


1Research and Development Centre, Sun Pharmaceutical Industries Ltd, Gurgaon, Haryana, India, 2Clinical Pharmacology and Pharmacokinetics, Sun Pharmaceutical Industries Ltd, Gurgaon, Haryana, India and 3Medical Affairs, Sun Pharmaceutical Industries, Inc., Princeton, NJ, USA
Two open-label, crossover studies compared the bioavailability of Micronized-isotretinoin 32 mg and Lidose-isotretinoin 40 mg in healthy adults. In the fed bioequivalence/food-effect study, participants (n = 71) received single doses of fed-state Micronized-isotretinoin 32 mg, fed-state Lidose-isotretinoin 40 mg and fasted-state Micronized-isotretinoin 32 mg. In the fasting study, participants (n = 18) received single doses of fasted-state Micronized-isotretinoin 32 mg and fasted-state Lidose-isotretinoin 40 mg. Bioavailability was assessed by isotretinoin LnAUC0–t, LnAUC0–∞ and LnCmax in blood samples taken pre-dosing and over 96 h post-dosing. The 90% confidence intervals for baseline-adjusted least squares geometric mean ratios for LnAUC0–t, LnAUC0–∞ and LnCmax fell within the 80–125% range for bioequivalence for fed-state Micronized-isotretinoin 32 mg vs. fed-state Lidose-isotretinoin 40 mg. Fasted-state Micronized-isotretinoin 32 mg had ~2 times higher bioavailability than fasted-state Lidose-isotretinoin 40 mg. Food had no effect on the rate and a marginal effect on the extent of absorption of Micronized-isotretinoin 32 mg.
Key words: acne vulgaris; isotretinoin; cross-over studies; bioavailability; healthy volunteers.
Accepted Nov 27, 2019; Epub ahead of print Nov 27, 2019
Acta Derm Venereol 2020; 100: adv00049.
Corr: Jeanett Segal, Medical Affairs, Sun Pharmaceutical Industries, Inc., Princeton, NJ, USA. E-mail: Jeanett.segal@sunpharma.com
For the treatment of acne, Lidose-isotretinoin does not need to be taken with a high-fat meal. Two studies compared the absorption of a novel form of isotretinoin (Micronized-isotretinoin 32 mg) and Lidose-isotretinoin 40 mg in healthy adults following either a fast or a high-fat meal. Absorption of Micronized-isotretinoin 32 mg was superior to Lidose-isotretinoin 40 mg, as demonstrated by the equivalent blood levels achieved when both were taken with food. Under fasted conditions, Micronized-isotretinoin 32 mg was absorbed approximately twice as much as Lidose-isotretinoin 40 mg. Micronized-isotretinoin 32 mg could be an alternative acne therapy without stringent food intake requirements.
Isotretinoin (13-cis retinoic acid) is the gold standard therapy for the treatment of severe nodular acne (1). It is recommended that isotretinoin is administered with a high-fat/high-calorie meal to optimize its bioavailability and efficacy (2, 3). Lidose-isotretinoin (Absorica®; Sun Pharmaceutical Industries, Inc., Princeton, NJ, USA) is a formulation of isotretinoin that is pre-solubilized in a lipid matrix to improve bioavailability via enhanced gastrointestinal absorption (4, 5). The absorption of Lidose-isotretinoin is less dependent on the amount and/or type of food intake than traditional isotretinoin; therefore, this formulation can be taken without regard to meals (5).
A novel capsule formulation of Micronized-isotretinoin 32 mg dispersed in a lipid carrier system has been developed recently (Sun Pharmaceutical Industries, Inc., Cranbury, NJ, USA). Micronized-isotretinoin 32 mg is formulated by adopting an optimized micronization technology that substantially increases the surface area per unit mass of the drug in formulation and hence increases the rate of dissolution and bioavailability of the drug product. Prior fasting and food effect pharmacokinetic studies of both Lidose-isotretinoin and isotretinoin utilized 40 mg doses (5). For exploration of fasting and food effect in this trial, the 32 mg dose of Micronized-isotretinoin was identified as the comparator to the 40 mg dose of Lidose-isotretinoin based on the finding that Micronized-isotretinoin dosed at 0.8 mg/kg would be expected to achieve therapeutic levels similar to Lidose-isotretinoin dosed at 1 mg/kg (data on file, Sun Pharma).
This paper presents the findings from 2 studies in healthy adult participants comparing the bioavailability of Micronized-isotretinoin 32 mg and Lidose-isotretinoin 40 mg under fasted and fed conditions and assessing the effect of food intake on the pharmacokinetic properties of Micronized-isotretinoin 32 mg.
Study design
The pharmacokinetic profile of Micronized-isotretinoin 32 mg was assessed in 2 open-label, randomized, single-dose, cross-over studies: a fed bioequivalence and food-effect study, and a fasting study.
The fed bioequivalence and food-effect study was a multicentre, 3-treatment, 3-period, 6-sequence, crossover study in healthy adult male and female participants that compared the bioavailability of Micronized-isotretinoin 32 mg and Lidose-isotretinoin 40 mg under fed conditions and the bioavailability of Micronized-isotretinoin 32 mg under fasted vs. fed conditions. Participants were randomized to 1 of 6 possible sequences that each included 3 periods of treatment, given in a predefined order. The 3 treatments were as follows: a single dose of Micronized-isotretinoin 32 mg following an overnight fast (defined as no food or beverage intake other than water) of at least 10 h (subsequently referred to as fasted-state Micronized-isotretinoin 32 mg), a single dose of Micronized-isotretinoin 32 mg following a standardized high-fat, high-calorie breakfast (2 fried eggs, 2 rashers of bacon, 4 oz hash browns, 2 slices of buttered toast, and 8 oz whole milk; this Food and Drug Administration (FDA) standard meal contained approximately 150 protein calories, 250 carbohydrate calories, and 500 fat calories) preceded by an overnight fast of at least 10 h (subsequently referred to as fed-state Micronized-isotretinoin 32 mg), and a single dose of Lidose-isotretinoin 40 mg following a standardized high-fat, high-calorie breakfast (as outlined above) preceded by an overnight fast of at least 10 h (subsequently referred to as fed-state Lidose-isotretinoin 40 mg). The interval between dosing was 21 days.
The fasting study was a single-centre, 2-treatment, 2-period, 2-sequence, crossover study that compared the bioavailability of Micronized-isotretinoin 32 mg and Lidose-isotretinoin 40 mg under fasted conditions in healthy adult male participants. Participants were randomized to 1 of 2 possible sequences and received the following 2 treatments: a single dose of Micronized-isotretinoin 32 mg following an overnight fast of at least 10 h (subsequently referred to as fasted-state Micronized-isotretinoin 32 mg) and a single dose of Lidose-isotretinoin 40 mg following an overnight fast of at least 10 h (subsequently referred to as fasted-state Lidose-isotretinoin 40 mg). The interval between dosing was 21 days.
In both studies, blood samples were collected before dosing to establish endogenous isotretinoin levels and then at intervals over the 96 h post-dosing.
The Novum Independent Institutional Review Board approved the study protocols and consent forms and any amendments to these documents. The studies were conducted in accordance with the US Code of Federal Regulations Guidelines for Good Clinical Practice, the International Council for Harmonisation Guidelines for Good Clinical Practice, the Declaration of Helsinki on the ethical conduct of medical research, and the Belmont Report. Written, informed consent was obtained from each patient before their enrolment in the study.
Key inclusion and exclusion criteria
Eligible participants were healthy males (both studies) and females (fed bioequivalence and food-effect study only), who were at least 18 years of age, with a body mass index (BMI) between 18 and 30 kg/m2. Male participants were required to use a reliable form of contraception throughout the study, and female participants were required to be of non-childbearing potential.
Exclusion criteria included a history of allergy or sensitivity to retinoids or vitamin A, a significant history or current evidence of chronic infectious disease system disorders or organ dysfunction, a history or presence of gastrointestinal disease or inflammatory bowel disease, or a history of malabsorption in the previous year, a history (personal or family) of psychiatric disorders in the last 2 years requiring treatment or hospitalization, presence of a medical condition requiring regular treatment with prescription drugs, and a history of excessive alcohol consumption or any drug or alcohol addiction that required treatment during the previous 12 months. Full inclusion and exclusion criteria are shown in Appendix S1.
Endpoints
The primary endpoints of the fed bioequivalence and food-effect study were the relative bioavailability of Micronized-isotretinoin 32 mg compared with Lidose-isotretinoin 40 mg in the fed state and the effect of food on the bioavailability of Micronized-isotretinoin 32 mg. The primary endpoint of the fasting study was the relative bioavailability of Micronized-isotretinoin 32 mg compared with Lidose-isotretinoin 40 mg in the fasted state. Plasma concentrations of isotretinoin were measured by fully-validated liquid chromatography with tandem mass spectrometry (LC-MS-MS). Safety was evaluated by the collection of adverse events, through both solicited and unsolicited means.
Statistical analyses
Sample size calculations determined that 58 participants were required for the fed bioequivalence and food-effect study and 18 participants were required for the fasting study.
The pharmacokinetic and statistical analyses were performed on baseline-adjusted isotretinoin plasma concentrations. Data from participants with some missing data were used if pharmacokinetic parameters could be estimated using the remaining data-points, otherwise data from these participants were excluded from the final analysis.
For all treatments, peak isotretinoin exposure (Cmax) was the observed maximum plasma isotretinoin concentration and time to peak isotretinoin exposure (Tmax) was the collection time at which Cmax was first observed. Area under the plasma concentration-time curve from time 0 to the time of the last measurable isotretinoin concentration (AUC0–t) was calculated by the linear trapezoidal method. Any sample with a missing value was treated as if the sample had not been scheduled for collection. Area under the plasma isotretinoin concentration-time curve from time 0 to infinity (AUC0–∞), the elimination rate constant (Kel), and the time taken for half the initial dose to be eliminated from the body (T1/2) were also calculated.
Analysis of variance (ANOVA) was performed for both studies on natural log- (Ln-)transformed Cmax (LnCmax), AUC0–t (LnAUC0–t) and AUC0–∞ (LnAUC0–∞) for baseline-corrected isotretinoin using SAS® (SAS Institute Inc., Cary, NC, USA) with the general linear model procedure used for the fasting study and a mixed procedure used for the fed bioequivalence and food-effect study. For both studies, ANOVA tested 2 one-sided hypotheses at the α = 0.05 level of significance.
In both studies, sequence effects were tested at the α = 0.10 level of significance against the Type III mean square term for participants within sequence. For the fed bioequivalence and food-effect study, centre effect was tested at the α = 0.05 level of significance against the Type III mean square term for participants nested within centre by sequence. All other main effects were tested against the mean squared error term. Least squares geometric means (LSGM) for the treatments, the differences between adjusted treatment means, and the standard errors associated with these differences were estimated.
For the bioavailability comparison between fed-state Micronized-isotretinoin 32 mg and fed-state Lidose-isotretinoin 40 mg, bioequivalence was determined if the 90% confidence intervals (CIs) on the LSGM Micronized-isotretinoin 32 mg:Lidose-isotretinoin 40 mg ratios for LnAUC0–t, LnAUC0–∞ and LnCmax fell within the range 80.0–125.0%.
Absorption rate in the fasted-state was compared between Micronized-isotretinoin 32 mg and Lidose-isotretinoin 40 mg by post hoc partial area evaluation from time 0 h to Cmax, after Cmax to 12 h, and 12 to 24 h.
Detailed statistical analyses were performed to investigate the centre-by-treatment interaction for the fed bioequivalence and food-effect study. These included examining the potential impact of the following factors: smoking status, sex, race and age. For each of these factors, an ANOVA model was performed on LnAUC0–t, LnAUC0–∞ and LnCmax, including terms for centre, treatment, factor, centre by treatment, centre by factor, and factor by treatment.
Participant disposition
In total, 71 participants were enrolled in the fed bioequivalence and food-effect study. Of these, 64 participants completed at least 2 periods of the study (of which one was Micronized-isotretinoin 32 mg administered under fed conditions) and 61 participants completed all 3 periods. The reasons for discontinuation were voluntary withdrawal (5 participants), positive substance abuse screen (2 participants), non-compliance with breakfast requirements (2 participants) and loss to follow-up (1 participant).
In total, 18 participants were enrolled in the fasting study. All participants completed both periods of the study.
Baseline demographics and clinical characteristics
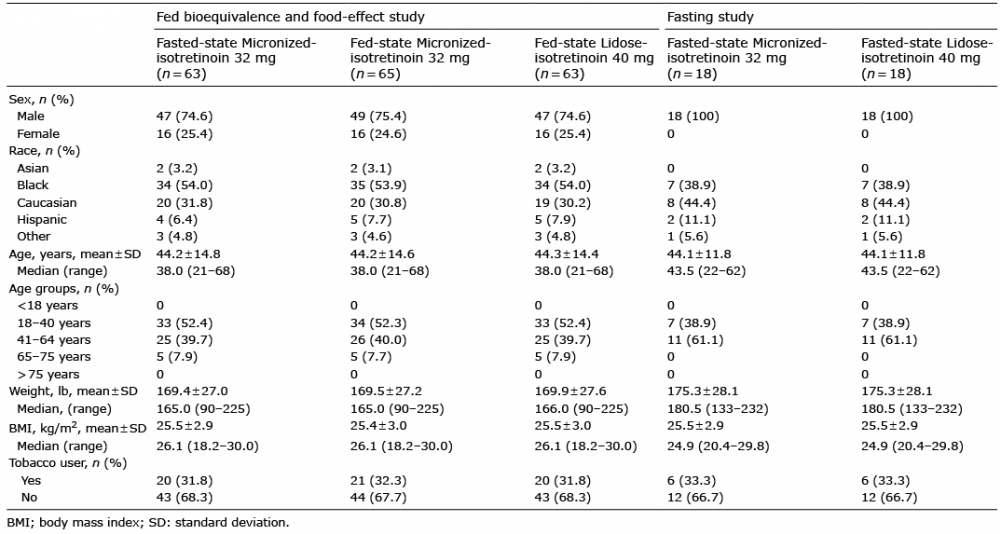
In the fed bioequivalence and food-effect study, participants who received fasted-state Micronized-isotretinoin 32 mg, fed-state Micronized-isotretinoin 32 mg, and fed-state Lidose-isotretinoin 40 mg had comparable demographics, with the majority of participants being male (47 [74.6%], 49 [75.4%], 47 [74.6%]), black (34 [54.0%], 35 [53.9%], 34 [54.0%]), and non-smokers (43 [68.3%], 44 [67.7%], 43 [68.3%]; Table I). The participants had similar mean ± standard deviation (SD) ages (44.2 ± 14.8, 44.2 ± 14.6 and 44.3 ± 14.4 years), mean ± SD body weights (169.4 ± 27.0, 169.5 ± 27.2 and 169.9 ± 27.6 lb), and mean ± SD BMIs (25.5 ± 2.9, 25.4 ± 3.0 and 25.5 ± 3.0 kg/m2).
In the fasting study, the majority of participants were Caucasian (44.4%) and non-smokers (66.7%) (Table I). The participants had a mean ± SD age of 44.1 ± 11.8 years, a mean ± SD body weight of 175.3 ± 28.1 lb and a mean ± SD BMI of 25.5 ± 2.9 kg/m2.
Table I. Demographic characteristics of participants randomized to each treatment group in the fed bioequivalence and food-effect study and the fasting study
Comparative bioavailability of Micronized-isotretinoin 32 mg vs. Lidose-isotretinoin 40 mg under fed conditions (fed bioequivalence and food-effect study)
In total, data from 65 participants were included in the analysis of the bioavailability of Micronized-isotretinoin 32 mg and Lidose-isotretinoin 40 mg under fed conditions. Mean ± SD baseline-adjusted AUC0–t, AUC0–∞ and Cmax parameters were similar for fed-state Micronized-isotretinoin 32 mg and fed-state Lidose-isotretinoin 40 mg (Table II). In addition, there was little difference between fed-state Micronized-isotretinoin 32 mg and fed-state Lidose-isotretinoin 40 mg for mean ± SD Tmax (7.78 ± 4.605 h vs. 7.84 ± 4.377 h), Kel (0.032 ± 0.0092 h–1 vs. 0.031 ± 0.0085 h–1) and T½ (23.52 ± 6.595 h vs. 24.04 ± 7.085 h).
Statistical analysis evaluation confirmed that most of the centre-by-treatment factors did not affect the pharmacokinetic parameters; therefore, data from the 2 treatment centres were pooled to compare the bioequivalence of fed-state Micronized-isotretinoin 32 mg vs. fed-state Lidose-isotretinoin 40 mg for LnAUC0–t, LnAUC0–∞ and LnCmax. The centre-by-treatment effect was dropped from the final statistical model.
Baseline-adjusted LSGMs for LnAUC0–t, LnAUC0–∞ and LnCmax were 9,915 h·ng/ml, 10,654 h·ng/ml and 596.7 ng/ml, respectively, for fed-state Micronized-isotretinoin 32 mg, and 10,430 h·ng/ml, 11,249 h·ng/ml and 573.2 ng/ml, respectively, for fed-state Lidose-isotretinoin 40 mg. Corresponding baseline-adjusted LSGM ratios for LnAUC0–t, LnAUC0–∞ and LnCmax for fed-state Micronized-isotretinoin 32 mg vs. Lidose-isotretinoin 40 mg were 95.1%, 94.7% and 104.1%, respectively.
The 90% CIs for the LSGM ratios for baseline-adjusted LnAUC0–t (91.9–98.4%), LnAUC0–∞ (91.5–98.0%) and LnCmax (96.3–112.6%) for fed-state Micronized-isotretinoin 32 mg vs. fed-state Lidose-isotretinoin 40 mg all fell within the 80.0% to 125.0% range for bioequivalence, showing that Micronized-isotretinoin 32 mg is bioequivalent to Lidose-isotretinoin 40 mg under fed conditions (Table II, Fig. 1).
The sequence effect was not statistically significant for baseline-adjusted LnAUC0–t (p = 0.1327), LnAUC0–∞ (p = 0.1940) or LnCmax (p = 0.4744). Age, race and smoking status did not appear to contribute to the pharmacokinetic profiles of Micronized-isotretinoin 32 mg or Lidose-isotretinoin 40 mg under fed conditions.
Table II. Summary statistics of baseline-adjusted plasma isotretinoin concentrations for fed-state Micronized-isotretinoin 32 mg and fed-state Lidose-isotretinoin 40 mg in the fed bioequivalence and food-effect study (with exclusion of a centre-by-treatment interaction term)
Fig. 1. Mean baseline-adjusted plasma isotretinoin concentration vs. time curves for fasted-state Micronized-isotretinoin 32 mg, fed-state Micronized-isotretinoin 32 mg, and fed-state Lidose-isotretinoin 40 mg in the fed bioequivalence and food-effect study.
Comparative bioavailability of Micronized-isotretinoin 32 mg vs. Lidose-isotretinoin 40 mg under fasted conditions (fasting study)
Data from 18 participants were included in the analysis of the bioavailability of Micronized-isotretinoin 32 mg vs. Lidose-isotretinoin 40 mg under fasted conditions. Mean ± SD baseline-adjusted AUC0–t, AUC0–∞ and Cmax parameters for fasted-state Micronized-isotretinoin
32 mg were nearly double those for fasted-state Lidose-isotretinoin 40 mg (Table III). However, there was little difference between fasted-state Micronized-isotretinoin 32 mg and fasted-state Lidose-isotretinoin 40 mg for mean ± SD Tmax (3.07 ± 1.014 and 2.99 ± 1.521 h), Kel (0.029 ± 0.0061 and 0.028 ± 0.0071 h–1) and T½ (24.59 ± 5.298 and 25.99 ± 7.083 h).
The baseline-adjusted LSGM ratios for fasted-state Micronized-isotretinoin 32 mg vs. fasted-state Lidose-isotretinoin 40 mg for LnAUC0–t (LSGM ratio: 198.6% [90% CI 175.2–225.2%]), LnAUC0–∞ (LSGM ratio: 196.3% [90% CI 172.9–223.0%]) and LnCmax (LSGM ratio: 219.6% [90% CI 187.3–257.6%]) show that Micronized-isotretinoin 32 mg has approximately 2 times higher bioavailability compared with Lidose-isotretinoin 40 mg under fasted conditions (Table III).
Table III. Summary statistics of baseline-adjusted plasma isotretinoin concentrations for fasted-state Micronized-isotretinoin 32 mg and fasted-state Lidose-isotretinoin 40 mg in the fasting study
The sequence effect was not found to be statistically significant for baseline-adjusted LnAUC0–t (p = 0.9168), LnAUC0–∞ (p = 0.7367) or LnCmax (p = 0.4234).
After reaching peak concentration, plasma concentrations of isotretinoin for fasted-state Micronized-isotretinoin 32 mg and fasted-state Lidose-isotretinoin 40 mg declined at the same rate, with isotretinoin levels remaining higher for fasted-state Micronized-isotretinoin 32 mg than for fasted-state Lidose-isotretinoin 40 mg (Fig. 2).
Fasted-state Micronized-isotretinoin 32 mg had a higher rate of absorption compared with fasted-state Lidose-isotretinoin 40 mg. Partial area evaluation indicates that fasted-state Micronized-isotretinoin 32 mg had higher absorption than fasted-state Lidose-isotretinoin 40 mg in each segment from dose to Cmax (LnAUC0–4 LSGM ratio: 164.8%), after Cmax to 12 h (LnAUC4–12 LSGM ratio: 206.1%), and from 12 to 24 h (LnAUC12–24 LSGM ratio: 200.3%).
Fig. 2. Mean baseline-adjusted plasma isotretinoin concentration vs. time curves for fasted-state Micronized-isotretinoin 32 mg and fasted-state Lidose-isotretinoin 40 mg in the fasting study.
Effect of food on the bioavailability of Micronized-isotretinoin 32 mg (fed bioequivalence and food-effect study)
In total, data from 65 participants were included in the analysis of the bioavailability of fed-state Micronized-isotretinoin 32 mg vs. fasted-state Micronized-isotretinoin 32 mg. Mean ± SD baseline-adjusted AUC0–t, AUC0–∞ and Cmax parameters for fasted-state Micronized-isotretinoin 32 mg and fed-state Micronized-isotretinoin 32 mg are shown in Table IV.
Table IV. Summary statistics of baseline-adjusted plasma isotretinoin concentrations for fasted-state Micronized-isotretinoin 32 mg and fed-state Micronized-isotretinoin 32 mg in the fed bioequivalence and food-effect study (with exclusion of a centre-by-treatment interaction term)
The high-fat meal delayed isotretinoin absorption by 1.5 h: median Tmax was 3.5 h for fasted-state Micronized-isotretinoin 32 mg and 5.0 h for fed-state Micronized-isotretinoin 32 mg. Micronized-isotretinoin 32 mg in the fasted state and Micronized-isotretinoin 32 mg in the fed state also had a different mean ± SD Tmax (3.68 ± 1.924 and 7.78 ± 4.605 h), a similar mean ± SD Kel (0.029 ± 0.0083 and 0.032 ± 0.0092 h−1), and a similar mean ± SD T½ (25.50 ± 7.074 and 23.52 ± 6.595 h).
Baseline-adjusted LSGM ratios and corresponding 90% CIs for fed-state Micronized-isotretinoin 32 mg vs. fasted-state Micronized-isotretinoin 32 mg for LnAUC0–t (124.8% [90% CI: 117.3–132.9%), LnAUC0–∞ (123.2% [90% CI: 115.9–131.0%) and LnCmax (108.3% [90% CI: 94.4–124.1%]) showed that administering Micronized-isotretinoin 32 mg with a high-fat meal increased LnAUC0–t and LnAUC0–∞ by 24.8% and 23.2%, respectively, but had no effect on LnCmax compared with administration in the fasted state (Table IV, Fig. 1).
The sequence effect was statistically significant for baseline-adjusted LnAUC0–t (p = 0.0351) and LnAUC0–∞ (p = 0.0600), but not for LnCmax (p = 0.2908). Age, race and smoking status did not appear to contribute to the pharmacokinetic profile of Micronized-isotretinoin 32 mg in either the fasted or fed state.
Safety
In the fed bioequivalence and food-effect study, 68 adverse events were reported by 36 of the 71 participants: 34 occurred after administration of fasted-state Micronized-isotretinoin 32 mg; 16 after fed-state Micronized-isotretinoin 32 mg; and 18 after fed-state Lidose-isotretinoin 40 mg. None of the adverse events were considered serious. The most frequently reported adverse event was headache (fasted-state Micronized-isotretinoin 32 mg: 6 (9.0%) participants; fed-state Micronized-isotretinoin 32 mg: 3 (4.5%) participants; fed-state Lidose-isotretinoin 40 mg: 2 (3.1%) participants).
In the fasting study, 7 adverse events were reported by 4 of the 18 participants: 3 occurred after administration of fasted-state Micronized-isotretinoin 32 mg and 4 after administration of fasted-state Lidose-isotretinoin 40 mg. None of the adverse events were considered serious. The most frequently reported adverse event was oropharyn-geal pain (fasted-state Micronized-isotretinoin 32 mg: 1 (5.6%) participant; fasted-state Lidose-isotretinoin 40 mg: 1 (5.6%) participant).
Results from the fed bioequivalence and food-effect study and the fasted study show that Micronized-isotretinoin 32 mg is bioequivalent to Lidose-isotretinoin 40 mg under fed conditions and has approximately 2 times higher bioavailability compared with Lidose-isotretinoin 40 mg under fasting conditions, meaning that these 2 isotretinoin formulations are not interchangeable and Micronized-isotretinoin 32 mg will be given a BX rating by the FDA. Micronization plays a key role in dose reduction because, with reduced particle size, Micronized-isotretinoin 32 mg achieves similar plasma levels to Lidose-isotretinoin 40 mg in the fed state with a 20% lower dose.
Administering Micronized-isotretinoin 32 mg with a high-fat meal resulted in an approximately 1.2-fold increase in LnAUC0–t and LnAUC0–∞, but had no effect on LnCmax compared with when Micronized-isotretinoin 32 mg was taken under a fasting state, indicating that food has no effect on the rate and a marginal effect on the extent of Micronized-isotretinoin 32 mg absorption. This is in contrast to the effect of food on the absorption of Lidose-isotretinoin 40 mg. LnAUC0–t and LnCmax for Lidose-isotretinoin 40 mg have been shown to be approximately 1.5- and 1.3-fold higher, respectively, under fed-state conditions compared with fasted-state conditions, indicating that Lidose-isotretinoin 40 mg has a food effect for both rate and extent of absorption (4). Micronization and the presence of a lipidic carrier system play a combined role in the reduced food effect observed for Micronized-isotretinoin 32 mg. These 2 factors increase the dissolution and bioavailability of Micronized-isotretinoin 32 mg, which is reflected by increased absorption in the fasted state.
The sequence effects for the LSGM ratios for baseline-adjusted LnAUC0–t and LnAUC0–∞ for fed-state Micronized-isotretinoin 32 mg vs. fed-state Lidose-isotretinoin 40 mg were significant. This may be due to the AUCs for these 2 formulations being affected differently by food, resulting in different error values being generated by the ANOVA statistical model when data are segregated according to sequence.
Comparable, or even improved, bioavailability between fasted-state Micronized-isotretinoin 32 mg and either traditional non-Lidose forms of isotretinoin or Lidose-isotretinoin in the fed state could represent an advantage for Micronized-isotretinoin 32 mg. Dose-ranging trials involving traditional non-Lidose isotretinoin demonstrate no difference in on-treatment efficacy for 0.1, 0.5 and 1.0 mg/kg/day of isotretinoin, yet a clear dose response is observed when examining the rate of relapse after a single course of therapy has been completed (6). In addition, numerous studies have reported that cumulative doses below a threshold (i.e. <120 mg/kg) are associated with relapse and repeated treatment (6–8). This suggests that there may be a minimum “effective” dose. An effective dose may reflect serum levels of sufficient value and duration to produce a prolonged treatment affect after treatment cessation. Therefore, the enhanced bioavailability of Micronized-isotretinoin 32 mg means that this formulation could provide the same on-treatment efficacy as Lidose-isotretinoin 40 mg or traditional forms of isotretinoin and lower rates of relapse upon completion of a single course of therapy. Clearly, a caveat is the need for future studies to be undertaken to help clarify more precisely if there is a threshold tissue exposure and duration of that exposure required to achieve lasting relapse-free/re-treatment-free outcomes for patients with acne, given the polymorphic presentation of the disease and the range of factors, endocrine and otherwise, that may be implicated in the onset, severity, distribution and risk of recurrence.
Both Micronized-isotretinoin 32 mg and Lidose-isotretinoin 40 mg were well tolerated, and no serious adverse events were reported for either formulation.
Micronized-isotretinoin 32 mg administration produces consistent serum levels irrespective of gastrointestinal contents, and thus relieves the patient from planning doses around co-administration of food to a greater extent than all preceding isotretinoin formulations. This lack of stringent dietary requirements could increase compliance, as young adults and teenagers (the most common recipients of acne therapy) are known for their poor and irregular eating habits (9). Busy adults can also have inconsistent eating habits that have to fit around varying schedules, indicating that an efficacious acne treatment that is not dependent on food intake could also be beneficial in this patient population (10).
The authors would like to thank the participants who took part in this study. Editorial support was provided by Tamsin Brown, MSc, JK Associates, Inc., part of the Fishawack Group of Companies, and was funded by Sun Pharmaceutical Industries, Inc. Statistical support was provided by Novum Pharmaceutical Research Services, Inc., and was funded by Sun Pharmaceutical Industries, Inc.
The studies were funded by Sun Pharmaceutical Industries Ltd, Gurgaon, Haryana, India.
SM and SK are employees of Sun Pharmaceutical Industries Ltd. JS is an employee of Sun Pharmaceutical Industries, Inc.


 Click to show fullsize
Click to show fullsize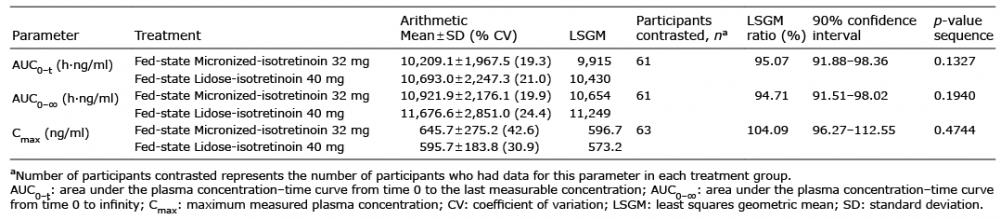 Click to show fullsize
Click to show fullsize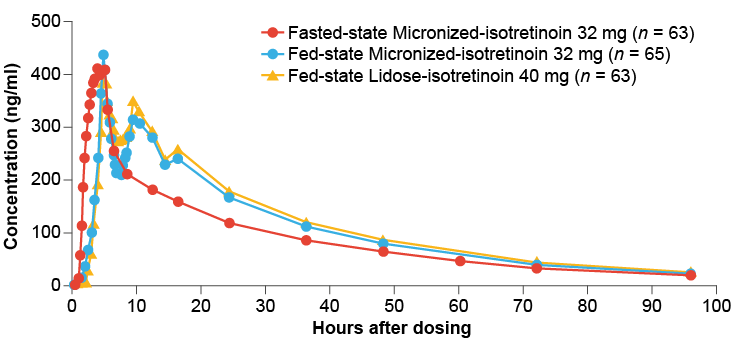 Click to show fullsize
Click to show fullsize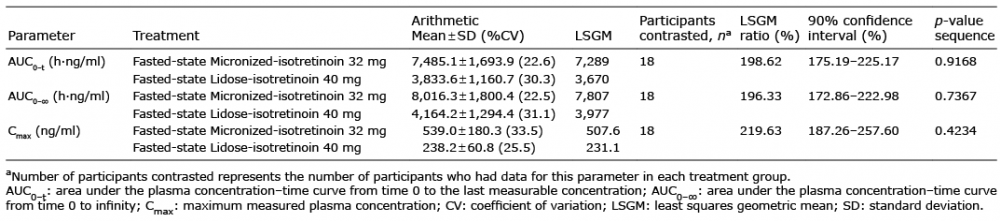 Click to show fullsize
Click to show fullsize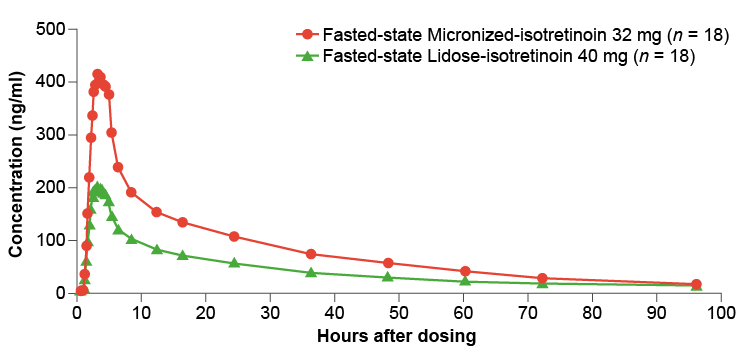 Click to show fullsize
Click to show fullsize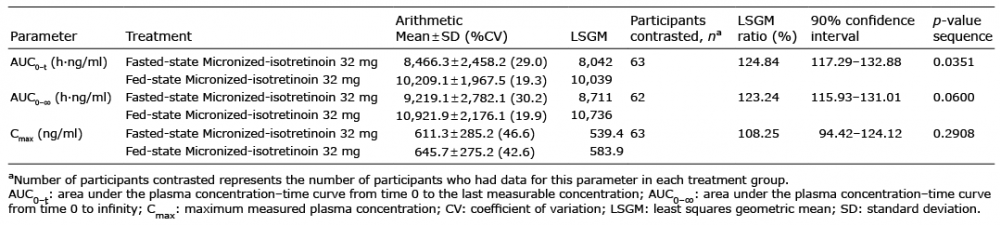 Click to show fullsize
Click to show fullsize