significantly overexpressed in SC (8). Lymphatic vessel formation and lymphatic vessel invasion by tumour cells are central events during the development of lymphatic metastasis (10). Podoplanin, VEGF, VEGFR-2 and VEGFR-3 play leading roles in these complex biological processes.
Podoplanin is strongly expressed in endothelial cells of growing and maturing lymphatic vessels and in a variety of malignant tumours (i.e., cutaneous squamous cell carcinoma), specifically in the tumour cells themselves and stromal cells, whereas endothelial cells of blood capillaries lack podoplanin expression (10–12).
In all, 77.5% (31/40) of our SC samples were D2-40 positive (Fig. 1b), whereas in another study, only 56% of the analysed SC expressed D2-40 (13). This difference may be due to the more representative greater number of cases in our study.
Recently, the identification of the ratio of small lymphatics (<10 μm) to larger lymphatics proved to be a robust tool to identify cutaneous lymphangiogenesis (9). Although we found no significant differences in the LMVD of small lymphatics comparing the intratumoural, paratumoural and ICT areas, the ratio of small lymphatics to larger lymphatics was significantly increased in the intratumoural areas compared to the paratumoural and ICT areas. Therefore, we assume that SC has the ability to induce intratumoural lymphatic microvessel formation. Our findings with regard to lymphangiogenesis are in contrast to the data of Yang et al. (13), who found no lymphangiogenetic potential in SC. This discrepancy might be explained by the use of more detailed methods of counting lymphatic vessels and the calculation of the ratio of small lymphatics to larger lymphatics by our group.
VEGF signalling is crucial for physiologic and pathologic (lymph-) angiogenesis and represents a potential target of anticancer therapy (14). Cutaneous VEGF expression has been shown in normal epidermis, epidermal appendages, skin tumours and in inflammatory/non-neoplastic conditions (15–18). Normal human epidermis exhibits low to moderate VEGF expression with basal cells tending to be less reactive or negative (16). In addition to its paracrine actions on endothelial cells, VEGF may promote skin carcinogenesis by altering the survival, proliferation or stemness of epidermal keratinocytes and tumour cells via an autocrine loop. Furthermore, immune cells, such as macrophages, are recruited by VEGF expression and contribute to skin carcinogenesis (19–21).
Interestingly, in the vast majority of cases, we found higher epidermal expression levels of VEGF in the epi-thelium directly above the SC, including all epidermal cell layers, compared with the paratumoural epidermis that revealed VEGF expression only in the uppermost cell layers (Fig. 1a). We interpret the strong expression of VEGF in peritumoural epidermis as an interaction of tumour cells with the overlying epithelium. VEGF production by keratinocytes may be stimulated by the production of transforming growth factor-alpha and other cytokines released by tumour cells (19). The increased epidermal VEGF production consecutively leads to angiogenesis through paracrine effects on endothelial cells and may additionally stimulate proliferation, maintain stemness and promote survival of tumours through direct effects on tumour cells (19).
Interestingly, we demonstrated a negative correlation between epidermal VEGF expression and the density of all intratumoural lymphatic vessel subgroups. One could speculate that less vascularized SC may interact via an unknown feedback loop with the epidermis to increase the intratumoural vessel density through increased epidermal VEGF production.
Furthermore, we found a positive correlation between the epidermal VEGF expression and tumoural VEGFR-2 expression, indicating that epidermal VEGF production stimulates VEGFR-2 expression. Nevertheless, no correlation was noted between epidermal VEGF expression and tumoural VEGF or VEGFR-3 expression.
Taken together, our findings suggest that VEGF expression by epidermal keratinocytes and tumour cells and its interaction with VEGFR-2 seems to contribute to the pathogenesis of SC not only by its effects on angiogenesis but also by direct effects on the tumour cells.
Our findings of VEGFR-2 expression in SC are in contrast to the data of Erovic et al., who described VEGFR-2 expression in all of their investigated samples (8). Only 52.5% of our specimens were VEGFR-2 positive (Fig. 1c), indicating a minor role in the pathogenesis of SC compared with VEGFR-3, which exhibited significantly higher expression in SC. Nevertheless, VEGFR-2 expression in our cohort was significantly stronger in ocular SC than in extraocular SC (Fig. 2). These findings indicate that the pathogenesis of ocular and extraocular SC might be different, leading to an increased tendency of regional metastases in ocular SC (4). VEGFR-2 expression in tumours may have translational relevance given the availability of VEGFR-2-specific tyrosine kinase inhibitors.
Expression of VEGFR-3 is largely confined to lym-phatic endothelial cells in adult tissue (10, 14). Only a few studies analysing its expression in tumour cells and tumour vasculature are available, and there are conflicting reports regarding VEGFR-3 location (endothelial cells and/or tumour cells) (14). One study found no expression of VEGFR-3 by tumour cells in a variety of human primary solid cancers, whereas the vascular endothelial cells within these tumours strongly expressed VEGFR-3 (14). Other studies clearly showed VEGFR-3 expression in prostate cancer cells (22), endometrial carcinoma cells (23) and non-small cell lung cancer cells (24).
We found that VEGFR-3 was strongly expressed in many of the analysed SC samples (Fig. 1d). Additionally, VEGFR-3 expression was significantly higher than VEGFR-2 expression in both ocular and extraocular SC. Our findings regarding VEGFR-3 expression indicate that this protein may play a critical role in the pathogenesis of SC and therefore might be of therapeutic interest.
Two of our central findings, namely, an increased intratumoural ratio of small lymphatics to large lymphatics and a negative correlation between epidermal VEGF expression and the intratumoural density of lymphatics, clearly underline the hypothesis regarding the lym-phangiogenetic potential of SC.
In summary, despite some limitations (i.e., small cohort and no clinical follow-up data), our data shed more light on the pathogenesis of SC and may provide translational relevance as a more detailed understanding of the expression and localization of VEGF and its receptors, and the lymphatic vessel architecture in SC might help in identifying patients who could benefit from anti-VEGF or anti-VEGFR therapy in advanced stages of the disease.


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize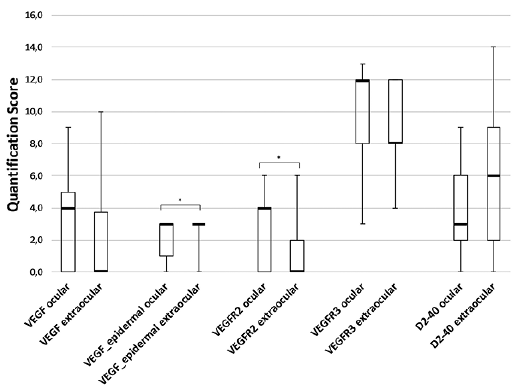 Click to show fullsize
Click to show fullsize