


Shandong Provincial Hospital for Skin Diseases & Shandong Provincial Institute of Dermatology and Venereology, Shandong First Medical University & Shandong Academy of Medical Sciences, 27397 Jingshi Road, Jinan, Shandong Province, 250022, China. *E-mail: zhangfuren@hotmail.com
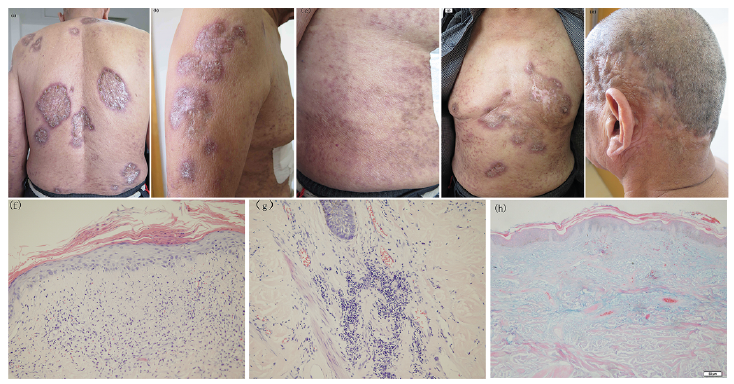
A 74-year-old man presented to the Department of Dermatology at our hospital with a 30-year history of a widespread pruritic patch. Physical examination revealed variegated brown and red patches of different sizes on his arms, abdomen and legs, and keloid-like plaques on his trunk and arms. The patches had a bulge at the edge and atrophy in the centre. The peripheral lesions were many purplish macules or papules. The scalp had an atrophic plaque and hair loss (Fig. 1A and E). He felt itching and had been diagnosed with eczema and keloids in a local clinic in the last 10 years. There were no systemic symptoms. Laboratory tests, including blood cell counts, urea, and liver function, were normal. Electrocardiogram, chest X-ray, and abdominal ultrasound examinations indicated no cardiac, pulmonary, hepatic, splenic, or nephritic abnormalities. A biopsy sample from the abdominal lesion showed hyperkeratosis, keratinization, basal cell liquefaction and degeneration, superficial and deep dermal vessels, and hair follicles infiltrated with peripheral lymphocytes, tissue cells (Fig. 1F and G).
What is your diagnosis? See next page for answer.
Fig. 1. (a) Atrophic patch on the back. (b) Mild protuberant plaque on the arm. (c) Purplish macules or papules on the abdomen. (d) Atrophic patches and keloid-like plaques on the abdomen. (e) Scarring alopecia in the scalp. (f) Hyperkeratosis, keratinization, basal cell liquefaction and degeneration (haematoxylin and eosin (H&E) staining, ×200). (g) Superficial and deep dermal vessels, hair follicles, peripheral lymphocytes, tissue cells (H&E staining, ×200). (h) Positive Alcian blue staining, ×100.
Acta Derm Venereol 2020; 100: adv00050.
Diagnosis: Discoid lupus erythematosus
Alcian blue staining of the skin biopsy was positive, which demonstrated that the deposition of mucin in the derma (Fig. 1H). The pathology indicated the probability of connective tissue disease. Additional serum immunological examination was performed and laboratory tests were positive for Ro-52 antibodies, centromere protein B antibody, and ribonucleoprotein antibody. Antinuclear antibody titre was 1:1000. The patient had not experienced any fever, arthralgia, oral ulcers, or Raynaud’s phenomenon in the past 30 years. Based on the clinical features, the pathology and laboratory tests, a diagnosis of discoid lupus erythematosus (DLE) was supported. Hydroxychloroquine, 0.2 g/day, was prescribed. After 30 days’ treatment, there was no change in the lesions. Prednisone, 30 mg/day, was then given. Two months later, some of the lesions had disappeared. The patient currently takes prednisone, 5 mg/day.
In humans the most common clinical subtype of chronic cutaneous lupus erythematosus is so-called DLE, which can be either localized or generalized. Generalized DLE is a rare condition. Although most patients presenting with DLE lesions never develop features of clinically significant systemic lupus erythematosus, this is somewhat more likely to occur in patients presenting with generalized DLE (1). This patient had undergone mild clinical course without developing severe systemic organ manifestations during a 30-year period.
Long-term follow-up patients with chronic cutaneous lupus erythematosus has shown scarring of some kind, producing destruction and deformity, such as scarring alopecia, cribriform scarring, atrophie blanche, and even squamous cell carcinomas (2). For the current patient, one of the initial clinical diagnoses was keloid, due to bumps on the trunk and arms. To our knowledge, widespread lesions, presenting as patches, bumps, purplish macules or papules, have not been reported previously in DLE in the English and Chinese literature.
The authors thank the individuals who participated in this project. This work was funded by grants from the Natural Science Foundation of Shandong Province (ZR2015YL025).


 Click to show fullsize
Click to show fullsize