


1Department of Dermatology, 2Institute of Biostatistics and Clinical Research, University of Muenster, Münster, and 3Department of Dermatology and Venereology, University Hospital Halle (Saale), Martin-Luther-University Halle-Wittenberg, Halle/Saale, Germany
Clinical differentiation between herpes zoster and bacterial superficial skin and soft tissue infections of the face can be difficult. In addition, diagnosis can be complicated by bacterial superinfection of lesional herpes zoster. The aim of this study was to determine whether inflammatory parameters, such as C-reactive protein (CRP) and blood counts, might be reliable biomarkers to distinguish between skin and soft tissue infections and herpes zoster when the face is infected. The study data (multivariate analysis and area under the curve) identified CRP (0.880) and leukocytes (0.730) together as the parameters that best discriminate between skin and soft tissue infections and herpes zoster. A CRP threshold ≥ 2.05 mg/dl indicated a diagnosis of skin and soft tissue infection with a sensitivity of 80% and specificity of 83.8%. For leukocytes ≥ 7.3×109/l, diagnosis of skin and soft tissue infection had a sensitivity of 75% and specificity of 67.6%. Thus, when differential diagnosis is difficult, CRP and leukocytes should be determined, while parameters such as neutrophils or immature granulocytes do not add diagnostic value.
Key words: herpes zoster; SSTI; cellulitis; erysipelas; CRP; leuko-cytes.
Accepted Oct 17, 2019; E-published Oct 18, 2019
Acta Derm Venereol 2020; 100: XX–XX.
Corr: Jan Ehrchen, Department of Dermatology, University of Muenster, Von-Esmarch Strasse 58, DE-48149 Muenster, Germany. E-mail: jan.ehrchen@ukmuenster.de
Clinical differentiation between superficial skin and soft tissue infections (SSTI, including cellulitis and erysipelas) and herpes zoster of the face can be difficult. Moreover, bacterial superinfection can develop in patients with herpes zoster. This may lead to delayed treatment or unnecessary use of antibiotics, which could lead to further microbial resistance or higher costs of treatment. This analysis of diagnostic parameters is often determined as standard of care in hospitalized patients and can help clinicians to guide their treatment decisions.
Superficial skin and soft tissue infections (SSTIs) (often referred to as cellulitis and sometimes encompassing erysipelas) and herpes zoster (HZ) are among the most common diagnoses leading to hospitalization in departments of dermatology. HZ is caused by reactivation of the varicella zoster virus. Its initial symptom is usually a burning pain, followed by erythema and then eruption of aggregated vesicles in a dermatomal distribution.
In our patients SSTIs comprise erysipelas and limited cellulitis (1). Erysipelas are caused by group A streptococci and are clinically characterized by an acute beginning, variably tender, bright-red erythema, and sharply demarcated borders. Depending on the type of bacterial toxins and the patient’s inflammatory response, blistering and haemorrhages may occur, but aggregated vesicles are usually not present. Limited cellulitis is most frequently caused by S. aureus (Staphylococcus) and is characterized by an infection of the dermis and subcutis extending a little deeper into the tissue than erysipelas. The lesion usually has a darker or more livid-red colour, is less shiny and less sharply demarcated than classic erysipelas, probably because it involves deeper tissue layers.
Although the clinical differential diagnosis between SSTIs and HZ is often not difficult for the experienced dermatologist, it is challenging in certain cases. When localized on the face, SSTIs are not always sharply demarcated, due to the anatomy of the region with loose connective tissue, and their distribution can be limited within a dermatome.
On the other hand, HZ can initially present with erythema without blisters. Moreover, the degree of pain varies in patients with HZ and, especially in elderly persons or patients with diabetes mellitus, does not differ decisively from the burning pain experienced by some patients with SSTI. Furthermore, there is a risk of ensuing bacterial infection in HZ due to disruption of the skin barrier by the vesicles.
The decision to treat patients with either antiviral or antibiotic therapy, or both, can therefore sometimes be difficult, and additional diagnostic parameters are needed.
Laboratory parameters of inflammation are often determined as standard of care, but the diagnostic value of these parameters for differentiation between these conditions has not yet been specifically addressed.
This study systematically investigated whether both standard laboratory parameters of inflammation, such as C-reactive protein (CRP) and complete and differential blood counts, or recently established parameters, such as immature granulocytes or platelet volume, are reliable biomarkers to differentiate between SSTI and HZ. There are some data on the variability of inflammatory markers, such as CRP, leukocytes and neutrophilic granulocytes, in patients with SSTIs (2–4), and on their value to discriminate erysipelas from necrotizing bacterial SSTI or non-infectious conditions, such as thrombosis (5, 6). There are also many data on both established and novel markers of inflammation in viral and bacterial systemic infection (7, 8), but no studies were found on the diagnostic value of these laboratory parameters to differentiate SSTIs from HZ.
Patients who were admitted to the Department of Dermatology at the University of Muenster between 1 January 2013 and 31 December 2017 with the diagnosis “herpes zoster”, “limited cellulitis”, “erysipelas” were identified in the hospital administration software “Orbis” by using the International Classification of Disease 2010 (ICD-10) codes “A46” for limited cellulitis/erysipelas, and “B02” for herpes.
Exclusion criteria were: patients with other skin infections, such as abscesses, carbuncles, inflamed epidermoid cysts, impetigo or severe, necrotizing soft-tissue infection; those on immunosuppressive therapy (e.g. glucocorticoids), chemotherapy, patients with cancer, and those with haematopoiesis disorders.
A final total of 242 patients were included. Patient data-sets were examined for localization of infection, age, sex, body temperature (Celsius, auricular measurement), CRP (mg/dl), leukocytes, erythrocytes, blood platelets, neutrophils, lymphocytes, eosinophils, immature granulocytes (all: ×109/l) and mean platelet volume (fl). In a second step patients with a diagnosis of both SSTI and HZ were identified and grouped as a separate cohort, which was excluded from the primary analysis. These patients received both antibiotic and antiviral treatment. In more than 75% of patients with HZ the lesions were localized on the face (i.e. trigeminal zoster in V1–3). Since the localization of the infection might influence laboratory markers, patients were grouped according to the anatomical region affected. Patient data were entered pseudonymously into Excel. Statistical analyses were performed using IBM SPSS® Statistics Version 25 for Windows (IBM Corporation, Somers, NY, USA). To evaluate differences between 2 groups, Mann–Whitney U test was used. Inter-group comparisons concerning categorical data were made by χ2 test. The diagnostic values of the laboratory parameter for differentiating between SSTI and HZ were compared by receiver-operator characteristics (ROC) analysis. The area under the ROC curve (AUC) is a measure to compare the marker’s performance to distinguish between the 2 groups. Youden’s Index was used to determine the optimal cut-off values. The variables were then entered into binary logistic regression analysis to identify predictors for the diagnosis of SSTI or HZ. All tests of significance were 2-tailed and, for each test, a p-value ≤ 0.05 was considered statistically noticable. The study was approved by the local ethics committee (AZ 2018-763-f-S).
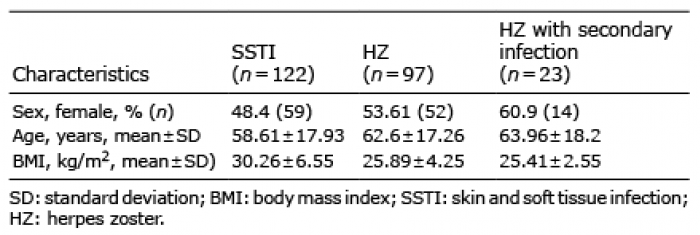
In this study (Table I, Fig. 1) 122 subjects with SSTI, 97 with HZ and 23 with both HZ and suspected bacterial infection were enrolled. The face was affected in 32.8% of patients with SSTI. HZ of the face was found in approximately 75% of all cases. In the third group all infections were detected on the face. Patients with SSTI had a higher body mass index (mean ± standard deviation (SD) 30.26 ± 6.55 kg/m2) than the HZ-group (25.89 ± 4.25 kg/m2), but did not differ in sex and age.
Table I. Demographic distribution of patients with skin infection on the face
Fig. 1. Distribution of skin infections.
Skin and soft tissue infection vs. herpes zoster
In order to exclude the effects of the site of infection on the measured parameters, only patients with the same anatomical region affected were compared. Detailed analysis was possible for patients with inflammatory lesions on the face. Since this group contained a relatively small number of patients, differentiation of SSTI into erysipelas and limited cellulitis was statistically not possible. Moreover, clinical differentiation between limited cellulitis and erysipelas on the face is not always easy and there is a high risk of S. aureus colonization and consecutive infection in this region. Hence, SSTIs of the face have always been treated with intravenous broad-spectrum antibiotic cefuroxime, which covers both bacterial infections. In the analysis this resulted in no further differentiation between these SSTIs.
The median values of body temperature and the recorded laboratory markers are shown in Table II. In comparison with HZ, subjects with SSTI had (p < 0.05) higher values for body temperature, CRP, leukocytes and neutrophils, while values for basophils were lower.
Table II. Body temperature and laboratory markers in patients with skin or soft tissue infection (SSTI) on the face
In univariate analysis ROC analysis was used to identify the discriminatory ability of these parameters (Table III and Fig. 2). Compared with the clinical parameter body temperature (AUC (0.699; 95% CI 0.582, 0.816)), the laboratory markers CRP (0.880; 95% CI 0.812, 0.948) followed by leukocytes (0.730; 95% CI, 0.631, 0.829) and neutrophils (0.717; 95% CI, 0.609, 0.824) showed higher discriminative values, while the AUC for basophil count was lower (0.665; 95% CI, 0.553, 0.776).
Table III. Area under the receiver-operator characteristics (ROC) curve (AUC) for significant parameters to discriminate skin or soft tissue infection (SSTI) and herpes zoster
Fig. 2. Receiver-operator characteristics (ROC) curves with highest values of laboratory parameters and body temperature for discriminating skin and soft tissue infections (SSTI) from herpes zoster on the face.
Threshold values with optimal sensitivity and specificity to discriminate between HZ and SSTI were identified. At a CRP threshold ≥ 2.05 mg/dl the sensitivity for diagnosis of SSTI was 80% and specificity was 83.8% (Youden’s Index (YI) 0.64). For CRP ≥ 0.90 mg/dl the sensitivity increased to 90%, but specificity decreased to 71.6% (YI 0.62). At a leukocyte threshold of 7.3 × 109/l sensitivity was 75% and specificity was 67.6% (YI 0.43), respectively. This threshold lies within the normal range for leukocytes. A leukocyte count above the threshold for the normal range (≥ 12.68 × 109/l)) showed a low sensitivity of 13%, but a very high specificity of 98.6% (YI 0.11). Neutrophils counts ≥ 4.23 × 109/l (within the normal range) showed a sensitivity of 84.4% and a specificity of 54.2% (YI 0.39). The sensitivity for neutrophils elevated above the laboratory cut-off for the normal range (≥ 6.98 × 109/l) was 31.3% and specificity was 86.4% (YI 0.18). Body temperature raised above a threshold of 37.5°C (auricular) had a lower YI and the sensitivity for the diagnosis SSTI was 48.6% with a specificity of 87%.
Multivariate analysis using logistic regression identified that only the laboratory parameters CRP and leukocytes, in combination with the clinical parameter body temperature, are needed for optimal separation of the 2 diagnoses. The odds ratio (OR) for the diagnosis SSTI vs. HZ increased 4.26-fold with every increased degree Celsius in body temperature, 1.96-fold with an increase of 1 mg/dl CRP level and 1.29-fold with an increase of 1,000 leukocytes/µl (Table IV).
Table IV. Odds ratio for C-reactive protein, leukocytes and body temperature
The addition of other laboratory parameters, such as neutrophils, did not improve separation in the logistic regression analysis.
In order to depict the correlation of these 2 parameters a dispersion diagram was used (Fig. 3). At CRP levels below 1.0 mg/dl the probability of a diagnosis of SSTI is very low independently from the leukocyte values. Similarly, very high CRP levels > 10 mg/dl were always associated with the diagnosis SSTI. In patients with CRP levels between 1.0 and 10.0 mg/dl leukocytes were most useful to predict the probability of SSTI.
Fig. 3. Dispersion diagram showing the correlation between leukocytes and C-reactive protein (CRP) levels in the differential diagnosis herpes zoster vs. skin and soft tissue infections (SSTI).
Herpes zoster with suspected secondary bacterial infection
Some patients with clinically typical HZ of the face were excluded from the primary analysis in the current study because a bacterial superinfection was clinically suspected and thus the patients were treated with both antiviral and antibiotic therapy. To test whether these patients differ with respect to laboratory parameters, this patient group was compared with the HZ cohort.
Differences in significance were seen only at higher levels of CRP (p < 0.05; AUC 0.693 (95% CI 0.562–0.823) compared with the HZ cohort.
The clinical differentiation between HZ and SSTI, especially when localized on the face, can be challenging, and the analysis of additional diagnostic parameters is warranted for more rationale treatment decisions (9).
CRP and leukocytes are well-established markers for bacterial infection in general (7, 10), but there are only limited data on their relevance in the diagnosis of skin infections. Moreover, there are only 2 studies reporting values of novel inflammatory markers, such as immature granulocytes and platelet volume in patients with SSTI (11, 12). No currently commercially available laboratory marker is specific for bacterial or viral infections. As an example, CRP is produced in the liver in response to cytokines (e.g. interleukin-6), released by cells of the innate immune system. Cytokine release is triggered by pattern recognition receptors, which can be activated by pathogen-associated molecular patterns in bacterial infections. These receptors, however, are also activated by endogenous ligands, called damage-associated molecular patterns, which can be released in response to situations of tissue damage due to cancer, autoimmunity or viral infections (13–15). Thus, data on specificity and sensitivity of laboratory markers must be specifically determined for every diagnostic situation and are completely lacking for the differential diagnosis of HZ and SSTI.
A threshold of CRP ≥ 2 mg/dl indicated a diagnosis of SSTI with a sensitivity of 80% and a specificity of 83.8%. Only 4.6% of SSTIs showed CRP levels < 0.5 mg/dl when treatment was started. This is in agreement with previous reports, which demonstrated normal CRP levels in 3–12% of patients with SSTI upon admission (3, 4). We did not specifically study parameters that indicate additional bacterial superinfection in initially clinically typical HZ; however, our data indicate that CRP levels greater than 2 mg/dl or increasing CRP levels could raise suspicion of superimposed bacterial infection in these patients.
The second laboratory parameter that can help to differentiate SSTI from HZ is the leukocyte count. Increased numbers of leukocytes are well known to indicate systemic bacterial infection; however, the specificity of leukocytes as a marker of bacterial infection is generally much lower than that of CRP (3, 4, 16). The increase in blood leukocytes is also mediated via cytokines released in response to signals that activate pattern recognition receptors on cells of the innate immune system. Systemic bacterial and viral infections in general cannot be easily discriminated based on elevated leukocytes (17–19). In agreement with this, leukocyte count in comparison with CRP shows a lower ability to discriminate SSTI from HZ in our patients. In our cohort only 41.8% of patients with SSTI had normal leukocyte counts. This is in agreement with previous data, which demonstrate that up to 50% of patients with SSTI have normal leukocytes (3, 4, 20). At a cut-off value of 7.3 × 109/l the sensitivity of leukocyte counts for SSTI was comparable to CRP levels, but the specificity was much lower. The combined measurement of CRP levels and leukocytes, however, improved discrimination between SSTI and HZ.
Neutrophil counts can be better predictors for bacterial infection than leukocyte counts (7), but in the current study neutrophils did not provide additional information in multivariate analysis.
In addition, significantly lower basophil counts were found in patients with SSTI. Basophils are usually not involved in bacterial or viral killing and they have not been demonstrated to change during systemic bacterial infection (21).
The more recently established inflammatory markers platelet volume and, especially, immature granulocytes, provide additional diagnostic information compared with leukocyte and granulocyte counts in patients with bacterial infection and sepsis (22, 23). However, in our patients these markers did not differ between patients with SSTI and HZ.
Our data indicate that CRP levels are most useful for discrimination between SSTI and HZ localized on the face, and we recommend measuring the CRP level when the clinical diagnosis is difficult. Whether CRP levels are also helpful in other anatomical regions must be established in consecutive studies. In our department, only patients with lesions on the face were treated with both antiviral and antibiotic drugs. This could be due to bacterial superinfection or difficulties making a definite diagnosis in this anatomical region. The results for this cohort must therefore be interpreted with caution. However, the current analysis showed that high levels of CRP in patients with well-established HZ might indicate a bacterial superinfection. Leukocyte counts are additional predictors of the diagnosis SSTI, especially in patients with medium levels of CRP (Fig. 3). Thus, a complete blood count should also be determined when clinical diagnosis is difficult, while neither the differential blood count nor additional markers, such as immature granulocytes or platelet volume, are helpful in this diagnostic setting. Therefore, these results also have an economic implication.
This study has the following limitations: (i) it presents a retrospective review of medical records. Therefore, we could not evaluate other inflammatory markers, such as erythrocyte sedimentation rate (ESR), procalcitonin (PCT), ferritin (4, 24) or anti-streptolysin titres, because they were not regularly determined in our patients. In particular, changes in anti-streptolysin titres during patient follow-up would provide additional information for discrimination between viral and bacterial infections due to streptococci. (ii) The presence of pathogens was not directly analysed and could differ between primary SSTI and bacterial superinfection of HZ (due to an increased risk of colonization of HZ lesions by S. aureus). (iii) Only blood samples from the day of admission, but no data on the time-course of these laboratory parameters were accessible in our patients. Thus, a prospective analysis taking all these considerations into account is highly warranted.
In conclusion, this study demonstrates that CRP levels are helpful to differentiate between SSTI and HZ of the face. The determination of leukocyte counts adds diagnostic value. Thus, if the clinical diagnosis is difficult, CRP levels and, ideally, leukocyte counts should be determined.


 Click to show fullsize
Click to show fullsize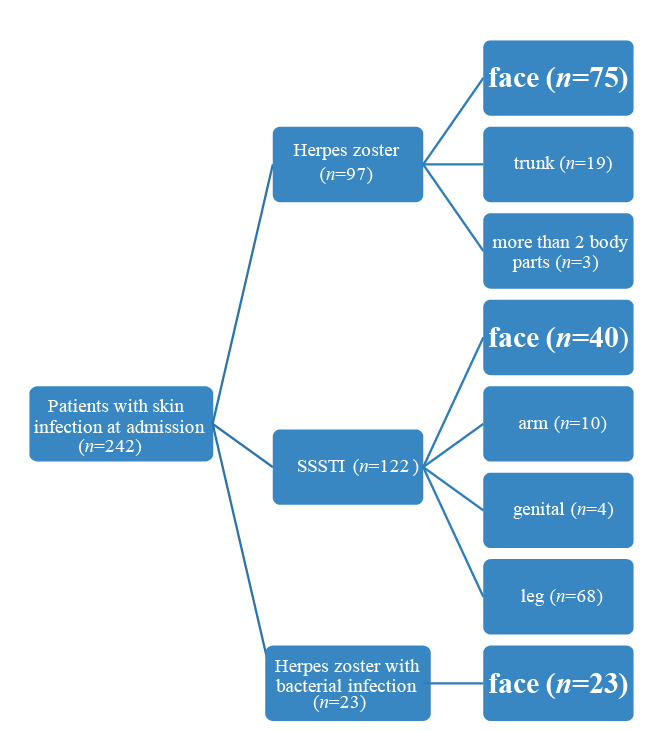 Click to show fullsize
Click to show fullsize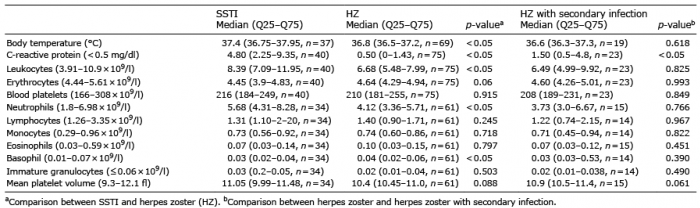 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize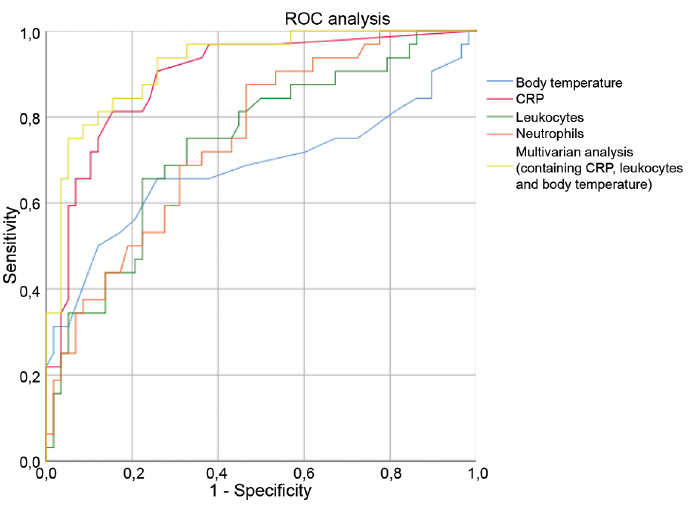 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize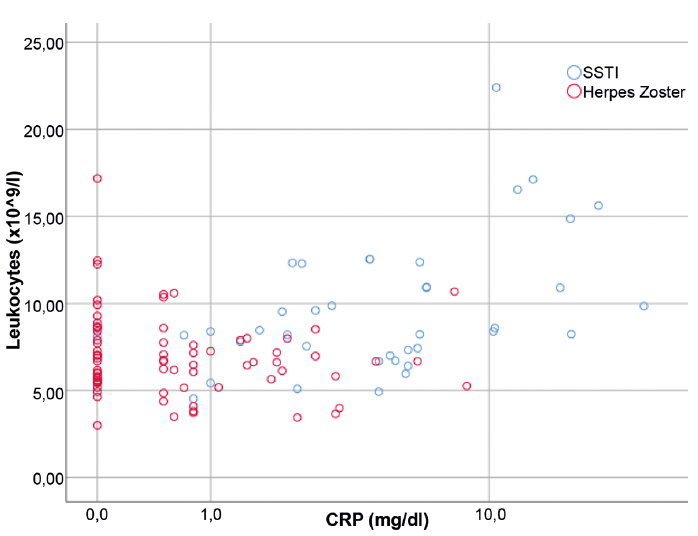 Click to show fullsize
Click to show fullsize