


Department of Dermatology, Ajou University School of Medicine, Suwon 16499, Korea. E-mail: esl@ajou.ac.kr
Accepted Dec 12, 2019; Epub ahead of print Dec 18, 2019
Acta Derm Venereol 2020; 100: adv00058
Psoriasis is a chronic inflammatory skin disorder, which is mainly mediated by T cells (1, 2). Plasmacytoid dendritic cells have been shown to play a major role in the initial stage of the disease (3, 4), and growing evidence suggests T-helper 17 cells (Th17) and CD4+CD25+ regulatory T (Treg) cells as the cause of psoriasis (1, 5–7). In addition, the inflammatory milieu activates keratinocyte proliferation via tumour necrosis factor (TNF)-α, interleukin (IL)-17, and interferon (IFN)-γ (8); thus, the TNF-α–IL-23–Th17 axis plays a central role in T-cell-mediated plaque psoriasis (9). Based on these findings, successful treatments are being conducted in adults using biologics targeting the cytokines secreted by these immune cells (10).
Although psoriasis is a relatively common disease in children, research into paediatric pathogenesis has not been carried out as actively as in adults, and the use of biologics has not been well founded in children (11, 12). Therefore, we investigated the differences in major inflammatory cell types and the cytokine milieu between adult and paediatric psoriatic patients.
This study retrospectively evaluated the electronic medical records and skin biopsy specimens of paediatric (not more than 20 years old) and adult patients diagnosed with psoriasis who visited Ajou University Hospital and underwent skin biopsy between January 2010 and June 2017. Clinical types of psoriasis were classified as plaque, guttate, or pustular type. A final total of 22 paediatric patients and 25 clinical type-matched adult patients were enrolled in the study. All skin biopsy specimens were independently examined by 2 dermatologists using immunohistochemical staining for anti-CD3, CD4, CD8, CD45, IL-13a, IL-17a, IL-22, TNF-α, IFN-γ, and FOXP3 antibodies. Both qualitative and quantitative analyses were performed on a representative area of each specimen, and the amount of positive antibody area was measured under the same magnification (×100). Full details of the Materials and Methods are given in Appendix SI. The study protocol was approved by the Ajou Institutional Review Board (IRB No.: AJIRB-BMR-MDB-15-341) prior to study commencement.
The demographic and clinical characteristics of the study population are shown in Table SI. There was no significant difference in sex, first-degree family history of psoriasis, past medical history, serum vitamin D and anti-streptolysin O titre level between paediatric and adult groups. The most common clinical type was plaque psoriasis, and the median age of the paediatric patients was 15 years and that of the adult patients 39 years. In addition, there was no significant difference in mean disease duration of the paediatric (4.24 years) and adult (3.77 years) patients.
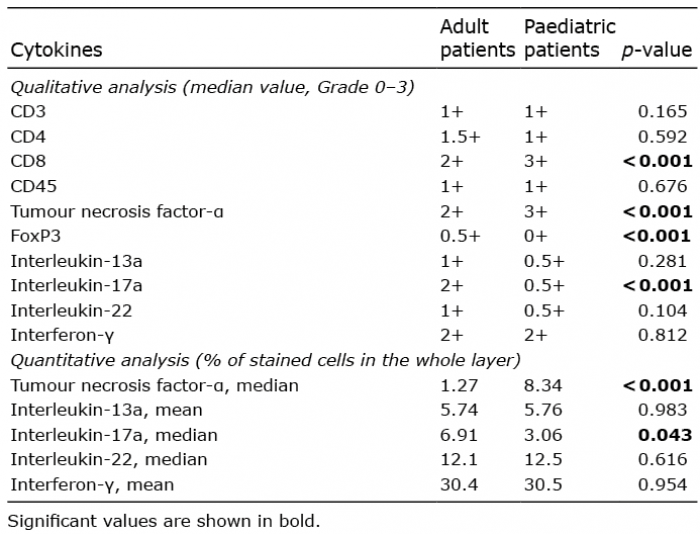
Furthermore, the results of qualitative and quantitative analyses for T-cell surface molecules and intracellular proinflammatory cytokine production are shown in Table I. Qualitative analysis revealed that the staining grades for CD8 and TNF-α in paediatric patients were significantly higher (p < 0.001 and p < 0.001, respectively), but those of FOXP3 and IL-17a were found to be significantly lower (p < 0.001 and p < 0.001, respectively), compared with those in adult patients. However, there was no statistically significant difference in the grade of CD3, CD4, CD45, IL-13a, IL-22, and IFN-γ between groups. Quantitative analysis revealed that paediatric psoriatic skin expressed significantly higher levels of TNF-α (p < 0.001) and lower levels of IL-17a (p = 0.043) compared with adult psoriatic skin (Fig. S1), and these cytokine levels were not related to disease duration in both groups (data not shown). How-ever, the other cytokines showed no statistically significant difference between the 2 groups. Representative images of the histopathological staining are shown in Fig. S2.
Subgroup analysis according to the clinical type of psoriasis was also performed to investigate potential associations with intracellular proinflammatory cytokines found to be significantly differentially expressed through quantitative analysis (Table SII). In plaque- and guttate-type paediatric psoriasis, TNF-α levels were found to be significantly higher in both qualitative and quantitative analyses compared with those in adult psoriasis. However, in pustular-type psoriasis, there was no significant difference in cytokine levels.
Table I. Mean production values of cytokines in lesional skin of adult and paediatric psoriasis patients
This study showed that paediatric patients with psoriasis have significantly increased TNF-α and decreased IL-17 levels compared with adult psoriatic patients, regardless of disease duration. Anti-TNF-α agents are currently used in the treatment of paediatric psoriasis. Etanercept is known to be efficacious and safe as an initial treatment in paediatric psoriasis (13). In addition, adalimumab is commonly used to treat paediatric psoriasis (14). These findings support our results and the importance of TNF-α as a therapeutic target in paediatric psoriasis. In contrast to TNF-α, there are limited studies that have used IL-17 as a target or demonstrated the therapeutic effect of anti-IL-17 agents in paediatric patients. However, some recent studies have shown that IL-17 could be an important therapeutic target in paediatric psoriasis. Zhang et al. revealed that an increased number of circulating Th17 and Treg cells was associated with disease severity in paediatric psoriasis (15). In other previous studies, significant differences in IL-17 expression were observed in paediatric psoriasis patients compared with healthy paediatric controls; however, this difference was less pronounced compared with that between paediatric psoriasis patients and adult psoriatic patients (11), as shown in our results. In the current study, it is unclear whether IL-17 expression is increased or unchanged compared with the normal control group; yet, increased expression could be expected due to the increased expression of IL-17 in paediatric patients compared with healthy controls. Therefore, based on these findings, it could be hypothesized that paediatric psoriasis might respond well to both anti-TNF-α and anti-IL-17 biologic therapies. However, TNF-α may play a greater role in the pathogenesis of paediatric psoriasis and, thus, is a more effective therapeutic target.
The main limitations of this study are the small sample size, and that the effect of disease severity (Psoriasis Area and Severity Index; PASI) on each cytokine level was not taken into account. In addition, there was recall bias for disease onset time and underlying disease, because this study was performed by a retrospective review of medical records. As such, the demographic and clinical characteristics of the study population may have served as confounding factors for statistical analysis.
In conclusion, this study revealed that there were significant differences in TNF-α and IL-17 expression between paediatric and adult psoriasis patients. Specifically, TNF-α levels were significantly increased and IL-17 levels were significantly decreased in paediatric psoriasis patients compared with those in adult psoriatic patients. These findings suggest that immunophenotypic differences can be an important factor for determining clinical characteristics in paediatric and adult psoriasis. In addition, these results provide further evidence that TNF-α is a more important proinflammatory cytokine in paediatric psoriasis compared with adult psoriasis. Taken together, these findings may be used as a guide for the targeted therapy of paediatric psoriasis.
This study was supported by grant from Korea Health Technology R&D programme thorough the Korea Health Industry Development Institute (KHIDI), funded by the ministry of Health and Welfare, Republic of Korea (HI16C0992).
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize