


Department of Dermatology and Allergy, University Hospital Bonn, Venusberg-Campus 1, DE-53127 Bonn, Germany. E-mail: joerg.wenzel@ukbonn.de
Accepted Apr 2, 2020; Epub ahead of print Apr 8, 2020
Acta Derm Venereol 2020; 100: adv00144
This case report describes the successful treatment of a woman with refractory dermatomyositis (DM) with ruxolitinib, a specific janus kinase (JAK) inhibitor, which concomitantly resulted in complete remission of her longstanding alopecia areata universalis (AA).
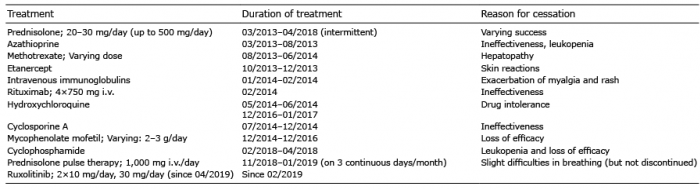
A woman in her 40s presented at our department with an acute exacerbation of a recalcitrant DM first diagnosed 6 years ago. She reported severe weakness of proximal muscles of the extremities, which left her incapable of coping with everyday business. Clinical examination revealed DM-typical skin symptoms, such as a heliotropic erythema at her periorbital area, her chest (“v-sign”) and neck (“shawl-sign”), as well as erythro-squamous papules on the dorsal side of the finger joints (“Gottron’s sign”). Her laboratory results revealed antinuclear antibodies (ANA) in high titres and transcriptional intermediary factor 1 (TIF1)-γ antibodies. Treatment attempts with prednisolone, azathioprine, methotrexate, etanercept, intravenous immunoglobulins, rituximab, hydroxychloroquine, cyclosporine A, mycophenolate mofetil and cyclophosphamide remained ineffective or had to be discontinued because of drug-related side effects (Table I).
Table I. Synopsis of all attempted treatments the patient received from 2013 until 2019, which partly remained ineffective or had to be terminated due to drug-related side effects
The patient had also had AA for more than 20 years, and despite the aforementioned immunosuppressive drugs, she presented clinically with complete baldness of the scalp during the last 10 years. Due to the ineffectiveness of the numerous previous treatment strategies it was decided to start steroid-pulse therapy (1,000 mg prednisolone/day on 3 days per month, for 3 consecutive months), which reduced creatine kinase (CK)-serum levels, but left the patient in a poor general condition and with a strong therapeutic need (Fig. 1B).
Since JAK inhibitors have been described previously as a potential therapeutic strategy for DM, treatment with the JAK inhibitor ruxolitinib was initiated at a dose of 10 mg twice a day (1). After 4 months the patient presented with a noticeable improvement in myalgia, muscle strength and skin condition. In addition, the patient showed generalized hair regrowth on the scalp and eyebrows (Fig. 1A). To date, both DM and AA have remained significantly improved under monotherapy with ruxolitinib (30 mg per day).
Fig. 1. Clinical and molecular findings of inflammatory hair and skin conditions under janus kinase (JAK) inhibitor treatment. (A) Complete hair regrowth of the scalp and eyebrows in a patient with longstanding AA universalis under treatment with the JAK inhibitor ruxolitinib: clinical images, taken in April, June and September (Sept) 2019, after initiation of JAK inhibitor therapy in February 2019. (B) Course of creatine kinase (CK) serum levels (in U/l) of the patient during steroid-pulse (3×3×1,000 mg prednisolone i.v.) and ruxolitinib treatments from November 2018 (Nov ‘18) to September 2019 (Sept ‘19). Ruxolitinib therapy was initiated in February 2019, with a dosage of 2×10 mg per day, and increased to 30 mg per day in April 2019. (C) Expression of genes attributed to the biological process “hair cycle” (gene ontology), such as keratins (KRT) and keratin-associated proteins (KRTAP) is significantly upregulated in JAK treated lesional skin (n = 3) compared with placebo (PBO)-treated skin (n = 3) of lupus prone TREX1–/– mice (n = 6). In contrast, the expression of interferon (IFN)-associated proinflammatory genes, such as CXCL- and CCL-chemokines in lesional skin treated with a JAK inhibitor is significantly downregulated in comparison with PBO (≥ 2-fold, p < 0,05; Welch’s t-test). Red represents upregulation of gene expression, green represents downregulation; higher intensity of colour denotes a greater fold-change.
JAK inhibitors have the potential to simultaneously target various pathogenic pathways by blocking intracellular signalling linked to a broad spectrum of receptors. Most importantly, these drugs are highly effective suppressors of proinflammatory cytokines, which function as key drivers in several autoimmune skin disorders, including DM, lupus erythematosus and AA (2). These diseases share a significant upregulation of interferon (IFN)-associated proinflammatory chemokine expres-sion, which is mediated by JAK/signal transducers and activators of transcription (JAK/STAT) signalling. In particular, CXCR3+ chemokines are known to recruit effector cells into lesional tissue, inducing myocyte and keratinocyte cell death in DM and loss of the hair follicle immune privilege with anagen arrest in AA (3, 4). Strikingly, in the current patient, hair growth re-occurred under JAK inhibitor treatment, despite the patient’s decade-long and therapy-resistant extensive AA with clinically observed complete absence of hair follicles, which normally makes a treatment response highly unlikely (5).This might be due to a specific positive effect of JAK inhibitors on reinduction of hair follicle progenitor cells and immune privilege. This suggestion is supported by recent findings of our group in a lupus-prone mouse model (TREX1–/–), in which treatment of hairless skin lesions with a topical JAK inhibitor resulted in hair growth and a strong upregulation of hair cell cycle associated genes (Fig. 1C) (6).
In summary, this case demonstrates a notable benefit from JAK inhibitor treatment in a patient with both recalcitrant DM and AA. This case supports the idea of JAK inhibitors targeting shared central pathobiological features of these conditions in a specific manner compared with conventional immunomodulating drugs; thus providing an effective therapeutic strategy, particularly in refractory cases.
We thank the patient for granting permission to publish this information. The animal experiment was performed in accordance with the guidelines of the EU Directive 2010/63/EU and approved by the animal welfare commission of North Rhine-Westphalia, Germany (AZ 2014.A436).
Conflicts of interest: The following authors have been an advisor and/or received speakers’ honoraria or travel expense reimbursements and/or received grants and/or participated in clinical trials of the following companies: DN: BMS, Novartis, GSK, Celgene, L’Oreal and MSD. JW: GSK, Incyte, Novartis, Medac, Merck/Serono, Roche, Actelion, Pfizer, Spirig, ArrayBio, Biogen. All other authors declare that the research was conducted in the absence of any commercial or financial interests and relationships that could be construed as a potential conflict of interest.


 Click to show fullsize
Click to show fullsize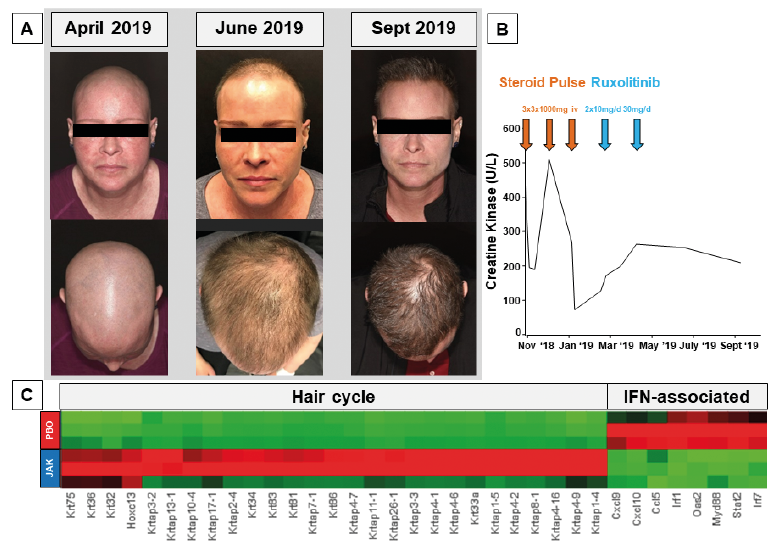 Click to show fullsize
Click to show fullsize