


1Department of Dermatology, Venereology, and Allergology, University Medical Center and Medical Faculty Mannheim, Heidelberg University, and Center of Excellence in Dermatology, 2Section of Clinical and Molecular Dermatology, and 3European Center for Angioscience, Medical Faculty Mannheim, Heidelberg University, Mannheim, Germany. *E-mail: cyrill.geraud@umm.de
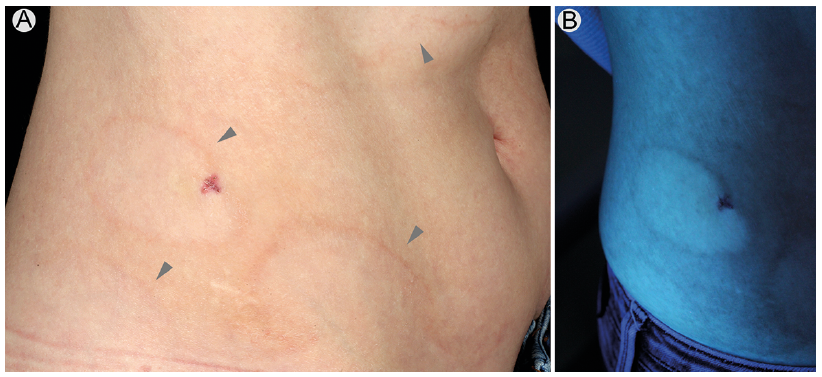
A 41-year-old woman presented to the outpatient department with annular erythematous lesions on her abdomen, which had appeared 8 years previously. The lesions were asymptomatic, relapsing and more pronounced during springtime. In recent months the lesions had been persistent, which had led the patient to present to a dermatologist. Furthermore, the patient reported the appearance of small white patches on her right arm 5–8 years earlier, which had progressed during the previous summer. Clinical examination revealed more than 10 non-confluent, 0.5–1 cm, well-circumscribed white macules on the ventral and dorsal sides of her arm, and the back of her right hand. Under Wood’s light, the lesions appeared bright white. On the lower abdomen the patient presented several extensive, larger than 5 cm diameter, annular patches with an elevated, erythematous border (Fig. 1A). The patches were depigmented compared with the non-affected skin. Due to the light complexion of the patient, the depigmentation was difficult to see in daylight. Wood’s light examination accentuated the depigmented areas (Fig. 1B). Her past medical history revealed autoimmune thrombocytopaenia, IgG deficiency, migraine and allergic rhinitis.
What is your diagnosis? See next page for answer.
Fig. 1. (a) Hypopigmented, large macules on the lower abdomen with an elevated erythematous border (grey arrowheads). (b) Wood’s light examination of the hypopigmented macules of the lower abdomen.
Acta Derm Venereol 2020; 100: XX–XX.
Diagnosis: Vitiligo with inflammatory raised borders
A punch biopsy from the erythematous border of a hypopigmented patch on the right lower abdomen revealed slight acanthosis, a moderate lymphocytic infiltrate with exocytosis of lymphocytes and mild epidermal spongiosis, as well as dermal pigmentary incontinence (Fig. 2a). Immuno-histochemical staining revealed an almost complete loss of MART-1- (Fig. 2b) and SOX10-positive melanocytes of the basal epidermal layer. Periodic acid–Schiff (PAS)-staining and serological testing for borreliosis were negative. The patient was diagnosed with vitiligo with inflammatory raised borders and prescribed mometasone furoate ointment locally twice daily for 6 weeks. Narrowband ultraviolet phototherapy was started with a 2-month follow-up.
Vitiligo is an acquired depigmenting skin disorder characterized by circumscribed amelanotic macules and patches. With an estimated prevalence of 0.5–1.0%, vitiligo equally affects both men and women (1). While erythema or itching is usually seen after sun exposure or at the border of early or progressive lesions (2), the clinical variant of vitiligo with raised inflammatory borders (VRIB) is rarely mentioned in dermatological literature and might be under-recognized by clinicians (3).
The first case of VRIB was described by Freudenthal in 1928 (4). Since the patient had a seropositive tertiary syphilis, the author termed the condition as a luetic pseudo-vitiligo. Nearly 20 years later, Garb & Wise (5) recognized the disease as a clinical variant of vitiligo. The lesions mainly appear as depigmented, well-defined patches with a raised erythema at the periphery and can affect any body area (6). Clinical differential diagnoses of VRIB include granuloma annulare, erythema migrans, erythema annulare centrifugum and tinea corporis. Most patients appear to be of Japanese or South Asian origin (2, 6–9). While nearly 20% of patients with vitiligo have at least one comorbid autoimmune disease (10), VRIB has only been described with Sjögren’s syndrome (6, 8). Other associated diseases include atopic dermatitis and hepatitis C infection (7, 9). Therefore, our case adds autoimmune thrombocytopaenia to the range of autoimmune diseases associated with VRIB.
Histopathological analysis shows an infiltration of lymphocytes, histiocytes, and melanophages in the upper dermis with exocytosis of lymphocytes (7). CD4+ T cells have been described in the raised borders and CD8+ T cells outside of the borders (7). The border of the lesion often shows mild spongiosis and liquefaction degeneration of the basal layer (3). While the border shows a diminution of pigment, complete absence of epidermal pigment and melanocytes is usually seen in the depigmented areas (3, 6). On electron microscopy of the inflammatory raised borders intraepidermal lymphocytes are seen in apposition to some melanocytes in the basal layer (2).
Therapy is similar to that of vitiligo vulgaris. While topical corticosteroids have been described to improve the inflammation in the raised border, they failed to induce repigmentation (6). Whole-body narrow-band ultraviolet B (NB-UVB) or psoralen plus UVA (PUVA) with or without oral prednisolone (20–30 mg daily) have been successful in improvement of erythema and repigmentation (6, 8, 9). Although treatment with low-dose systemic steroids can enhance UV-treatment (11), steroid-related side effects ranging from 12% to 69% need to be considered when discussing treatment options with patients (12). Furthermore, high repigmentation rates can be achieved by off-label treatment with Janus kinase inhibitors, such as tofacinitib (13).
Since depigmentation may be difficult to recognize in patients with skin phototype I or II, VRIB might be easily mistaken for other erythematous annular lesions by clinicians. Dermatopathologists may also easily miss the diagnosis if depigmentation is not mentioned by the clinician as histological changes can be similar to eczema or erythema annulare centrifugum and would therefore usually not induce the dermatopathologist to perform immunohisto-chemistry for melanocytic antigens. Since the contrast of Wood’s light examination might not be as distinct in depigmented areas of light-skinned patients, its correlation with clinicopathological findings is therefore important for the correct diagnosis of this rare variant of vitiligo, especially in patients with light complexion.
Fig. 2. (a) Haematoxylin-eosin stained skin biopsy specimen with a moderate perivascular lymphocytic infiltrate and pigmentary incontinence (grey arrowheads). (Scale bar: 100 μm). (b) Immunohistochemical staining of MART-1 in skin biopsy specimen from an elevated erythematous border of a lesion on the right lower abdomen showing paucity of melanocytes. (Scale bar: 100 μm).


 Click to show fullsize
Click to show fullsize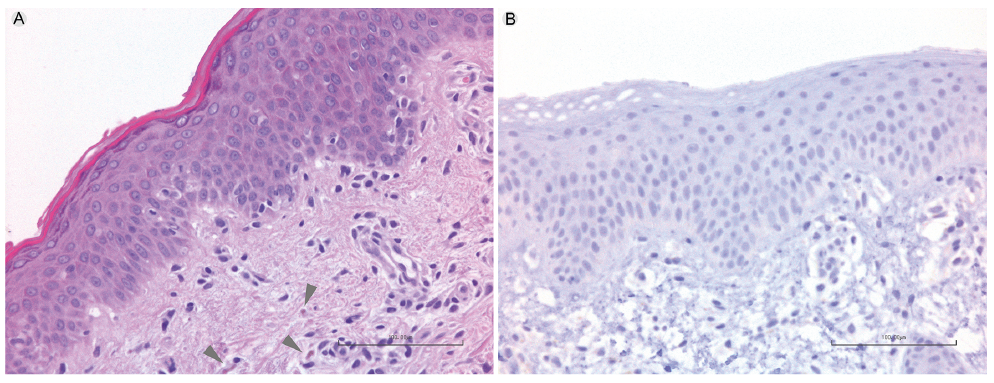 Click to show fullsize
Click to show fullsize