


Outpatients Centre for the Diagnosis of Infectious Venerodermatological Diseases, Vienna, Austria
As long as 400 years ago, syphilitic ulcers and gonococcal discharge were observed in connection with sexual intercourse. War, poverty, and lack of efficient therapeutic options led to a high incidence of venereal diseases, many of which had devastating outcomes. This situation continued until the beginning of the 20th century, when the microbial aetiology of venereal diseases was discovered. The infection rate dropped with the availability of antibiotic therapy after the Second World War. However, since the beginning of the 21st century, a steady increase in sexually transmitted infections (STIs) has been recognized worldwide. The number of reported cases of syphilis is increasing in Europe, especially in men having sex with men (MSM). Antibiotic resistance in several genital pathogens, such as Neisseria gonorrhoeae and Mycoplasma genitalium, causes therapeutic problems. Viral genital infections have become a therapeutic challenge, especially for prevention of STIs. Due to better knowledge of the long-term consequences of STIs and the connection between genital cancer and papillomavirus infections, sexual health services with screening programmes have been established in many European countries. There is general awareness of the importance of human papilloma virus vaccination programmes for young adolescents as a preventive strategy for genital cancer.
Key words: sexually transmitted infection; venereal disease; syphilis; gonococcal resistance.
Accepted Mar 19, 2020; Epub ahead of print Mar 24, 2020
Acta Derm Venereol 2020; 100: adv00114.
Corr: Angelika Stary, Outpatients Centre for the Diagnosis of Infectious Venerodermatological Diseases, Franz Jonasplatz 8-2-3, AT-1210 Vienna, Austria. E-mail: angelika.stary@meduniwien.ac.at
Sexually transmitted infections (STIs) refer to a broad spectrum of bacterial, fungal, viral and protozoal infections that share a common mode of transmission through sexual contact. While syphilis was recognized as long ago as 1496, it took several centuries to detect Treponema pallidum as the agent, and to describe Neisseria gonorrhoeae as the cause of gonorrhoea. Discovery of penicillin, and molecular biological diagnostic advances, were enormous steps forward in the control of STIs, leading to a decrease in the reported numbers of infections worldwide. However, the development of antibiotic resistance in gonococci, and the emergence of new viral infections, such as genital herpes, human papilloma virus and HIV/AIDs, have changed the pattern of STIs. Despite efforts to prevent, diagnose, and treat STIs, they remain a major problem.
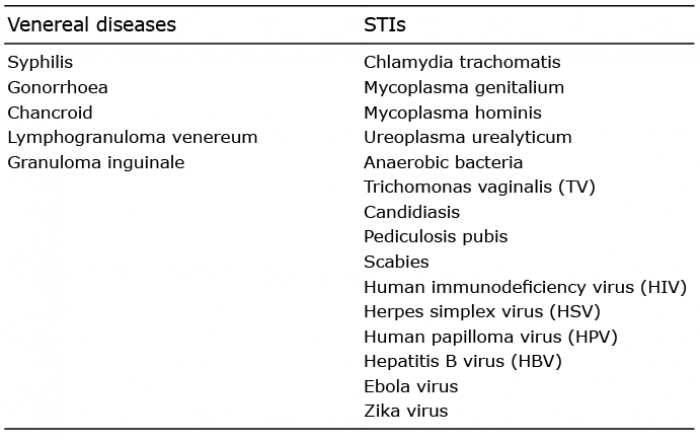
Although STIs are defined by a common mode of transmission, the diseases vary enormously in their aetiology and clinical manifestations. They may be bacterial, viral, protozoal or ectoparasitic in nature. The number of sexually transmitted or transmissible pathogens is permanently increasing and many of them can be divided into subtypes with differing clinical manifestations, e.g. Chlamydia trachomatis (Table I) (1).
Table I. Venereal diseases and sexually transmitted infections ( STIs)
The so-called venereal diseases (VD) include syphilis, gonorrhoea, chancroid, lymphogranuloma venereum (LGV), and granuloma inguinale, and were recognized as exclusively sexually transmitted when the relevant laws and regulations were written in many countries. Evolution from the term VD to the term sexually transmitted diseases (STDs) or STIs reflects the recognition of the increasing number of symptomatic or asymptomatic infections or conditions due to the high number of sexually transmitted pathogens. While some of them are transmitted predominantly, or even exclusively, by sexual intercourse, others may qualify as sexually transmissible (e.g. hepatitis B virus, HIV, yeasts), and non-sexual routes of transmission may even predominate (2).
In most STIs clinical symptoms first occur at the point of entry of the microorganism and appear as ulcers (“genital ulcer disease” (GUD): syphilis, chancroid, genital herpes), mucosal inflammation or discharge (gonorrhoea, chlamydial and Mycoplasma genitalium infection, trichomoniasis), or even neoplasia. In certain STIs the infection may spread to neighbouring (gonococcal salpingitis/epididymitis) and distant organs (gonococcal septicaemia, secondary syphilis, neurosyphilis). While usually benign (genital warts), human papilloma virus (HPV) infections with high-risk genotypes may occasionally bear the risk of malignancy and possibly result in invasive carcinoma of the vulva, cervix, penis or anal region (3). Hepatitis B (HBV), scabies and HIV-disease, mainly affect extragenital sites.
The major complications of STIs include AIDS, cancer, pelvic inflammatory disease (PID) and related sequelae, neurological symptoms, sexually-acquired reactive arthritis (SARA), complications of pregnancy and the puerperium, congenital, perinatal and postnatal infection of the foetus/infant and a variety of other diseases.
More than 100 years ago, Europe was the leading region in research on STIs. The vision that diseases in the genital tract might be caused by microorganisms was discussed in Paris in 1836, by Donne, who made some important discoveries about Trichomonas vaginalis (former name: Trico-monas vaginale), suggesting that it might not only be a harmless commensal, but a sexually transmissible microorganism causing symptoms (4).
As long ago as the 16th century, syphilis had been recognized as sexually transmitted, and was identified as a “venereal disease”, stigmatizing the infected individual. This situation continued for 400 years, until the cause of syphilis had been detected and described in Europe. Fritz Schaudinn and Eric Hoffmann, in 1905, recognized pale rotating spiral organisms when using a Zeiss microscope to examine the secretion of an erosive vulval papule from a woman with secondary syphilis (5). They named the microorganism Spirochaeta pallida and published their discovery in the paper “Preliminary report on the presence of Spirochaetes in syphilitic lesions and in Papillomas”. This was the beginning of intensive research into syphilis, a little over 100 years ago.
At that time, opinions on the cause of syphilis were diverse, until Karl Landsteiner was able to validate the presence of the microbe in specimens by dark-field microscopy, and created the new genus classification Treponema pallidum (6). This observation was followed by an enormous increase in publications on syphilis. A few years later, the “Wassermann reaction” was developed, and the results were presented at a conference in Vienna in 1908 during a congress for internal medicine. This was the first step to a reliable serological diagnosis of sy-philis, which, in modified form, is still the recommended diagnostic procedure. Treatment of syphilis ranged from mercury, organic arsenicals, bismuth, and fever cycles, or even their combination. This was often followed by mild to severe side-effects, including death. In the pre-penicillin era, infections with Treponema pallidum were a serious cause of disability or even death, and the 10th leading cause of death in the USA in 1923–25 (7). These tortuous treatments ended with the discovery of penicillin by Alexander Fleming in St Mary’s Hospital in London.
For a long time gonorrhoea was overshadowed by the severe syphilitic epidemic that threatened the infected population. The recognition of a different genital pathogen was another important scientific advantage in microbiology. Albert Neisser was the leading person in detecting gonococci in smears from men with urethral discharge (8). However, there were doubts, and the cultivation of the microbes was difficult, and they were indistinguishable from other bacteria. In Prague, Wertheim inoculated the urethra of men with pure cultures of Neisseria gonorrhoeae and induced the typical clinical picture of gonorrhoea. He also re-cultivated the bacteria from the symptomatic men, finally silencing doubters (9).
By the beginning of the 20th century the aetiology of syphilis, chancroid and gonorrhoea had been discovered, but the identity of urethral infections now known to be caused by Chlamydia trachomatis was still not defined. Halberstaetder & Prowazek described inclusion bodies in scrapings of the infected eyes of orangutans in 1907 (10). Lindner postulated a connection between genital (trachoma) and ocular infections; but it took time to discover the organism by cultivation in embryo egg cells and, furthermore, by modern immunological assays and finally by molecular biology (11).
Penile and anal warts were well known for many years, their clinical designation was changed from konylos to condylomata acuminatum, and these were described by different authors, along with an association with gonorrhoea (“gonorrhoeal warts”) (12).The hypothesis that anogenital condylomas were caused by a virus identical to skin warts was finally proven by electron microscopy in the late 1960s. Since papillomaviruses could not be cultured either in cell culture-like viruses, or on agar plates, it needed the ability to prepare cloned viral genomes and compare with virus extracted from different anatomical sites to realise that there were differences between papilloma viruses on the mucous lesions in the genital areas and the skin.
During the First World War there were high numbers of different kinds of genital infections with inadequate facilities for treatment. Venereal ablution rooms and washing units were established for infected individuals, especially those with gonorrhoea and syphilis. VD had become a problem for the soldiers and, in particular, for the US army. The importance of medical examinations and Wassermann tests was recognized. Prostitutes were regulated in several countries, and notification of infected individuals became mandatory. After the First World War the International Union against Venereal Diseases and Treponematoses (IUVDT) was formed in 1923, with the aim of encouraging member nations to collaborate in the prevention and control of VD. There was agree-ment on the need for a European network in diagnosis, treatment, and post-treatment surveillance of infected individuals and their contacts. While VD clinics were opened in Europe with improvement in health education and clinical and diagnostic development, the interest in STIs had almost disappeared in the USA. It was Thomas Parran (13) who brought the VD problem to national attention. He established programmes for syphilis control, with compulsory blood tests before marriage and during pregnancy, and established contact tracing (14). Clinical services began to improve and VD reporting also became mandatory in parts of the USA.
The Second World War had an enormous impact on the epidemiological situation of VD. Soldiers were looking for sex, not only in Europe, but also in Africa and in the Far and Middle East of Asia, and war poverty added to a high and uncontrolled incidence of STIs. The development of penicillin and other antibiotics after the Second World War changed the pattern of syphilitic and gonococcal infections, with a dramatic decline in the number of early infections throughout the world. The policy of mass testing for syphilis was established in the USA, and this was followed by mass treatment. In many European countries and in the USA the importance of VD diminished. However, despite the availability of effective treatment and better diagnosis, the symptoms of STIs re-emerged, and many men developed epididymitis, became sterile, or even developed uraemia. The resurgence of VD and STIs was due to population movements, oral contraception, the so-called sexual revolution, and the reduced use of condoms to prevent transmission. In addition, resistant microbes became a problem for gonorrhoea in developing, as well as in developed, countries.
Worldwide, over 357 million new cases of 1 of the 4 major STIs (chlamydia, gonorrhoea, syphilis and trichomoniasis) occur each year in men and women aged 15–49 years, and, according to data from the World Health Organization (WHO), more than 1 million STIs are acquired every day (15, 16). During the last decade, the numbers of genital infections in European countries were collected by the European Centre for Disease Control (ECDC) through annual data collection and online reporting (TESSy).This offers a better insight into the epidemiological situation and STI surveillance in EU/EEA countries, and includes the European gonococcal antimicrobial surveillance programme (Euro-GASP) (17). Reporting, contact tracing, and treatment of STIs is legally regulated and controlled in most, but not all, European countries, and laws have been changed during the last decade. In most of the countries, gonorrhoea, chancroid, and syphilis are mandatory reportable infections, but the procedure differs regarding what and how much on information should be reported. In many European countries, reporting of Chlamydia trachomatis infection is recommended, and, in a few countries, even mandatory.
The organization of medical services for STIs varies across Europe. Dermato-venereology is the recognized specialty in Europe, Asia, and Latin America, but not in the anglophone regions. In 1948, in the UK and in Ireland, municipal authorities established a separate specialty, called “venereal diseases” with clinics and services specifically for the management of venereal diseases. In the 1970s, the name changed to genitourinary medicine (GUM) in order to minimize the stigma associated with the term “venereology” in the general population. In contrast to the European Academy of Dermatology and Venereology (EADV), STIs are not part of remit of Dermatology associations in the USA.
In the past 50 years there has been an extraordinary improvement in the quality of science, diagnostic facilities, and the number of services concerned with STIs and HIV, as well as more options for treatment and prevention. The emergence of HIV has influenced the epidemiology and clinical pattern of STIs. Knowledge of the impact of STIs/HIV on reproductive health has increased the recognition of STIs, with public benefit. In Europe the number of reported STIs decreased with the threat of acquiring HIV, but since the beginning of this century, a steady increase has occurred again, when the status of HIV infection was changed to that of a chronic disease. The number and rates of new diagnoses of STIs have increased in the EU/EEA since the 1990s, predominantly due to transmission between men who have sex with men (MSM), except for chlamydia where the increase has been associated with more sensitive diagnostics. Improved molecular biological methods can detect asymptomatic infections in both, men and women (18, 19). Although the surveillance methods vary across Europe, data suggest that HIV-positive men contribute a significant proportion of cases of syphilis, lymphogranuloma venereum (LGV) and gonorrhoea.
Despite simple and sensitive diagnostic tests and treatment effectiveness with a single dose of long-acting penicillin, syphilis remains a global public health problem. Since the beginning of this century the infection is re-emerging and affects two-thirds (66%) of MSM, with a high proportion of HIV-infected individuals. (Fig. 1) This was especially recognized after, and in connection with, the availability of efficient antiretroviral treatment and with pre- and post- retroviral prophylaxis (PREP and PEP). In 2016, 28 EU/EEA Member States reported approximately 30,000 syphilis cases to the ECDC, a rate of 6.1 per 100,000 population, being 8 times higher in men than in women.
The clinical presentation of syphilis has not changed and it can easily be treated, since, so far, no resistance against penicillin has been recognized. However, early forms of neurosyphilis, notably ophthalmic syphilis, often remain under-diagnosed. Syphilis still causes several hundred thousand stillbirths and neonatal deaths every year in developing nations. Therefore, strong advocacy and community involvement are needed to ensure that syphilis is still given a high priority on national health agendas.
Fig. 1. Number of confirmed syphilis cases by gender, transmission category and year, EU/EEA countries reporting consistently, EU/EEA, 2010−2016. Source: Country reports from the Czech Republic, Denmark, Finland, France, Germany, Hungary, Iceland, Ireland, Latvia, Lithuania, Malta, the Netherlands, Norway, Portugal, Romania, Slovakia, Slovenia, Sweden and the United Kingdom. Permission to publish this figure is given by Gianfranco Spiteri, ECDC. Gianfranco.Spiteri@ecdc.europa.eu.
Gonococcal infections are the second most prevalent European and worldwide bacterial STIs. Infection rates vary considerably across Europe, with higher rates reported in northern Europe. In 2016 almost half of the reported cases (46%) were in MSM (ECDC). The number of reported cases increased over the last 15 years in the European region, until 2016, while in the UK the gonococcal cases remained stable in 2015 and 2016 (Fig. 2).
Fig. 2. Number of confirmed gonorrhoea cases by gender, transmission category and year, EU/EEA countries reporting consistently, EU/EEA, 2008−2016. Source: Country reports from the Cyprus, the Czech Republic, Denmark, France, Latvia, Lithuania, Malta, the Netherlands, Norway, Romania, Slovenia, Sweden and the United Kingdom. Permission to publish this figure is given by Gianfranco Spiteri, ECDC. Gianfranco.Spiteri@ecdc.europa.eu.
In contrast to Treponema pallidum, Neisseria gonorrhoeae has developed resistance to all antimicrobials previously used as first-line treatments. Most institutions, such as WHO, CDC, ECDC, and IUSTI Europe, currently recommend dual therapy with ceftriaxone (injectable, in variable volumes), together with azithromycin as first-line drugs (20). Alternatively, cefixime (400 mg once orally) has been preferred in many countries, due to its acceptance by patients as an oral single-dose regimen (21). However, the susceptibility to both extended-spectrum cephalosporins (ESCs) is decreasing worldwide (22, 23). The increase in azithromycin MICs or resistant strains, affects the mainstays of dual gonococcal treatment with third-generation cephalosporins and macrolides. The British Association for Sexual Health and HIV (BASHH) has already changed the recommendation from dual therapy to a single-shot therapy with ceftriaxone, at a high dosage of 1 g, influenced by the diagnosis of a gonococcal strain with resistance to both first-line drugs. Progression of resistance of Neisseria gonorrhoea in Europe and a realistic danger of multidrug-resistant gonorrhoea is an ever-present concern (24, 25). In this regard, performance of gonococcal culture is still necessary. In order to obtain better diagnostic information on resistant strains, a real-time PCR-based assay was designed to detect the genomic DNA of strains harbouring mosaic pen A-alleles and to discriminate them from N. gonorrhoeae and Neisseria spp. strains harbouring other genes (26). A new treatment study with zoliflodacin was performed, with successful results for urogenital and rectal infections, but was less efficacious in the treatment of pharyngeal infections (27).
Notification rates of chlamydia infections vary consider-ably across Europe, and continue to be highest among young adult women and heterosexuals. Over recent years, the overall trend appeared stable, both at the European and at the country level, with 150–250 cases per 100,000 population.
A special subgroup of Chlamydia trachomatis are the genotypes LGV1-3, causing the Lymphogranuloma venereum (LGV). In 2016, LGV data were reported by 22 European countries, out of which France, the Netherlands, and the UK accounted for 86% of the 2,043 notified cases. Almost all cases were reported among MSM with a 70% HIV-positivity rate (Fig. 3) (28). In addition to the classical clinical symptoms, with ulcers and inguinal buboes, rectal ulcerations are caused by these chlamydia strains, especially in infected HIV-positive individuals (29–31). Treatment recommendations are summarized in the guidelines of IUSTI Europe and the EADV (32).
Fig. 3. Confirmed lymphogranuloma venereum cases among the five EU/EEA Member States reporting the largest number of cases in 2016, 2007–2016. Permission to publish this figure is given by Gianfranco Spiteri, ECDC. Gianfranco.Spiteri@ecdc.europa.eu.
M. genitalium has been described recently as an important cause of genital infections in men and women, with a clinical pattern similar to Chlamydia trachomatis. It is the aetiological agent in 15–25% of symptomatic men with non-gonococcal urethritis and probably approximately 10% of women having pelvic inflammatory disease (PID) (33). Detection by nucleic acid amplification tests is the only diagnostic method available, and new CE-marked tests are approved for diagnostic use in Europe. Diagnosis and treatment is recommended in symptomatic patients. One of the main concerns is the lack of a universally effective treatment. Doxycycline has a cure rate of only 30%, whereas azithromycin is significantly more effective, with cure rates approaching 90% in macrolide-susceptible infections. However, an increase in macrolide resistance is reported in Europe, and has to be considered in treatment recommendations (34–36).
The 21st century, in general, has been characterized by a steep rise in viral STIs, in comparison with bacterial STIs. The major impact of STIs on public health today predominantly derives from viral rather than bacterial infections. This is mainly because the latter are usually amenable to curative treatment, whereas most viral STIs still represent a major therapeutic challenge. Viruses causing STIs belong to various families, such as herpes viruses (e.g. genital herpes), human papilloma viruses (HPV, high- and low-risk groups causing genital warts, intraepithelial neoplasia, genital cancer), hepadnaviruses (hepatitis B), and retroviruses (HIV-disease). Antiviral drugs are effective against HSV infections, and are recommended prophylactically if a high number of genital relapses are observed annually. HSV can cause serious problems, including brain infections, to the newborn at the time of delivery. A close association exists between course and frequency of HIV infection and that of other STIs. Sexually promiscuous patients with GUD and/or gonorrhoea or chlamydial infections are at a particularly high risk of contracting HIV. Once infected, such individuals shed considerably more virus than HIV-infected persons without genital lesions. Conversely, STIs may accelerate the course of HIV-disease; this can be deduced from the observation that different viruses upregulate HIV transcription. These facts imply that the implementation of screening and treatment programmes for STIs will not only reduce the incidence of these infections, but also help to control the spread of HIV infection.
For viral STIs, vaccination against Hepatitis B and HPV has become common, especially in the West and Centre of Europe. The prevalence of high-risk HPV in Europe is 2–16%. Although the majority of acquired genital HPV infections appear to be subclinical or asymptomatic, several high-risk strains of HPV play a central role in the pathogenesis of most squamous cell cancers, and cause the most common cervical carcinoma with potentially life-threatening consequences. High- and low-risk HPV genotypes are also inducing other cancers or genital warts in the genital tract in women and men. Vaccines to protect against high- and low-risk genital HPV infections are available worldwide and modulate the progression of HPV disease (37). Vaccination programmes are already established in many European countries, and offer pre-adolescent girls and boys HPV prevention free of charge as a public health issue.
In summary, the number and rates of new cases of STIs, such as chlamydia, gonorrhoea and syphilis, have increased in the EU/EEA since the 1990s. STIs are among the most frequently reported infections globally, indicating that national strategies, clinical services, and public health activities are beneficial public health instruments for the prevention and control of STIs and their long-term sequelae.


 Click to show fullsize
Click to show fullsize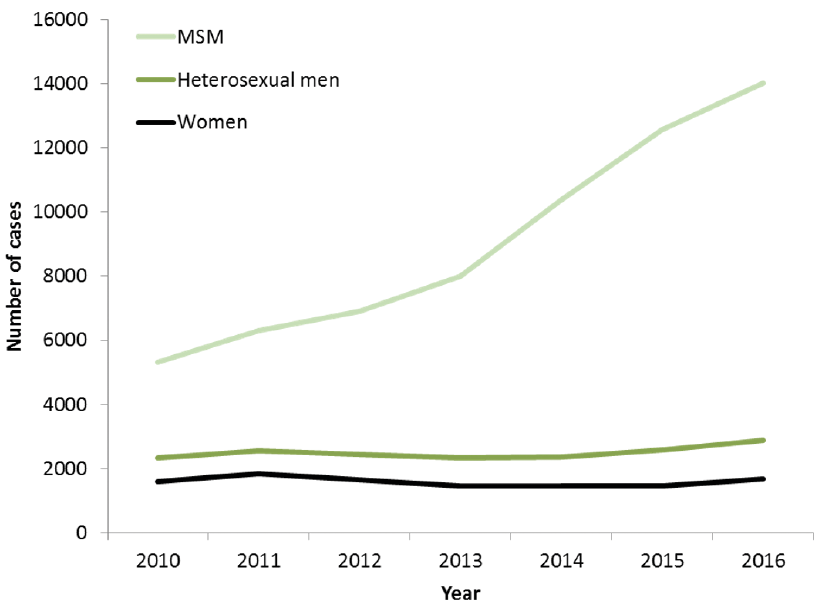 Click to show fullsize
Click to show fullsize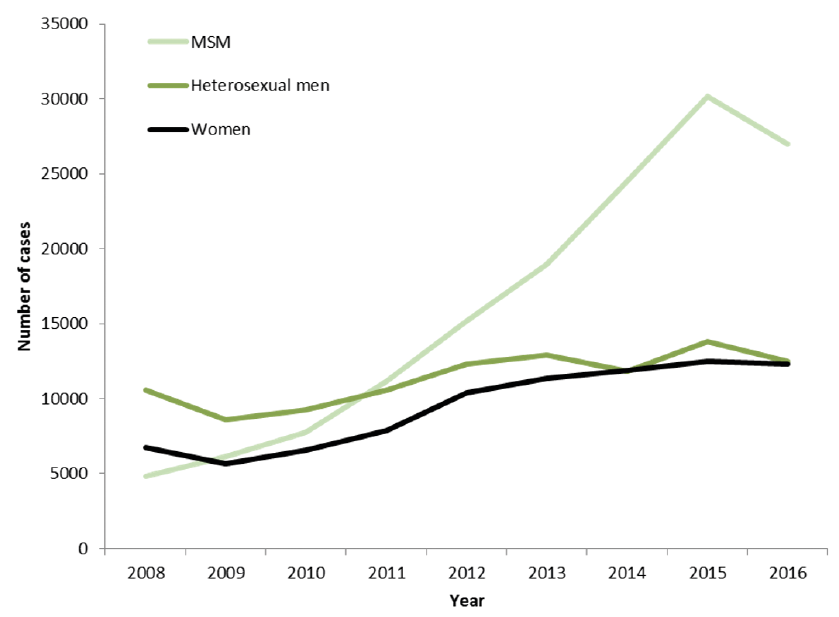 Click to show fullsize
Click to show fullsize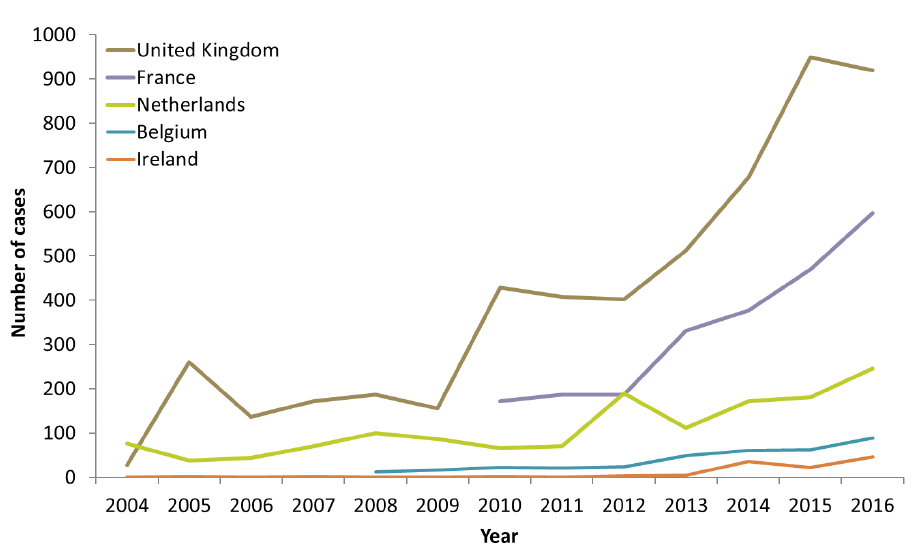 Click to show fullsize
Click to show fullsize