


1Department of Dermatology, University Hospital of Brest, FR-29609 Brest, France, 2LIEN, University of Brest, Brest, 3EMMA, Fontenay-sous-Bois, 4Santé Publique, Hôpital Necker Enfants Malades, Paris, 5Bioderma (Naos Group), Lyon, and 6Department of Dermatology, Hôpital Necker Enfants Malades, Paris, France. E-mail: laurent.misery@chu-brest.fr
Accepted Nov 19, 2019; Epub ahead of print Nov 19, 2019
Acta Derm Venereol 2020; 100: adv00039
According to the special interest group (SIG) on sensitive skin of the International Forum for the Study of Itch (IFSI), sensitive skin is consensually defined (1) as “a syndrome defined by the occurrence of unpleasant sensations (stinging, burning, pain, pruritus, and tingling sensations) in response to stimuli that normally should not provoke such sensations. These unpleasant sensations cannot be explained by lesions attributable to any skin disease. The skin can appear normal or be accompanied by erythema. Sensitive skin can affect all body locations, especially the face”.
Numerous studies have assessed the prevalence of sensitive skin among adults (2). These studies used similar methodologies that were based on surveys of samples of a population aged 15 years and older in accordance with quota sampling. The global prevalence of “sensitive skin” is estimated to be approximately 40%, with potential considerable upward trends in certain countries that may be attributed to genetic or environmental factors but more likely to socio-linguistic factors or cosmetic habits. Indeed, a comparison of 4 studies in the USA suggests that the frequency of sensitive skin might vary from 50 to 85% (3).
Although an increase in frequency with aging has been reported for sensitive scalp (4), there is evidence for a weak decrease in the frequency of sensitive skin with aging (5, 6). To the best of our knowledge, the presence of sensitive skin in children has not been evaluated. The aim of this study was to estimate the prevalence of sensitive skin in children under 6 years of age according to a survey among mothers.
In total, 608 mothers responded. The mean ± SD age was 33.6 ± 5.7 years (31.6 ± 5.7 for mothers with an only child vs 34.8 ± 5.4 for mothers with 2 or more children). Of the sample, 44.6% declared that they were concerned about the skin of their child: 49.6 if they had an only child vs 41.5% in other cases (p = 0.03).
The prevalence of sensitive skin was calculated to be 53.9% based on the declarations of the mothers (girls: 58.2%/boys: 48.7%). Children were considered to have sensitive skin when their mothers reported that they had very sensitive (9.7%) or sensitive (43.6%) skin, whereas they were classified as without sensitive skin if the mothers
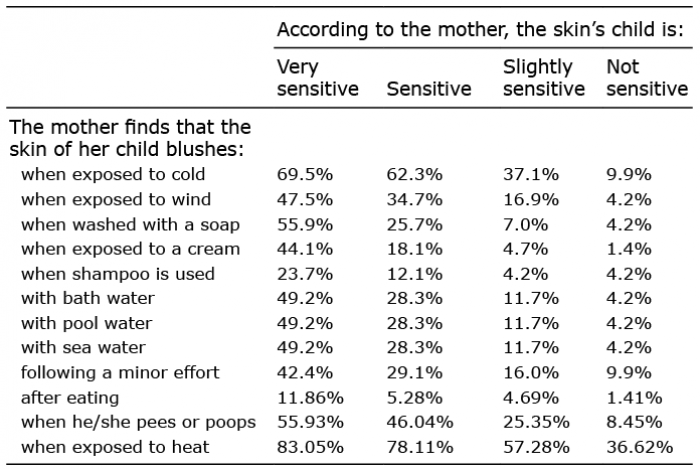
answered that they had no (11.7%) or slightly (35%) sensitive skin. The mothers reported dry skin for 93.2% of the children with very sensitive skin, 54.3% of those with sensitive skin, 15% of those with slightly sensitive skin and 2.9% of those without sensitive skin. The triggering factors of sensitive skin are listed in Table I.
Table I. Triggering factors of skin blushing
The mothers thought that their children suffered from itching in 45.8% of cases with very sensitive skin, 16.6% of those with sensitive skin, 4.2% of those with slightly sensitive skin and 5.6% of those without sensitive skin. Their opinions were 15.3%, 6.4%, 1.4% and 1.4% for tingling or burning sensations in the above categories, respectively, difficulties falling asleep were reported in 42.4%, 31.3%, 17.4% and 22.5% of cases, respectively, and nocturnal wakefulness was observed in 66.1%, 52.3%, 42.7% and 43.7%, respectively.
Regarding themselves, the mothers reported having sensitive skin when their children had very sensitive skin (86.4%), sensitive skin (74.7%), slightly sensitive skin (50.2%) and no sensitive skin (32.4%).
The children were classified in 2 groups: sensitive skin (n = 324) and no sensitive skin (n = 284). According to univariate analysis, the children had sensitive skin (by comparison with the group “no sensitive skin”) if their mother had sensitive skin (76.9% vs 48.9%; p < 0.0001), if they were girls (52.5 vs 43.0%; p = 0.02), if their mother was concerned with their skin (69.5 vs 21.9%; p < 0.0001), if dry skin was reported (636 vs 12.3%; p < 0.0001), if they had an associated skin disorder (60.2 vs 27.8%; p < 0.0001) and if they had nocturnal wakefulness (54.9 vs 43.0%; p = 0.003). Multivariate analysis confirmed these results (p < 0.0001), except for the associated regarding sex difference and nocturnal wakefulness. All triggering factors of skin blushing reported in Table I were significantly associated with the presence of sensitive skin (p < 0.0001), with the exception of blushing after eating, in the univariate analysis. In the multivariate analysis, significant odds ratios, from to 2 to 3, were obtained only for exposure to cold (p < 0.0001), urinating or defecatingactivities (p < 0.0001), exposure to soaps (p = 0.002) and exposure to creams (p = 0.001).
To our knowledge, this is the first study to evaluate the prevalence of sensitive skin in children under 6 years (53.9%), and this prevalence appears to correlate positively with the prevalence in adults (5). It is also notable that sensitive skin is closely related in children and adults: females rather than males, association with skin dryness and same triggering factors. Nonetheless, the induction of blushing due to peeing or pooping activities is probably not a symptom of sensitive but a physiological reaction in these young children.
This study is the first to suggest a hereditary component in sensitive skin: children who have a mother with sensitive skin have an increased risk of experiencing sensitive skin themselves (odds ratio 3.5). Until now, sensitive skin has instead been considered as a consequence of exposure to environmental factors (7). The high frequency of a maternal history of sensitive skin as well as a prevalence of sensitive skin in young children closely aligned to that in adults strongly suggests inherited factors. For example, involvement of the skin nervous system similar to that observed in small-fiber neuropathies (8, 9) is currently the promising pathophysiological hypothesis for sensitive skin. Mutations in SCN9A and SCN10A leading to hyperexcitability of sodium channels Nav1.7 and Nav1.8 in nerve endings are frequently observed in small-fiber neuropathies (10, 11). Although alterations of the skin barrier in sensitive skin are controversial (12), the frequency of dry skin is high in children with sensitive skin, and inherited factors that may be associated with dry skin are numerous. The triggering of sensitive skin by a large variety of factors (physical, chemical or physico-chemical) is likely related to the activation or rather the hyperactivation of proteins, allowing for the identification of multiple environmental factors that might be modified due to genetic variations (13, 14). As an example, microarray studies have demonstrated adiponectin deficiency in sensitive skin (15).
The main limitation of our study is that the diagnosis of sensitive skin was performed by mothers. Currently, there is no tool available for assessing sensitive skin in children, and our methods appear to be the best for an epidemiological approach. However, the higher declared frequency of sensitive skin in children with a mother who is concerned about the skin of her children suggests possible bias. Nonetheless, the strong correlation of positive answers for all questions on triggering factors of redness and unpleasant sensations clearly indicates that the majority of mothers know what sensitive skin is and might provide an adequate diagnosis.
Funding: Bioderma (Naos Group).
Conflict of interest statement: LM: Beiersdorf, Bioderma, Clarins, Expanscience, Johnson&Johnson, L’Oréal, Nestlé Skin Health, Pierre Fabre, Solabia and Uriage. CT is an employee of EMMA. EB: Bioderma. FH: Beiersdorf. CAT has no conflicts of interest to declare. MS is an employee of Bioderma. CB has no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize