


1Department of Operative and Restorative Dentistry and 2Division of Human Genetics, Medical University Innsbruck, Innsbruck, Austria, 3Department of Dermatology, Chelsea & Westminster Hospital NHS Foundation Trust, London, and 4EDS Syndrome National Diagnostic Service, Northwick Park Hospital, Harrow, UK
Ehlers-Danlos syndromes (EDS) are a group of inherited connective tissue disorders characterized by joint hypermobility, skin hyperextensibility, and variable tissue fragility. However, there are limited published data on the dental manifestations of EDS. This review systematically assessed the spectrum of published dental anomalies in various types of EDS. Twenty-four individual case reports/series and 3 longer case-control studies, reporting on a total of 84 individuals with a clinical diagnosis of EDS, were included in the data analysis. The main dental features listed in classical EDS were pulp calcification and localized root hypoplasia. Common dental abnormalities observed in vascular EDS were pulp shape modifications (52.2%), exceeding root length (34.8%), and molar root fusion (47.8%). Dentinogenesis imperfecta is a consistent finding in osteogenesis imperfecta/EDS overlap syndrome. Data on dental manifestations in other types of EDS are both rare and generally inconclusive.
Key words: Ehlers-Danlos syndromes; hypermobility; oral manifestation; dental anomaly.
Accepted Feb 12, 2020; Epub ahead of print Mar 9, 2020
Acta Derm Venereol 2020; 100: adv00092.
Corr: Johannes Zschocke, Division of Human Genetics, Medical University of Innsbruck, Peter-Mayr-Straße 1, AT-6020 Innsbruck, Austria. E-mail: johannes.zschocke@i-med.ac.at
Ehlers-Danlos syndromes are a group of rare inherited connective tissue diseases. In general, dental problems in Ehlers-Danlos syndromes are minor compared with the serious systemic manifestations, such as complications of generalized joint hypermobility or life-threatening events (e.g. vascular and organ ruptures). Nevertheless, dental problems can severely impact on patients’ quality of life. In order to clarify the range of dental manifestations in Ehlers-Danlos syndromes, and create precise disease-specific information for medical and dental practitioners, a systematic search of the medical literature for relevant reports was carried out.
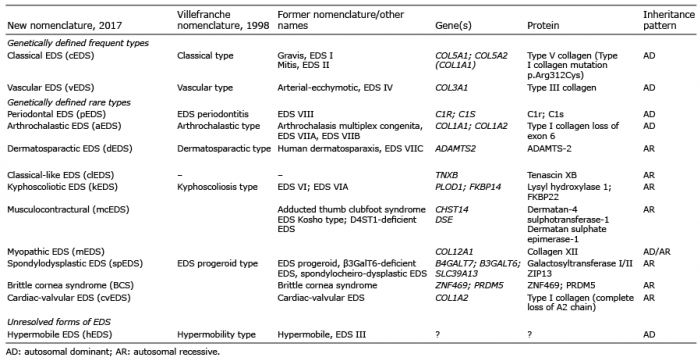
Ehlers-Danlos syndromes (EDS) are a clinically and genetically heterogeneous group of hereditary connective tissue disorders characterized by variable connective tissue fragility, mainly affecting skin, ligaments, blood vessels, and internal organs. The current classification recognizes 13 distinct types of EDS (Table I) (1), 12 of which are monogenic, with known genes that allow diagnostic confirmation. Most types of EDS are caused by disease-causing variants (mutations) in collagen-encoding genes or in genes encoding collagen-modifying enzymes (1).
Table I. Present and past clinical classifications of Ehlers-Danlos syndromes (EDS), inheritance pattern and genetic basis
The biology of dental tissues implies that tooth abnormalities might occur in various types of EDS (Fig. 1). Enamel is an epithelially derived and highly (approximately 96%) mineralized tissue with traces of non-collagenous organic material (2). Recent biochemical studies have found that enamel contains low amounts of collagen I and VII (3, 4). Immunofluorescence studies have localized type VII collagen to the organic matrix near the dentino-enamel junction, suggesting a role of collagen VII in bonding enamel to dentine (4). Animal studies have revealed that proteoglycans control early stages of tooth formation (5). They promote dentine formation and mineralization, but also restrain amelogenin synthesis and consequently enamel formation.
Fig. 1. The tooth and its supporting tissues. The biology of dental tissues implies that tooth abnormalities might occur in various subtypes of Ehlers-Danlos syndrome.
Dentine is a mineralized tissue composed of approximately 70% hydroxyapatite crystals embedded in a 3-dimensional collagenous network. The organic matrix is enriched in type I collagen with traces of type III and V collagen, associated with non-collagenous proteins and proteoglycans. Histological studies have revealed a network of dentinal tubules crossing the mineralized tissue and extending through the entire thickness of the dentine, from the dentino-enamel junction to the pulp (6). These tubules harbour odontoblast cell processes and tissue fluid. Electron microscopic studies have investigated the assembly of the collagenous matrix prior to mineralization, a key step in the formation of dentine (7, 8). During tooth development, odontoblasts secrete collagen fibrils with high concentrations of non-collagenous proteins (9) and proteoglycans (10). These matrix constituents regulate the process of mineral deposition (8).
The dental pulp is a loose connective tissue characterized by its specific anatomical location (11). Various types of collagens were isolated by differential salt precipitation and extraction. Types I, III and V collagen represented 56%, 41% and 2% of the total collagen, respectively (12).
The periodontal ligament belongs to the tooth-supporting tissues and anchors the tooth root to the alveolar bone. It is a highly specialized connective tissue and contains well-defined collagen fibre bundles embedded in ground substance – predominantly collagen types I, III and XII (2). Acellular root cementum is a mineralized hard connective tissue that anchors the periodontal ligament fibres to the tooth root. Its main function is tooth attachment. The cellular cementum covers the apical root and adapts to mechanical loading. Cementum consists of approximately 50% inorganic hydroxyapatite. Collagen (mainly type I with traces of type III and XII) and non-collagenous proteins, including several proteoglycans, form the organic matrix.
Patients with EDS often have a low oral health-related quality of life due to physical pain, psychological discomfort, and handicap (13). A questionnaire study among a large group of adults with EDS, mostly hypermobile or unspecified types of EDS (n = 144), revealed a high prevalence of oral problems, including pain in the masticatory muscles, periodontal disease, spontaneous fractures of teeth and complicated tooth extractions (14). Although EDS-related dental problems may appear less relevant in comparison with severe, sometimes life-threatening, systemic manifestations, they can strongly impact on quality of life. Major issues include pain during oral hygiene procedures, time-consuming dental treatments, and impaired cosmetic appearance. Dental health professionals are often overwhelmed with the medical care of individuals affected by rare diseases; the general dentist may not be familiar with special requirements or disease-specific oral symptoms, and treatment guidelines and precise disease-specific information are currently lacking. The complexities of EDS complications are difficult to handle in general dental practice and vary considerably among individual types of EDS. In 2017 we reviewed periodontal manifestations of EDS (15).
The aim of the present study was to systematically assess manifestations of dental tissues (dentine, enamel, cementum, and pulp) in various types of EDS. This approach allows the delineation of dental anomalies in specific types of EDS, with clinical implications for practicing clinicians.
Protocol and registration
A systematic literature search was performed according to Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) guidelines (16) and was registered at PROSPERO.
Literature search strategy
Two authors (IK, DS) systematically searched the literature up to 1 April 2019 in the following electronic databases: Medline (PubMed), LIVIVO, and Google Scholar. Medline (PubMed) was searched with the following keywords: (“Ehlers-Danlos syndrome” OR “joint hypermobility” OR JHS OR BJHS) AND (“dental abnormalities” OR “dental abnormality” “dental anomalies” OR “dental anomaly” OR “pulp stones” OR “hypercementosis” OR “tooth colour” OR “tooth color” OR “root deformities” OR microdontia OR transposition OR “supernumerary teeth” OR enamel OR dentine OR dentinogenesis). In addition, grey literature (www.opengrey.eu) was browsed and a “manual search” was performed on the reference lists of the selected articles and identified reviews.
Screening and selection
The inclusion criteria applied during the literature search were: (i) population: individuals affected with any type of EDS; (ii) outcome: dental anomalies (enamel, dentine, cementum or the pulp); (iii) English, German, or Italian language; (iv) full text available. There were no restrictions on publication date (available data from 1969 to 2019). Clinical trials, case-control studies, cross-sectional studies, cohort studies, case series, and case reports published in peer-reviewed scientific journals were included. Exclusion criteria were: cell culture laboratory studies, animal studies, and reviews. Titles and abstracts were checked with regard to the listed criteria. Abstracts with unclear methodology were included in full-text assessment to avoid exclusion of potentially relevant articles. Discrepancies detected during the selection process were discussed regularly.
Assessment of heterogeneity
The heterogeneity of the included studies was evaluated based on following factors: (i) study design, and (ii) subjects’ characteristics.
Quality assessment
Quality assessment tools for case series and case-control studies were available from the National Heart, Blood, and Lung Institute (Bethesda, MD, USA) (17). Quality assessment of case reports was performed according to the Joanna Briggs Institute (Adelaide, Australia) (18). Each study was classified into the following groups: low risk of bias if all quality criteria were judged as “present”, moderate risk of bias if one or more key domains were “unclear”, and high risk of bias if one or more key domains were “absent”.
Data extraction
The following main outcome(s) were individually extracted: (i) EDS subtype; (ii) type of dental manifestation(s). The following secondary outcomes were extracted for each individual as available: (iii) clinical characteristics of dental manifestations; (iv) clinical and/or genetic diagnosis of EDS; (v) EDS-specific features. Types and prevalence of dental manifestations and clinical characteristics available on the subjects level were analysed by standard descriptive measures, such as absolute and relative frequencies of dental manifestations in the present cohort.
The article selection process is documented in Fig. 2. Out of a total of 106 studies identified originally, 59 were excluded based on title and abstract. Of these, 45 did not report on either EDS or tooth anomalies, or covered other dental aspects in patients with EDS, such as dental implants, temporomandibular joint disorders, periodontal disease, mucosal alterations and aberrant frenula, or non-specific oral treatments, such as wisdom tooth extraction or orthodontic treatment. Six reviews, 2 animal studies, and 6 studies in other languages (Japanese, French or Dutch) were also excluded.
Fig. 2. PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram illustrating the study literature search and selection process.
Out of 47 publications selected for full-text review, 20 were excluded after subsequent evaluation. Two did not report on EDS: one described dental treatment in a child with Keratitis-ichthyosis-deafness syndrome; the other was a cohort study on dentinogenesis imperfecta not including patients with EDS (19, 20). Six studies did not report on EDS dental manifestations (21), but on unspecific dental treatments, such as tooth extraction, caries therapy, etc. (22–25), or on oral manifestations other than tooth anomalies, such as aberrant frenula or craniomandibular disorders (26, 27). One letter to the editor (28) and 2 case reports (29, 30) were excluded because no full text was available. One questionnaire study on EDS oral symptoms including 144 individuals was excluded from clinical data analysis because of insufficient data quality, but is mentioned in the introduction (14). Finally, after content classification, 8 papers with high risk of bias due to insufficient data on dental or EDS-specific manifestations were excluded from data analysis (31–38).
The review thus included a total of 27 articles (24 case reports/series with 1–3 individuals each and 3 case-control studies), of which 22 were judged as high quality and 5 as moderate quality due to lack of data or incorrect classification of EDS necessitating reclassification by MP based on clinical descriptions provided in the paper.
Population
Two studies addressed only histological dental anomalies of classical EDS (cEDS) and hypermobile EDS (hEDS) (39, 40). Two subjects were reported twice. In total, 84 individuals with EDS were included in this systematic review: 24 with hEDS, 23 with vascular EDS (vEDS), 17 with cEDS, 10 with spondylodysplastic EDS, 3 with dermatosparactic EDS, 3 with osteogenesis imperfecta/EDS overlap syndrome, 2 with periodontal EDS (pEDS), one with arthrochalastic EDS (aEDS), and one with kyphoscoliotic EDS.
Classical Ehlers-Danlos syndromes
Study characteristics. Seven studies, including 17 affected individuals with classical Ehlers-Danlos syndromes (cEDS), reported various dental manifestations. The included studies were of 2 different designs:
Clinical manifestations (Table II). The diagnosis of cEDS was based on the clinical characteristic features of joint hypermobility, skin hyper-elasticity, easy bruising, and atrophic scarring. Two studies reported on genetic testing (41, 43). The age range was 11–40 years; sex distribution was 36% male to 64% female.
Table II. Clinical studies on dental manifestations of classical Ehlers-Danlos (cEDS) syndrome
Fifteen out of 17 individuals with cEDS showed variable pulp calcification, ranging from single pulp stones to complete pulp obliteration. Other typical dental cEDS changes included localized aplasia or hypoplasia of tooth roots, also described as shortened or sometimes bulbous roots in 9 individuals (44). Technically, severe root aplasia may lead to premature tooth loss mimicking periodontal disease (43, 44).
Two of 17 patients with cEDS showed 2–5 supernumerary teeth (42, 45). None showed crown malformations, tooth discoloration or hypodontia, the latter was validated by inspection of the published orthopantomographs.
Histological analysis. Three papers including 26 teeth reported on histological and ultrastructural features of extracted teeth (39, 40, 44). The dental tissues demonstrated significant structural abnormalities in all investigated samples. Both Pope et al. (44) and De Coster et al. (40) reported on consistently fewer uniform dimensions and cross-sections of the dentinal tubules. A number of dentinal tubules were dysplastic (enlarged), ill-defined and irregularly branched; collagen fibres were short and of irregular size and diameter (40). Klingberg et al. (39) focused on enamel analysis of primary teeth, exhibiting a high frequency of postnatally hypomineralized enamel and postnatally located incremental lines.
Vascular Ehlers-Danlos syndromes
Study characteristics. Two case-control studies investigated dental manifestations in 23 individuals with clinically and genetically diagnosed vEDS (age range 4–61 years) and 95 age- and sex-matched controls with no history of cardiovascular, endocrine, haematological, infectious or connective tissue diseases (41, 48). In both studies, teeth were clinically and radiologically assessed for structural abnormalities and secondary lesions (decay, traumatic injury), as well as root or pulp anomalies. Panoramic radiographs and bitewings were examined for anomalies of tooth number, shape and structures.
Clinical manifestations. Dental abnormalities observed with patients with vEDS affected dentine formation rather than more common dental pathologies, such as caries, pain or periodontal features (48). Pulp shape modifications (e.g. reduction in pulp volume) were reported in 52.2% of patients with vEDS; however, no pulp calcification occurred. Root malformations included exceeding root length, especially in the second mandibular molars in 34.8%, and molar root fusion in 47.8% of patients. No abnormalities were observed in tooth number or crown morphology. De Coster et al. (41) reported on demarcated enamel opacities, possibly due to caries (Table III).
Table III. Clinical studies on dental manifestations of vascular Ehlers-Danlos syndrome (vEDS)
Hypermobile Ehlers-Danlos syndromes
Study characteristics. A total of 9 clinical studies, including 24 affected individuals, reported on dental manifestations in hypermobile Ehlers-Danlos syndromes (hEDS). The included studies were of 2 different designs:
Clinical manifestations (Table IV). The clinical diagnosis of hEDS was based primarily on obvious joint hypermobility without major features of EDS. Ages ranged from 10 to 15 years, sex distribution was 6 males and 2 females (no absolute frequencies given by De Coster et al. 2005 (41)).
Table IV. Clinical studies on dental manifestations of hypermobile Ehlers-Danlos syndrome (hEDS)
There were no consistent dental features reported. Partial or total pulp obliterations of several teeth, pulp stones, and/or shortened roots were reported in 5 out of 24 individuals (41, 50, 53). In 4 individuals, 1–8 supernumerary teeth were reported (49, 51, 56). Rotation and/or transposition of single teeth were reported in 2 individuals (50, 53). In none of the cases were crown malformations or tooth discoloration reported. None of the individuals had hypodontia, as validated by inspection of the orthopantomographs provided.
Histological analysis. Histological observations of extracted teeth were reported by one paper, including 8 primary teeth of individuals diagnosed with hEDS (39). Four out of 9 teeth exhibited areas of postnatally hypomineralized enamel and postnatally located incremental lines. The dentine was always normal.
Rare subtypes
Study characteristics. Nine clinical case reports/series published up to April 2019 described various dental manifestations in 20 individuals with rare subtypes of EDS. These included aEDS, dermatosparactic EDS, kyphoscoliotic EDS, pEDS, spondylodysplastic EDS, and osteogenesis imperfecta (OI)/EDS overlap syndrome. One individual was separately included in 2 papers (57, 58).
Clinical and histological manifestations (Table V). Dental features of dermatosparactic EDS described in 3 separate individuals included agenesis of 4 permanent teeth (n = 2), irregular occlusal morphology of deciduous molars (n = 2), localized tooth discoloration (n = 2), enamel attrition of the deciduous dentition (n = 2), and localized tooth pulp obliteration (n = 1) (58).
Table V. Clinical studies on dental manifestations of rare types of Ehlers-Danlos syndromes (EDS)
In a case of kyphoscoliotic EDS dental changes included irregular occlusal morphology and malocclusion (59). No other abnormalities were reported or evident on available X-rays.
One female diagnosed with aEDS had enamel discoloration and microdontia (60). No pulp stones, pulp shape modifications, or root abnormalities of deciduous teeth were present. Microscopic examination of an extracted tooth demonstrated abnormal collagenous patterns in both the dentine and the pulp.
Three individuals with OI/EDS overlap syndrome were diagnosed with dentinogenesis imperfecta (61–63). A severely malformed exfoliated primary incisor was subjected to histological analysis (61). The dentine contained unorganized calcified masses and loss of typical dentinal tubules. The hardness and elasticity of probands’ enamel and dentine was significantly lower than those of the controls, which was attributed to the abnormal structure or quality of collagen and not to a decreased level of calcification.
Majorana & Facchetti (64) described dental features other than periodontal destruction in 2 children, aged 7 and 10 years, diagnosed with pEDS. Pulp calcifications and supernumerary teeth occurred in one individual, the other individual presented with a dens in dente. No further abnormalities were reported.
Various narrative reviews and case reports describe dental anomalies in EDS (66–69), but the true prevalence and relevance is unknown. Previously, the absence of genetic confirmation and problems of separating dental features in EDS from other conditions have confused the understanding of the oral phenotypes of EDS. Lack of evidence has led to various incorrect assumptions. For example, the recent Classification of Periodontal and Peri-Implant Diseases and Conditions claims that individuals affected by cEDS are at higher risk of periodontitis (70). This assumption is based on a case series including 3 individuals describing early loss of teeth due to root aplasia (44). In contrast, our recent systematic evaluation of published data did not reveal any individuals with cEDS and periodontitis (15). We now aimed to provide adequate information on the prevalence of dental hard-tissue abnormalities in specific types of EDS.
To date, the strongest evidence of disease-specific dental abnormalities is available for vEDS. Two case-control studies evaluated oral manifestations in a total of 23 affected individuals and 96 healthy controls. Pulp shape modifications, such as decreased pulp volume and malformed pulp chambers, were reported in 75% of affected individuals, but in only 30% of healthy individuals (48). Root abnormalities, including root fusion (50%) or exceeding root length (69%), especially in mandibular molars, were significantly more prevalent in individuals clinically and genetically diagnosed with vEDS than in controls (20% and 2%, respectively) (48). No pulp calcification, abnormalities in tooth number or other dental findings were reported.
Calcification of the pulp, i.e. pulp stones or obliteration (Fig. 3), is a common finding in cEDS and was reported in 15/17 individuals. Since cEDS is caused mainly by heterozygous mutations in COL5A1 or COL5A2, this implies a regulatory function of collagen V in pulp homeostasis. The general opinion is that pulp chamber calcification is a response to chronic irritants, such as carious and/or tooth restorations (70). Pulp calcification has also been reported in individuals with hEDS (n = 5), dermatosparactic EDS (n = 1) and pEDS (n = 1). However, there is a high prevalence of pulp calcification in the general population (71), and the mutual presentation of EDS and pulp calcification in individual cases may be a coincidence rather than a disease manifestation. Since calcification does not usually cause pulp disease or subjective symptoms, it is not clear whether it represents pathology or biological variation (71). However, calcification complicates root canal treatments, and their large size in the pulp chamber may block access to canal orifices and alter the internal anatomy (72). In the absence of any additional signs or symptoms, pulp stones should not be interpreted as a disorder requiring endodontic therapy (72).
Fig. 3. Pulp stones. Dental radiograph of a 41-year-old woman, clinically and genetically diagnosed with periodontal Ehlers-Danlos syndrome (pEDS), showing pulp stones (black circle) in the mandibular right first molar.
Defective dentinogenesis with bulbous enlargement or localized root hypoplasia (shortened roots) is both common and specific to cEDS. Subsequent loosening of the tooth can mimic localized periodontal destruction (44). The diagnostic distinction of these 2 pathologies is essential, as adequate treatment is completely different: mobile teeth with hypoplastic roots should be securely splinted to minimize subsequent bone loss. In contrast, tooth mobility from reduced periodontal attachment in the course of periodontitis requires periodontal treatment. Four patients with cEDS presented with an identical clinical phenotype of severe root aplasia restricted to the lower front teeth (43, 44). There were also 2 further case reports with identical dental phenotype, but without appropriate clinical subtyping of EDS (32, 35). Assuming that these individuals may also have had cEDS, it appears possible that root aplasia is a specific dental manifestation of this type of EDS. Further prospective studies in a cohort with validated cEDS are needed to test this hypothesis.
Dentinogenesis imperfecta is a rare published feature of aEDS, which is characterized by particularly severe joint hypermobility, with bilateral congenital hip dislocation the presenting finding in a high number of patients. aEDS is caused by loss of exon 6 in either COL1A1 or COL1A2, leading to failure to enzymatically remove the N-terminal propeptide of either alpha1(I) or alpha2(I) collagen by procollagen N-propeptidase (OMIM 130060, 120160 and 617821) and, in consequence, altered stability and assembly of triple helical collagen type I. This disorder also overlaps with certain milder forms of osteogenesis imperfecta type I (OI; OMIM 166200), also known as OI/EDS overlap syndrome. In this condition, N-terminal helical collagen COL1A1 and COL1A2 mutations typically cause dentinogenesis imperfecta and increased joint hypermobility with variable bone fractures. aEDS is distinguishable from OI/EDS both by DNA analysis (exon 6 splicing or deletion mutations in aEDS vs. mutations between exons 7 and 16) or electron microscopy of dermal cutaneous collagen fibril patterns (which are normal in aEDS). Type I collagen is the major faulty structural protein responsible for many types of OI, as well as aEDS and cardio-valvular EDS.
Previously we systematically reviewed periodontal manifestations of various EDS subtypes (15) and identified 30 articles on pEDS and 13 articles on other subtypes of EDS. In pEDS, early severe periodontitis (98.4%) and gingival recession (87.1%), as well as a striking lack of attached gingiva, were the predominant features. Early severe periodontitis was also reported in one individual clinically diagnosed with vEDS (73) and in one with hEDS (74), although from current knowledge these cases more likely represent pEDS. In vEDS, a particular gingival phenotype (generalized thinness and translucency of the gingiva and the mucosa, and decreased stippling with a papyraceous aspect) was observed in 94% of affected patients (48). Reports on periodontal manifestations in other types of EDS were rare. Severe gingival enlargement was described in 3 individuals with dermatosparactic EDS (58). Our systematic review concluded that early severe periodontitis is the hallmark of pEDS, but does not appear to be part of the clinical phenotype of other types of EDS. Just like dental manifestations, stringent analyses of periodontal manifestations in most subtypes of EDS are missing.
The published evidence on dental manifestations of EDS has substantial limitations. Specification of the EDS type based on molecular data was missing in many papers. Many published cases with dental descriptions fail to adequately specify EDS typing, and molecular data supporting a particular diagnosis are missing in the majority of reports. Due to the rarity of the syndromes themselves, mostly isolated cases were reported; therefore, uncommon dental features, including tooth rotation or transposition and abnormalities in tooth number, may be coincidental findings. Cross-sectional and longitudinal studies with systematic dental examination and radiographic analysis should be performed in various subtypes of EDS. In future, only case reports/series and studies with genetically validated EDS diagnosis should be published.
Dental phenotypes of the various types of EDS have been poorly studied. Pulp calcification and localized root hypoplasia or aplasia appear to be specific findings in cEDS. vEDS is associated with pulp shape modifications, molar root fusions and exceeding root length. Data on dental manifestations in other subtypes of EDS are inconclusive.


 Click to show fullsize
Click to show fullsize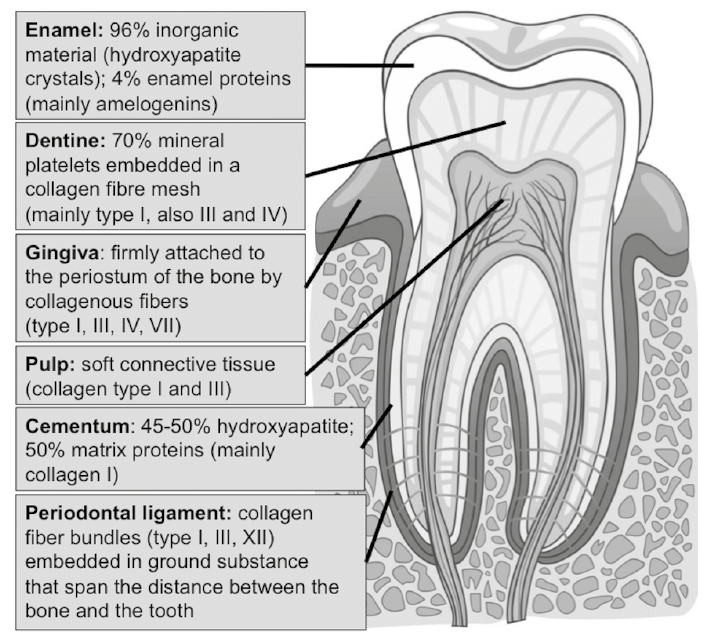 Click to show fullsize
Click to show fullsize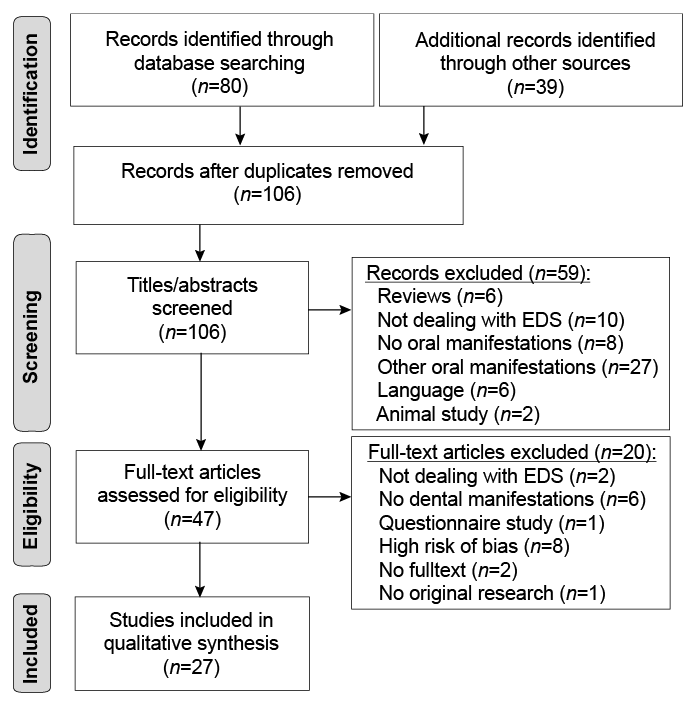 Click to show fullsize
Click to show fullsize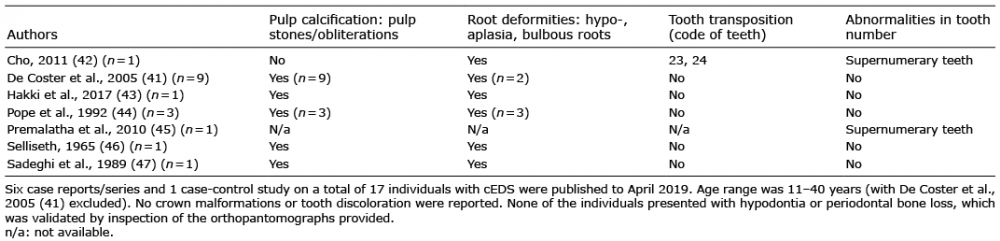 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize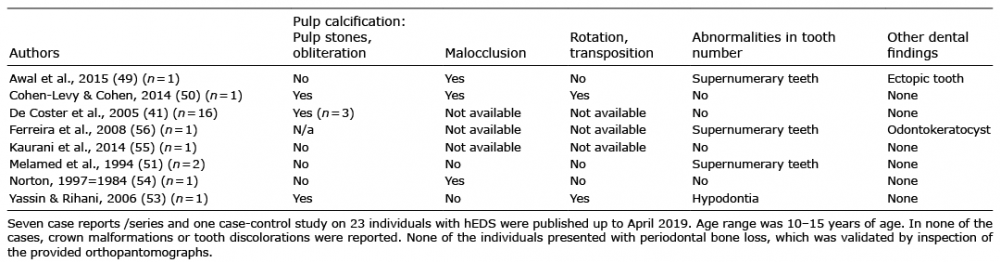 Click to show fullsize
Click to show fullsize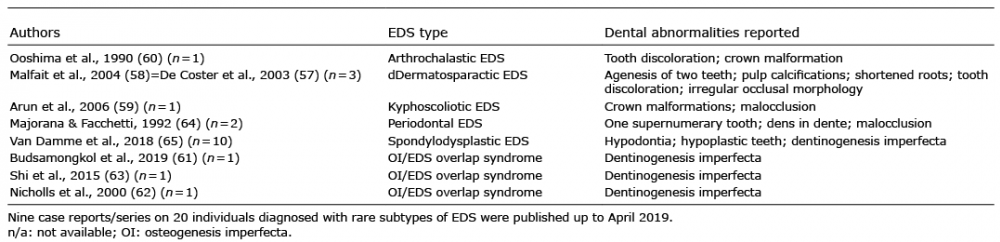 Click to show fullsize
Click to show fullsize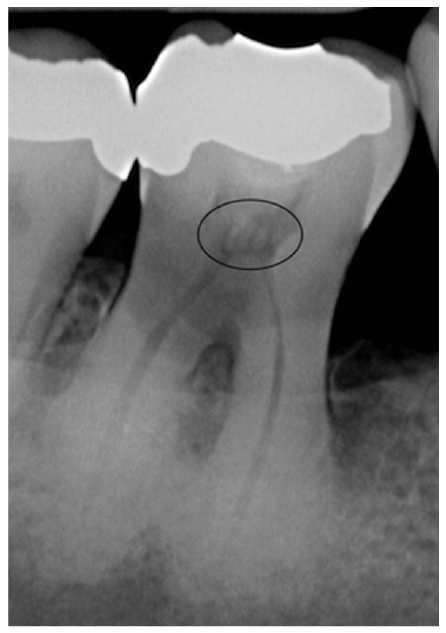 Click to show fullsize
Click to show fullsize