


Kings College London and the International Foundation for Dermatology, London UK
Skin disease is a common illness in most tropical regions where the pattern of clinical, presentations is dominated by infections. Along with common diseases such as pyodermas and fungal infections, a group of conditions known collectively as the neglected tropical diseases of the skin or Skin NTDs, which are the targets for worldwide control or elimination are also seen in health care facilities. These diseases range from the common, such a scabies, to those that are less frequent including leprosy and mycetoma. The initiative to use skin presentations of tropical diseases as a route to diagnosis by front line health workers is both logical and welcome. However, this requires training and monitoring and as the work gets under way, it is critically important that time invested in this programme is backed by firm and lasting commitment at regional and national levels.
Key words: skin disease; tropics; NTDs; scabies; tinea; mycetoma; leprosy.
Accepted Mar 19, 2020; Epub ahead of print Mar 24, 2020
Acta Derm Venereol 2020; 100: adv00113.
Corr: Roderick Hay, The International Foundation for Dermatology, Willan House, 4 Fitzroy sqaure, London W1T 5HQ, UK. E-mail: roderick.hay@ifd.org
Skin diseases are very common in the tropics. They include illnesses like ringworm, impetigo and scabies. A recent WHO programme has been to take advantage of the fact that many of the serious diseases seen in the tropics, such as leprosy and river blindness, first appear in the skin and that by detecting them, because of their appearances in the skin, their treatment and control becomes much more feasible.
Skin disease is estimated to affect more than 900,000,000 persons globally each year. It is therefore unsurprising that it is one of the common disorders seen at front line health care level in all regions (1). In most countries with a tropical climate between 20–40% of new consultations at primary care level are motivated by skin problems, although this varies, depending on the underlying prevalence of skin disease and the existence of local variations in the normal pattern and distribution of skin disease (1). Generally, in hot climates, this picture is dominated by infections, including bacterial skin infections such as pyodermas and cellulitis, mycoses including dermatophytosis as well as Candida and Malassezia infections. Viral skin infection is generally less common although warts and herpes simplex are seen regularly and the presence of an underlying high level of HIV in the community can be associated with local spikes in the prevalence of molluscum contagiosum and extensive plane warts resembling epidermodysplasia verruciformis (2). Likewise, the prevalence of scabies is variable and changes over time and, while often it affects more than 5% of the population in the tropics, it can reach even higher levels of more than 10%; these prevalence rates have been reported from Ethiopia and the West Pacific and have driven major public health initiatives designed to control the infection (3).
There is less data on the social and economic costs of these infections in poor communities, although they may have a significant impact on overstretched resources. One study in Mexico estimated that, over a 3-month period, households in rural areas were using over 24$ per household to treat scabies – and generally the treatment given was ineffective (4). This used up all cash reserves destined for other needs such as additional food. In Papua New Guinea managing tropical ulcer, or just one skin disease, accounted for more than 30% of the health budget of individual aid posts (primary health centres) in one region (5). Skin infections in the tropics are also associated with significant levels of disability and morbidly which can vary both with region and individual circumstances. For instance, the presence of tinea pedis in patients with lymphoedema, living in areas endemic for lymphatic filariasis, is a major risk factor for the development of recurrent episodes of cellulitis which lead to pain and debility, as well as loss of work (6). Alleviating disability and preventing further damage in patients with tropical ulcerated conditions such as the neuropathic ulcers in leprosy or the massive limb and scrotal swelling in lymphatic filariasis are major challenges to local resources (7). Yet linking their management to that of patients with other conditions with similar needs, such as diabetic foot or podoconiosis, is increasingly used as an effective form of integrated care package, even in remote rural areas (8, 9). Beyond physical incapacity skin disease may also be associated with severe mental illness particularly depression and in addition it affects household and societal relationships through discrimination and stigma (10). In some countries there has been both community discrimination as well as discriminatory legislation against patients with some skin diseases, including leprosy. This is now changing. In most areas such legislation, which was often introduced many years ago, has been repealed thereby allowing patients to participate in various activities that had previously been prohibited and even simple but important interventions such as ceasing to use the word “leper” or listing leprosy as grounds for divorce are making a difference (11).
While the pattern of skin disease is dominated by infection in tropical countries, it is important to recognise that other skin diseases may have an important impact on health. Although previously sparsely distributed in hot climates eczema, particularly atopic eczema, is now seen more frequently in clinical services and there is evidence that the prevalence of atopic eczema is increasing in some tropical areas (12). There are also specific problems encountered in particular population groups. Oculocutaneous albinism, with its attendant risk of early non-melanoma skin cancer, is more common in tropical regions than the colder north, affecting those living in countries from Central America, to Sub-Saharan Africa and the Pacific Region (13, 14). This poses a strain on resource-limited health systems as, if it is ignored and patients left without sun-protection advice as well as treatment, there is a high risk of fatal squamous cell carcinoma. Certain populations are also susceptible to other specific skin conditions. For instance, some native American groups are genetically predisposed to actinic prurigo which may cause severe itching and persistent debilitating light sensitive dermatoses (15). This is difficult to manage in rural populations whose main occupation is agriculture.
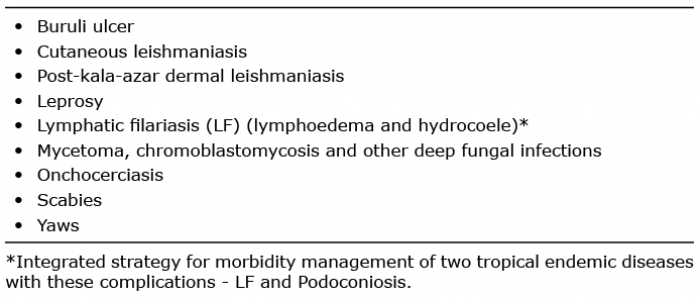
Skin disease or diseases that present in the skin are also important in a different context. Many of the important disabling infections that dominate health care in the tropics, such as onchocerciasis and leishmaniasis, are known collectively as Neglected Tropical Diseases or NTDs. Recently the World Health Organisation, supported by other agencies and scientific journals, has focused on a strategy of integrating preventative, curative and supportive care, as well as research, for NTDs, whose elimination or control forms a core part of global health strategy. A key element of this initiative has been to group these neglected diseases into clusters; in one such cluster diseases such leprosy, lymphatic filariasis, yaws and scabies constitute a group of disorders known as Skin NTDs (16) (see Table I for the full list). In order to focus on implementing their control and addressing health inequalities, it has been important to recognise and include the common readily treatable skin conditions, such as impetigo and fungal infections, together with the more serious neglected diseases such as leprosy, as part of an overall skin-centred strategy. By developing integrated schemes for case detection, management and mapping, it will be possible to maximise the advantages of an economy of scale and to rationalise the use of scarce resources (17–19). There is also a further practical benefit to be derived from combining the management of disability caused by these problems, in combatting discrimination and stigma and in sensitising communities and providing health education.
In furtherance of this initiative a new handbook on the recognition of skin diseases and Skin NTDs has been produced by the WHO and is available in 5 different languages (20). Other strategies to address Skin NTDs such as improving access to training programmes, developing common management pathways and co-distribution of drugs used for mass administration are in development. There have been a number of new initiatives arising from this work and designed to improve case detection, as well as to provide specialist support, that range from the development of diagnostic apps (21) usable in the field on handheld devices, to the provision of diagnostic algorithms and the use of long range expert support through electronic messaging and communication e.g. Telederm and Whats-App technologies (22, 23).
Table I. The neglected tropical diseases of the skin (skin NTDs)
Fungal disease
The reason for the dominance of skin infections in tropical countries is thought to reflect the prevalence of factors that favour spread and pathogenesis, such as climate and overcrowding, particularly household overcrowding. But there are other changes encountered that are different from those encountered in temperate climates, including the clinical patterns of infection. For instance, with dermatophyte infections, onychomycosis and tinea pedis are frequent presentations in colder climates whereas, in the tropics, tinea capitis and tinea corporis are much commoner. This is also subject to variation in different areas. In sub-Saharan Africa, for instance, tinea capitis is endemic in school children and prevalence rates in schools can exceed 20% (24–26). Furthermore several studies in recent years have emphasised a changing pattern of infection with Trichophyton tonsurans beginning to become more prevalent in both West and East Africa, whereas, previously, T. violaceum and Microsporum audouinii, although still common, dominated the pattern of disease (24–26). There is little to no surveillance for scalp infection in these countries and effective treatment through oral antifungal therapy is costly and inaccessible to most. Although local communities recognise that, normally, tinea capitis does not persist into teenage years the more inflammatory symptomatic forms of scalp ringworm, including kerion, pose a dilemma as effective management requires control of tinea capitis within the community, a strategy which is currently not achievable. There are other distinctive features of superficial fungal infection in the tropics. In India, for instance, there is a widespread epidemic of recalcitrant dermatophyte infection caused by Trichophyton rubrum and increasingly a strain of T. mentagrophytes (27, 28). This results in extensive tinea corporis and some strains of T. mentagrophytes appears to have mutations in the squalene epoxidase gene, meaning that terbinafine, which targets this enzyme, is less effective. Other factors which may have affected spread of this infection include the ready availability and use of topical potent corticosteroid combinations and low-quality generic antifungals. Over the past few years similar cases have been seen in Europe. The main differences seen in this new epidemic, which is affecting India and some adjacent countries and migrant populations in the Middle East and Europe, are the widespread nature of the infection and its persistence despite adequate treatment or an initial response followed by early relapse. In other tropical countries, particularly in isolated communities, there is persistence of endemic tinea imbricata caused by T. concentricum which can result in chronic and very widespread scaling and itching. New endemic areas for tinea imbricata continue to be reported (29) – the latest being in the Solomon Islands and amongst the Batek people of Malaysia (30).
Bacterial infections
Amongst the bacterial infections, there are also differences in the pattern of skin infection seen in the tropics. In colder environments Staphylococcus aureus is the main cause of skin infections. But Group A streptococcal infections are commoner in the tropics than in northern climates and the complications of nephritis (31) and rheumatic fever (32) are a potential public health problem in these regions. Streptococcal skin infection is particularly seen in association with scabies (31, 32). The relationship between streptococci and scabies mites is a complex one, as the mites produce different substances, such as Scabies Mite Inactivated Protease Paralogues or SMIPPs (33) which may interfere with complement activation and phagocytosis. As a result, scabies infestation has a direct impact on the development of streptococcal infection. As a result although traditional dermatological teaching often emphasized the need to treat secondary bacterial infection first and then the scabies infestation, current work with the oral drug ivermectin used as mass drug treatment of scabies has shown that this will not only combat the scabies mites, but also bacterial infection declines as well which supports a direct role for scabies mites in predisposing to bacterial infection (34).
Mycetoma
Mycetoma is a chronic infection, whose first signs are localised swelling and the development of papules and sinus tracts on the skin surface. It is caused either by actinomycetes or filamentous bacteria (actinomycetoma) (Fig. 1) or fungi (eumycetoma) in tropical regions from Mexico to Thailand (35). The countries with the highest prevalence are Mexico and Sudan (35). In 2016, mycetoma was formally declared to be a neglected tropical disease by WHO, becoming the first fungal infection to be given this designation. The decision was largely based on the lack of progress in controlling this infection and achieving early diagnosis which reduces the risk of disability caused by the disease that, if unchecked, can proceed to cause severe limb deformities and osteomyelitis (36). There has been a corresponding lack of research on new drug development, new diagnostics and epidemiology. The call for change was taken up in February 2019 in a large conference on mycetoma held in Sudan and attended by the Director of the NTD programme for WHO (37).
Fig. 1. Actinomycetoma due to Nocardia brasiliensis.
However, despite slow progress there are several new interesting findings about this infection. In Sudan there is an associated increase of infection in communities where cattle are grazed close to houses and the organism M. mycetomatis has been identified close to the thorn hedges around corrals used to pen the livestock (38). The taxonomy of the genera of fungal mycetoma agents has also been changed with several new species identified. For instance, we now recognise M. mycetomatis, M. tropicana, M. pseudomycetomatis and M. fahalii (39). This may have implications for accurate laboratory diagnosis and the choice of treatment options. M. fahalii, for instance, is not sensitive to itraconazole. There is now a new clinical trial of fosravuconazole for treatment of fungal mycetoma due to M. mycetomatis, based on in vitro data supporting the potential effectiveness of this group of antifungals (40). There are also newer approaches to the treatment of actinomycetoma caused by Nocardia species which have been found to respond to a wide range of antibiotics including imipenem, moxifloxacin and linezolid, in addition to the more traditional dapsone and cotrimoxazole (41). Yet there remain formidable problems in some of the simplest aspects of disease such as in detection of cases at community level (42) and improving access to laboratory diagnosis, as identification of the causative organisms is a key step in selecting the best treatment for patients (43).
Leprosy
Leprosy has long been a scourge in many tropical countries. While it causes skin lesions, which, if untreated, can be extensive and destructive, nerve damage leads to progressive sensory loss and destructive trophic changes. Changes in immunological responses to the infection, Type 1 and Type 2 leprosy reactions, lead to aggressive local and systemic reactions which are potentially fatal (44). These severe symptomatic reactions are accompanied by tissue swelling, rash, arthritis and eye disease as well as further nerve damage. Most cases of human leprosy are caused by Mycobacterium leprae, although a second species, M. lepromatosis, is now recognised (45). There is a difference of 9.1% in nucleotides between the two, confirming that they are distinct species rather than clonal variants (46). The latter causes leprosy in certain parts of the world. In Mexico for instance it is probably the commoner of the two as a cause of human disease, and it is responsible for cases of the form of leprosy known as diffuse lepromatous leprosy or Lucio’s leprosy where there can be vasculitic ulceration of lesions (46). M. lepromatosis has also been detected in Brazil, Myanmar and Singapore (47). In other countries M. leprae remains the dominant organism.
Although once endemic in Europe dermatologists in our region now only see imported cases, although it was not so long ago that Gerhard Amauer Hansen carried out his methodically planned studies in Norway, where leprosy was still endemic in the 19th century, to prove the infectious and transmissible nature of the infection. Only one autochthonous case has been reported in Europe, from Italy, in recent years (48). Elsewhere the burden of leprosy in endemic areas has shrunk over the years, although it is still seen in most parts of the tropics. There have been many attempts to identify potential natural sources of M. leprae in the environment, yet none of these have yielded results, although two animal species can be infected naturally – the 9-banded armadillo and the red squirrel (49).
A decline in the numbers of cases of leprosy towards the end of the twentieth century followed intensive case detection and the evolution and deployment of a series of drugs with potent antileprosy activity. This also involved the pioneering of suitable effective drug combinations, as well as heightened awareness at national and regional levels (50). A key aspect of leprosy has been the recognition that it presents in a spectrum, with some forms having distinctive changes on the skin and in the nerves accompanied by large numbers of organisms, whereas in others the skin lesions are different and bacteria very sparse or undetectable. These are the multibacillary and paucibacillary forms known as lepromatous and tuberculoid leprosy respectively, although variants intermediate between these two poles of the spectrum such as borderline lepromatous and tuberculoid forms, as well as an indeterminate form, are seen regularly (Fig. 2) (51). The other key feature of leprosy is that, as it is not possible to repair the damaged and defunct nerves, once this destructive process has been completed, patients are left with denervated areas resulting in anaesthetic limbs. These are prone to trauma and ulceration as well as trophic change and disfigurement even if the patient is freed from active infection as a result of treatment. Early recognition and treatment of individual cases is the way to prevent this disabling consequence of leprosy. In addition to purely clinical features of the disease, combatting disability and stigma remain other important components of leprosy care, even in the 21st century.
Fig. 2. Leprosy – borderline tuberculoid leprosy on the chest wall.
In the course of identifying major health goals to coincide with the millennium, elimination of leprosy was promoted as a suitable target. Ironically, attention was often drawn away from implementation of rigorous programmes for the detection of disease, as case numbers appeared to be on the decline, and, in order to deliver this target, diagnostic criteria were softened. As a result, there was a reduction in planned case detection programmes in some countries, which given the long incubation period of the disease, subsequently allowed the numbers of new cases to stabilise and, in some areas, to increase. Several countries such as India and Brazil are still reporting substantial case numbers and it is likely that the current official figures from other regions are a significant underestimate of the actual picture, as reporting leprosy depends on implementing programmes for the detection of new patients.
The current classification of leprosy used by WHO is based on assessment of the number of skin lesions; patients with less than 5 lesions are classified as paucibacillary (PB) and those with more than 5 as multibacillary (MB) forms of leprosy (52). There are some flaws in this scheme; for instance, acid-fast bacilli (AFB) have been detected in cases classified as PB. Such cases, presumably, provide a risk of onward transmission of the infection. Given the importance of improved case finding there have been a number of different initiatives designed to improve detection rates and simplify the process of making the diagnosis. These include both laboratory-based and clinical actions. The two traditional laboratory-based testing methods the slit skin smear and histopathology of skin biopsies, while useful, have limitations as both are susceptible to variations in observer skills or the availability of staining facilities and depend on an adequately trained work force. So one priority has been to devise a simple laboratory based test deliverable in front line health care environments – a point of care test – using techniques that can be implemented with minimal resource such as a simplified molecular tool or a card antigen detection test (53). Although a great deal of work has been carried out and is still evolving, no single antigen or PCR probe has been identified that will unequivocally identify patients with leprosy of both multibacillary and paucibacillary forms or distinguish between patients and contacts who have no active disease (54). In part this may be due to bacterial load – tuberculoid leprosy, where there is a high level of immunity and very low numbers of organisms, is potentially a difficult target. It is also worth considering the adoption of other options, such as using a combination of different laboratory tests, including some that might be combined with an algorithm based on clinical findings.
The most recent molecular results have focused on M. leprae-specific repetitive element RLEP and 16S rRNA which are the most frequent markers used in experimental studies to detect the presence of bacilli with up to 80% sensitivity, although the range of results is wide, starting from as low as 15% (51, 55). Combining molecular methods with a different test system including detection of organisms in smears may be another route for successful diagnosis (56).
Other methods, that have been attempted, have adopted a different strategy, focusing on novel surveillance and training programmes for clinical recognition of leprosy in its many different forms or the identification of the simplest features of the disease that would allow a primary health worker to refer suspected cases to a more expert team – this forms the basic premise of the new WHO training manual (20). Behind most of these programmes lies a realisation that direct clinical observation needs to be supported by at least one or two other signs such as the presence of detectable nerve damage e.g. through loss of sensation or enlargement of peripheral nerves. The detection of both requires training. Attempts to use such approaches in the field as part of broader Skin NTD programmes, aimed at detecting a range of endemic NTDs, are now under way (17, 57).
In order to rationalise the need for extensive programmes for case recognition, a new strategy is being delivered that centres around the treatment of contacts of leprosy patients with single dose rifampicin. It is known as post exposure prophylaxis or PEP (58, 59). While the idea behind this has merits, there are potential problems inherent in the widescale deployment of this strategy, notably that it does not appear to protect contacts of patients with multibacillary leprosy who are the greater sources of spread; also it only protects for up to 2 years post treatment and is only effective in some contacts of leprosy patients (60). There is also a social downside as in drawing attention to the presence of cases of leprosy in small communities, unless there is adequate local patient support, there is a consequent risk of discrimination and social ostracisation. A further practical problem is that it risks diverting attention and resource from the strategy that can deliver control i.e. new case detection, even though this is essential for identifying contacts. Measures are being taken to seek ancillary methods, such as drug combinations or different dosages, to widen the scope and inclusivity of PEP, although this may prove difficult to activate and assess, as the existing PEP scheme has already been adopted as policy in many areas.
Leprosy is a complex disease which has long been feared in many societies and sending mixed messages about elimination has served to confuse as well as divert attention from delivering a potentially achievable goal – a world free of leprosy.
The skin remains the key entry point for diagnosis and management of many tropical diseases including NTDs and HIV related skin disease, as well as other common skin diseases such as pyoderma, eczema and fungal infection. Addressing all of these is a difficult task as it means increasing the public profile of skin disease in areas where resources are limited and there is inevitable competition with other calls on financial and clinical support, such as diabetes and cardiovascular disease. But the first step to maximise the potential of using the skin, as the entry point for a radical rethink of health strategies, is to sensitise those responsible for national health care in Ministries of Health and regional health offices about the importance of proper identification and management of diseases that are seen on the skin as a means of health improvement, well beyond the confines of the skin itself. Public support, through advocacy at community level, and through regional or national media services is also key to this mission. But in all this it is important to remember a key message learned from experience with other tropical diseases in the past, that it is important to be unrelenting in reminding and re-reminding all those involved in health care, from Ministry officials to front line workers, not to forget the disease that they aim to control as soon as there appears to be an improvement in its overall burden, whether this is leprosy or scabies. To coin a soccer metaphor, by “taking ones eye off the ball” it is possible to undo years of hard work and surveillance – and for the sake of what?


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize