


Department of Dermatology, University Hospital Zurich, Gloriastrasse 31, CH-8091 Zurich, Switzerland. *E-mail: reinhard.dummer@usz.ch
Accepted Oct 17, 2019; E-published Oct 18, 2019
Acta Derm Venereol 2020; 100: adv00007.
Immune checkpoint inhibitors (ICIs) and kinase inhibitors (BRAF and MEK inhibitors) have improved clinical outcomes in patients with advanced BRAFV600 mutant melanoma. Preliminary results from ongoing, phase III clinical trials of combined ICIs and kinase inhibitors have shown a manageable safety profile with promising efficacy. However, unbridled activation of the immune system may be associated with a wide spectrum of autoimmune or inflammatory side-effects. We describe here a case of a 62-year-old woman with stage IIID melanoma, treated with anti-PD1, BRAF and MEK inhibitors, which resulted in proximal hair depigmentation of the scalp and patchy hair loss, with complete response (CR) of the disease. It can be hypothesized, that this case represents a clinical example of cross T-cell reactivity against shared antigens between tumour cells and melanocytes on previously protected sites on the hair follicle, which may indicate an anti-tumour efficacy in patients treated with ICI-based therapy.
ICIs have shown a remarkable response and survival benefit in metastatic melanoma (1). Their enhanced anti-tumour activity accrues through the inhibition of negative regulators of immune activation, such as CTLA-4 or PD-1, which, on the other hand, can deregulate immunological homeostasis, resulting in immune-related adverse events (irAE) (2). Alopecia areata (AA), an autoimmune disorder of patchy hair loss, has been reported in 0.9% of patients being treated with pembrolizumab (anti-PD1 monoclonal antibody (mAb)) and in 2% of patients being treated with nivolumab (anti-PD1 mAb) alone (3). We describe here a case of a 62-year-old woman with unresectable, stage IIID (AJCCv8), BRAFV600E mutant metastatic melanoma treated with anti-PD1 (spartalizumab 400 mg Q4W), BRAF inhibitor (dabrafenib 150 mg BID) and MEK inhibitor (trametinib 2 mg QD) in a clinical trial (NCT02967692). She was diagnosed with a polypoid cutaneous melanoma on her left lower leg (Breslow thickness 4.3 mm, with ulceration, without regression, pT4b) and presented with multiple iliac and inguinal lymph node metastases on the left side, as well as in-transit metastases on her left leg, with no distant metastases (N3c, M0). Her personal and family medical history was insignificant for any autoimmune or skin and hair diseases. She was treated initially with spartalizumab + dabrafenib + trametinib for 3 treatment cycles and developed immune-related (ir) Sjögren syndrome (Grade 2, CTCAEv4), secondary to her melanoma treatment with clinical signs of xerostomia and xerophthalmia, laboratory signs of elevated antinuclear antibodies (ANA 1:320) and anti-SSA antibodies > 240 U/ml (n < 10), and histological signs of chronic granulomatous sialadenitis in a lower lip biopsy. She had received 7 treatment cycles, resulting in a complete response (CR) of her tumour.
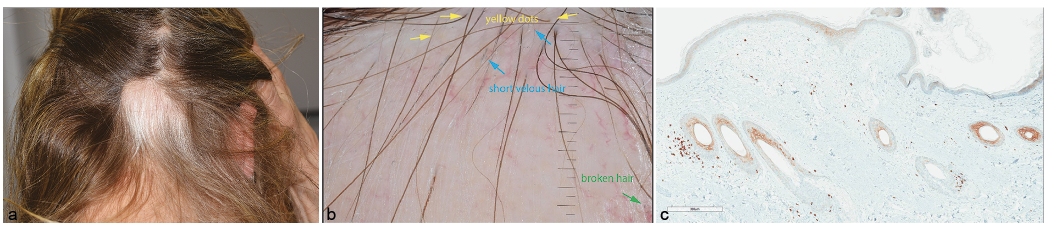
Six months after the initiation of treatment the patient presented with well-demarcated areas of proximal hair depigmentation, which resulted in patchy hair loss limited to her scalp, and symmetrical patches of depigmentation on the skin of both forearms, consistent with “vitiligo-like” depigmentation. No nail or mucosal alterations were observed. Clinical examination of the scalp revealed diffuse hair thinning and well-defined areas of proximal depigmentation of the hair, resulting in non-scarring alopecia (Fig. 1a). The hair pull test was positive. Dermoscopy showed multiple yellow dots surrounding the hair follicle openings, vellus hair and broken hair (Fig. 1b). Histopathology of the scalp revealed mild perifollicular lymphocytic inflammation, intrafollicular infiltrate of CD8+ T cells mostly in the deep dermis, and isolated CD4+ T cells (Fig. 1c). Laboratory investigations were unremarkable for thyroid dysfunction or an underlying infection. A diagnosis of immune-related AA (irAA) was established. She began treatment with topical steroids (clobetasol foam), resulting in an amelioration of the alopecia. In areas of previous hair loss she developed regrowth of white hair.
Fig. 1. (a) Scalp with patchy hair loss with multiple, well-defined areas of non-scarring alopecia, diffuse hair thinning and proximal depigmentation. (b) Dermoscopy with multiple yellow dots surrounding the hair follicle openings, short velous hair and broken hair. Scale bar corresponds to 1 mm. (c) Immunohistochemical staining for CD8+ of a biopsy specimen (original magnification ×100) with mild perifollicular lymphocytic inflammation, intrafollicular infiltrate of CD8+ T cells mostly in the deep dermis and isolated CD4+ T cells.
AA is an autoimmune condition affecting the hair follicle, and is characterized histologically by immune infiltration against pigmented hair, with perifollicular lymphocytic infiltrates, primarily CD4+ (4). There have been rare reports of AA secondary to ICIs (3). Due to the rare incidence of this irAE, very little data concerning its clinical and histological presentation are available. It is notable that vitiligo-like depigmentation is correlated with anti-tumour efficacy in patients with metastatic melanoma, treated with immunotherapy (5). In contrast to the observed poliosis associated with hair regrowth in areas of previous hair loss in AA (6), in the above-mentioned case, proximal hair depigmentation of well-demarcated areas on the scalp was observed prior to hair loss, which subsequently resulted in alopecia. We hypothesize that this case of localized hair-depigmentation, also similarly described in vitiligo-like depigmentation cases (5), is an example of an antigen-specific immunity in patients with melanoma. Hair loss is the subsequent result of this “off-target” attack. As a possible pathomechanism we consider a T-lymphocyte-mediated cross-reactivity between tumour cell antigens and related antigens in the protected melanocytes of the hair bulb, as described in ir-AA (2). This theory correlates with our immunohistochemical findings, of intrafollicular predominant CD8+ infiltrates (Fig. 1c). Previously reported cases of localized hair re-pigmentation in melanoma have correlated melanin production from melanoma cells in hair follicle melanocytes by paracrine stimulation, probably induced by growth factors, such as c-kit ligand (7). It is notable that, in both cases, no melanoma cells were seen histologically in the hair papillae.
It has been proposed that microphthalmia-associated transcription factor (MITF), may contribute to the connection between melanoma response to immuno-therapy and vitiligo (8). Malignant transformation of the melanocytes occurs, among other mechanisms, also as a result of the disruption of the regular function of MITF as a melanocyte lineage promoter, thus prompting the immune system to recognize specific epitopes not only on melanoma cells, but also on normal melanocytes. These findings may correlate with the clinical observation of pigmented hair being lost preferentially to non-pigmented hair and also with the observation that in most cases hair regrowth tends to appear nonpigmented. In vivo data suggest that optimal transfer of hair loss in mice requires both CD4+ and CD8+ T cells (9). In addition to T cells, increased IFN-γ response indicative of T-cell activation following enhanced anti-tumour activity induced by ICI may also be involved in the pathophysiology of the disease. Besides, clinical and preclinical data prove that blockade of common signalling pathways downstream of cytokine receptors (JAK/STAT) could clinically reverse AA (10).
Recently, ongoing clinical trials combining immuno-therapy and targeted therapy for the treatment of metastatic melanoma have shown promising efficacy with a manageable safety profile (11). Dual MAPK pathway inhibition through BRAF and MEK inhibitors induce significant changes in the tumour microenvironment, thus making tumours more susceptible to immunotherapy (12). However, the release of numerous pro-inflammatory cytokines and kinase inhibitors may lead to aberrant immune activation (13). It can be hypothesized that this dual immune activation may be associated with susceptibility to irAA in predisposed individuals. However, further research is needed to determine whether the frequency of these events is increased compared with immunotherapy alone.
The authors thank Mr Phil F. Cheng for the help with the figures.
Conflicts of interest. FD receives intermittent travel support from Amgen and Pierre Fabre outside of the submitted work. JM has intermittent project-focused consultant or advisory relationships with Merck/Pfizer, Merck Sharp & Dohme and Pierre Fabre and receives travel support from Merck Sharp & Dohme und Pierre Fabre outside of the submitted work. RD has intermittent, project-focused consulting and/or advisory relationships with Novartis, Merck Sharp & Dhome (MSD), Bristol-Myers Squibb (BMS), Roche, Amgen, Takeda, Pierre Fabre, Sun Pharma, Sanofi outside the submitted work.


 Click to show fullsize
Click to show fullsize