


1Department of Dermatology and Allergy, School of Medicine, Technical University of Munich, Biedersteiner Str. 29, DE-80802 Munich, and 2Chair of Zoology, Entomology, Technical University of Munich, Freising, Germany. E-mail: alexander.zink@tum.de
Accepted Jan 9, 2020; Epub ahead of print Jan 14, 2020
Acta Derm Venereol 2020; 100: adv00067
Spider bites, also know as arachnidism, are rare and in daily clinical practice many suspected cases are eventually caused by other conditions. Most verified spider bites, however, result in mild symptoms. Rarely, they are serious with severe pain and even necrotic wounds. Typically, the spider is not caught in either case, making identification and verification impossible. We present a case of necrotic arachnidism with exploration of the culprit spider.
Two weeks prior to admission to our department, a 30-year-old, otherwise healthy, woman reported being woken up due to painful skin lesions on both feet. The previous day she had returned to Munich, Germany, from a 5-day hiking holiday in South Tyrol, Italy. Over the next few days the lesions became bullous, with significant surrounding erythema and oedema, and significant pain. The patient also had general symptoms of pronounced nocturnal sweating and intermittent “blurred vision”. Antiseptic and anti-inflammatory treatments prescribed by her GP had had no effect; hence the patient was referred to our hospital. She had no personal history of any skin disease and the only medications she was taking were thyroxine due to hypo-thyroidism and oral contraceptives.
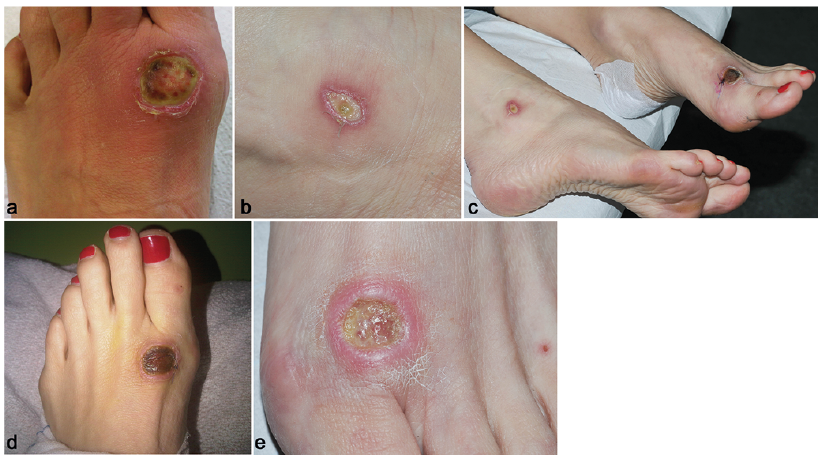
On admission the patient presented an ulceration, approximately 4 cm in diameter, with yellowish adherent coatings and necrotic parts surrounded by significant erythema on the left foot with massive oedematous swelling. On her right foot she had an oval 2×1-cm ulceration with yellowish deposits and a reddish livid border (Fig. 1a–c).
Fig. 1. Skin lesions. On (a) left and (b) right foot, photographed by the patient prior to presentation at our hospital. (c) Both feet and (d) left foot at initial presentation to our clinic. (e) Left foot after 4 weeks of treatment.
Laboratory examinations yielded normal blood and differential blood count, coagulation parameters, serum chemistry including C-reactive protein (CRP) and electrophoresis. Antinuclear antibodies, cardiolipin- and β2-glycopene-antibodies were negative. There were no signs of cryoglobulinaemia. An X-ray of 2 levels of the left foot revealed no signs of osteolysis, osteodestruction or any other abnormal finding. Microbiological analysis of the ulcers revealed abundant Pseudomonas aeruginosa. Dermatohistopathology of a punch biopsy of the ulcer on the left foot revealed ulceration with associated degenerated connective tissue, interspersed with many neutrophilic, focal also eosinophilic granulocytes, and less dense infiltrate of lymphocytes and histiocytes, with no signs of malignancy.
Considering the ineffective topical and oral anti-inflammatory and antibiotic treatment, the patient was treated intravenously with piperacilling/tazobatam 2 g/0.25 g (Fresenius Kabi Deutschland GmbH, Bad Homburg, Germany) combined with prednisolone for 7 days, together with topical treatment with povidone iodine gauze and sterile wound dressings. During treatment, medical maggots (Lucilia sericata) were applied to the necrotic ulcers 3 times on both feet. However, the maggots died rapidly (within a few hours) despite meticulous efforts to provide an ideal environment as described in the manufacturer’s instructions (BioMonde GmbH, Barsbüttel, Germany). Surgical wound debridement was performed several times by subsequent application of a vacuum suction of 125 mmHg followed by sodiumbituminosulfonate gel (Cordes, Hermanni & Co. (GmbH & Co.) KG), which resulted in a slow improvement in the skin lesions (Fig. 1d–e) and complete healing within 13 weeks, with pronounced scarring.
The diagnosis of toxic ulceration following a spider bite, secondarily infected with P. aeruginosa, was made on the basis of clinical symptoms and typical dermatohistological (1) and microbiological findings, but only after repeated and extensive history-taking. The patient reported seeing an unusual spider in her bedroom on the day of onset of the skin lesions. A spider (Fig. 2) was subsequently found in the bedroom by a pest control professional. The spider belongs to the genus Dysdera (Arachnida: Araneae: Dysderidae), but the species was not identified due to poor preservation of the specimen. Spider toxins are still under investigation, but myelinases leading to necrosis and an influx of neutrophils due to chemotactic toxins may cause local vasculitis and necrosis (2). Although Dysdera spiders have been reported as usually rather harmless (3), there is no other reasonable explanation for the systemic reactions observed by our patient, such as night sweats and blurred vision, following exclusion of several differential diagnoses, as suggested recently by Stoecker et al. (4).
There are only a few published cases of necrotic arachnidism with distinct identification of the culprit spider in Europe, and, worldwide, only a very small proportion of spiders have so far been identified to induce necrotic ulcers (2, 5, 6). Therapeutic strategies therefore remain speculative and empirical. Consequent wound care, with local wound debridement, prophylaxis of possible superinfections, and stimulation of granulation as supportive measures, are currently the best strategy (2, 7).
Fig. 2. Spider found in the patient’s bedroom in her 6th-floor apartment in Munich, Germany, possibly transported in a suitcase from South Tyrol, Italy after a hiking holiday. Scale: > 1 mm.


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize