


1Twin Research and Genetic Epidemiology Department, Kings College, London, and 2Dermatology Department, West Herts NHS Trust, Herts, UK. E-mail: bataille@doctors.org.uk
There is increasing evidence that the behaviour of naevi and melanoma is under significant genetic and/or epigenetic control. Melanoma tumours behaves similarly all over the world. Many genes have now been implicated in melanoma risk and naevi number. Embryogenesis has also been important in the discovery of links between several neurological diseases and melanoma susceptibility. Telomere biology, which regulates cell senescence, is increasingly relevant in melanoma. Melanoma is often found in the context of family cancer syndromes and the identification of these families is important as screening for cancer will save lives. Melanoma is also one of the most immunogenic cancer as the behaviour of naevi and melanoma differ in patients with vitiligo or eczema. The search for non-sun-related melanoma risk factors should continue as it is likely to lead to important discoveries which will, in turn, have an impact on therapeutic targets for this tumour.
Key words: telomere; naevi; vitamin D; family cancer syndromes; body mass index.
Accepted Apr 27, 2020; Epub ahead of print Apr 28, 2020
Acta Derm Venereol 2020; 100: adv00137.
Corr: Veronique Bataille, Twin Research and Genetic Epidemiology Department, Kings College, London, UK. E-mail: bataille@doctors.org.uk
Many risk factors for melanoma are non-UV-related and progress in the last 20 years have been instrumental in discovering melanoma genes which are involved in telomere biology, naevi number, pigmentation, body composition, energy expenditure, neural and melanocyte differentiation. Melanoma behaves in a very similar way all over the world in all Caucasian populations and many host factors are under tight genetic control. Research in these areas is important as it sheds new light on genetic and epigenetic factors which are often set early on in life and less likely to be influenced by sun exposure in adulthood. It is also unravelling pathways which could be exploited for future therapies as public health campaigns have, so far, not been very effective. Perhaps, the role of sun exposure in melanoma has been over-estimated in the past as, like all cancers, melanoma is a very complex tumour so addressing environmental exposure cannot be the only focus of our efforts.
In this review, the importance of non-sun-related melanoma risk factors are presented looking at telomere biology, genetics, gender differences, body mass index, body sites, naevi biology, immune-related factors and links to neurological disorders.
Telomeres are strand of non-coding DNA capping the end of chromosomes protecting them from decay. They are having important and complex roles in cell replication and senescence. Protecting against cancer formation is achieved by silencing telomerase which leads to telomere erosion with age. The speed of telomere attrition is under the influence of both genetic and environmental factors. Chronic illnesses and obesity have been associated with shorter telomeres. On the other hand, cancer is usually linked to longer telomeres (1). In 2007, the first report of a link between melanoma susceptibility and telomere biology was suspected with a positive association observed between high number of naevi, the strongest risk factor for melanoma, and circulating white cell telomere length (2). In 2009, case-control studies supported this finding in melanoma case control studies (3). A few years later, a very large melanoma pedigree with no previously known germline mutation, was found to have a germline mutation in the promoter of the TERT gene, a telomere gene (4). Mutations in the promoter of the TERT gene were then investigated at the somatic level and were found to be common in melanoma tumours (5). The same year, 11 SNPs in genes predicting white cell telomere length were published (6). Using the same 11 SNPs, genetic scores were created to assess their effects in a large melanoma case control study in the UK. These combined SNPs scores predicting telomere length were confirmed to be predictive of melanoma risk (7).
The associations between TERT promoter mutations, telomerase activity and telomere length are, however, quite complex. It has been shown recently that different SNPs within the TERT promoter have different effects on TERT expression and telomere length despite all being associated with an increased risk of melanoma (8, 9). This implies that the risk of melanoma is not solely explained by elongation of telomeres in some of these families. In rare melanoma families, POT1, another telomere gene, has been identified over the last few years (10). Recent genome wide scan analyses (GWAS) on melanoma and/or naevi number have also identified further telomere genes (11, 12). There are more telomere genes linked to melanoma susceptibility compared to naevus count highlighting the fact telomere genes do not always drive melanoma risk via an excess of naevi (11). Mutations in telomere genes also raise the risk of many types of cancers so the documentation of all cancers in first- and second-degree relatives of melanoma patients is important. Glioma, neuroblastoma, lung cancer and melanoma are more commonly reported in rare families with telomere mutations but many cancer types can be found (13).
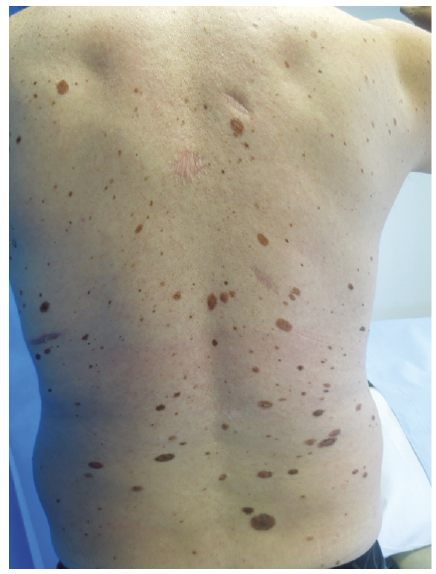
The fact that long telomeres are associated with a susceptibility to melanoma may be behind the observation that individuals within melanoma families with high number of naevi, have reduced cutaneous photoageing. The delayed senescence in melanocytes reflected by the presence of the atypical mole syndrome phenotype is likely to be seen in other cell types such as fibroblasts and keratinocytes (Fig. 1). The background for squamous cell carcinoma is, on the contrary, a very photoaged skin. SCC is more likely to be associated with shorter telomeres contrary to melanoma (14). So, by looking at skin phenotypes, short or long telomeres may have opposite effects on signs of cutaneous ageing and, in turn, on specific skin cancer risk (15). This is supported by the negative association between solar keratoses and naevi number both risk factors for melanoma despite adjusting for age (16). This dichotomy has been reported a long time ago via phenotypic studies and is known as the dual pathway to melanoma (17).
Fig. 1. Male with the atypical mole syndrome phenotype with previous melanoma primaries. Presence of larger atypical naevi towards the lower back.
Melanoma survival is also affected by TERT promoter mutations with worst survival for those carrying different types of mutations. This contrasts with a study published by Ribero et al. (18) showing that large number of naevi (hence predicted longer telomeres) confers a survival advantage in melanoma even in patients with positive sentinel node. However, as mention above, not all telomere gene mutations have the same effect on telomere length so this may explain opposite effects. Telomere biology is also important for potential therapeutic targets: RAS mutated melanomas represent 25% of melanoma tumours and have not had, as yet, effective gene targeted treatments. These RAS mutated melanomas appear to have a dependency on TERT which could be exploited for slowing melanoma growth (19, 20).
The balance between long telomeres leading to an increased risk of cancer versus short telomeres leading to premature ageing with frailty needs to be fine-tuned as the extreme spectrums of long and short telomere syndromes show that belonging to either of these extreme group is not advantageous (1). Most melanoma patients survive their disease and the beneficial impact of longer telomeres is likely to be apparent in old age with reduced senescence in many cell types. It could therefore be speculated that genes associated with melanoma susceptibility may have a survival advantage and have therefore remained common in Caucasian populations.
Melanoma is more common in cancer prone families as discussed above. However, many other non-telomere genes can be implicated in cancer susceptibility within these families. P16 or CDKN2A was one of the first melanoma gene discovered more than 20 years ago and mutations in this gene lead to an increased risk of melanoma, pancreatic cancer, lung cancer and many other tumours (21). The recruitment of melanoma families for genetic studies over the last 20 years mainly included families with multiple melanomas so family cancer syndromes were excluded. It is, however, well known that some melanoma families may present with many different cancer primaries. These family cancer syndromes are now being studied as well with collaborations from many countries via the GENOMEL consortium (www.genomel.org) with many new genes shared with other cancers being discovered. This is why melanoma germline genetic panel have become more comprehensive. The risk of melanoma in these families is higher in Australia compared to the UK so the penetrance of rare high penetrance genes such as p16/CDKN2A is affected, in part, by sun exposure. Screening bias is also at play in Australia with many borderline melanomas excised in Australia compared to Europe in view of the active skin surveillance there. Many individuals with p16/CDKN2A mutations have the atypical mole syndrome phenotype usually evident by late teens. However, this phenotype is not always found in mutant individuals so using the naevus phenotype to select family members at risk is not reliable (22). Individuals within these families have reduced senescence in many cell types and not only melanocytes and therefore patients with high number of naevi have reduced photoageing, higher bone mineral density and better cognitive functions with age (23, 24).
Families with BPA1 mutations may present with clinically and histologically recognisable lesions typical of this syndrome called BAPOMAs. These families also have an increased risk of skin and eye melanoma, kidney cancer, mesothelioma and breast cancer (25). BRCA1 and BRCA2 families, apart from the high risk of breast and ovarian cancer, also have an increased but smaller risk of both skin and eye melanoma. However, eye melanoma is a rare tumour and there is no need to offer screening for this as retinal photography is now being offered by many opticians. Melanoma can also occur in rare retinoblastoma families because of the link between the Rb gene and the CDKN2A/CDK4 pathway. Neurofibromatosis families are at risk of melanoma because of the role of NF1 in melanocyte differentiation and growth. This syndrome is part of a group of diseases called Rasopathies where melanoma is more commonly seen such as Noonan syndrome and Leopard syndrome (26). MITF mutations predispose to melanoma and kidney cancer (27, 28). The MITF gene is a crucial gene in melanocyte differentiation.
Many cancer genetic clinics now include p16/CDKN2A and CDK4 in their panels as well MITF, BAP1 and several telomere genes. However, it is likely that very soon all melanoma families will undergo much more comprehensive gene panel for mutation screening as they are becoming cheaper. These panels should not be limited to melanoma genes only. This will be beneficial for these families as the identification genes linked to other cancers such as colon, kidney, breast and ovary, for example, can be addressed with specific screening recommendations for the family and will save lives. Genes associated with melanoma in the context of family cancer syndromes are summarised in Table I.
Table I. Genes and family cancer syndromes linked to melanoma
Melanoma risk, like all cancers, is related to body mass index (BMI) (29). Whilst it was thought to be mainly driven by increased weight, the relationship is mainly driven by height. Naevus count is also related to height rather than weight and it is speculated that growth factors are important in melanoma susceptibility. One possible explanation for this observation is telomere biology. Telomere length and cancer risk are also positively associated with height (24, 29). High BMI or obesity is, on the contrary, inversely, correlated with telomere length (30). Another observation is that patient with the atypical mole syndrome phenotype are usually taller than average but not significantly overweight or underweight with strong muscular mass. There is therefore some interesting links between melanoma susceptibility and body composition and growth. Bone mineral density is also correlated with number of naevi and this remains significant despite adjusting for telomere length, so bone senescence is also delayed in these patients as discussed above (24).
Another paradox in melanoma is the lack of cachexia in advanced melanoma. Compared to other cancers, melanoma patients in stage 4 of the disease present with weight loss very late in the evolution of their metastatic disease. There is also some evidence that melanoma patients treated with immunotherapy have different treat-ment responses according to fat distribution with better responses in patients with higher subcutaneous fat and strong muscle mass but not with high fat mass and low muscle mass (31).
Insulin metabolism and energy expenditure may also have a role in melanoma. However, a recent study showed that levels of IGF1 were not linked to an increased risk (32). The melanocyte-stimulating hormone (MSH) pathway is also relevant as, apart from the MC1R gene controlling pigmentation and other immune-related factors, other genes in the MSH pathway such as MC4R gene are also important in energy expenditure. In animal models, weight is related to colour coat pigmentation (33). The FTO gene, also linked to obesity, is reported in melanoma GWAS (33). However, there is some evidence that the FTO gene may not act via its effects on obesity as SNPs involved in melanoma differ from those reported in high BMI (34, 35). The effects may, in fact, be mediated by pathways shared between the FTO gene and telomere genes (36).
Vitamin D has been found to have a significant role in melanoma survival as low levels of serum vitamin D are a negative prognostic indicator in melanoma (37, 38). On the contrary, patients with high vitamin D levels have thinner melanoma tumours but also have higher number of naevi. The relationship between high number of naevi and higher vitamin D levels is complex but despite adjusting for age and skin type, the association between high number of naevi and high vitamin D remains (39). Further adjustment for telomere length (as telomere length affects vitamin D levels as well), decreases the magnitude of the association but it remains significant. This shows that whilst telomere biology is important in the relationship between melanoma and vitamin D metabolism, other factors are at play. This has implications for public health as patients are advised to avoid sun exposure after a melanoma diagnosis and this may affect their survival. This is supported by a study showing that sun exposure after diagnosis of melanoma was protective in terms of relapse in Italy (40).
Melanoma behaves differently in women and men both in terms of body sites and survival. It is well established that melanoma in females are more common on the legs compared to males and the reverse is true for males where melanoma is commonest on the trunk. This difference in body sites is observed all over the world and sun exposure levels do not affect it. Furthermore, the distribution of naevi in girls versus boys is already different earlier on in life and mirrors the distribution of melanoma in adults: boys have more naevi on the torso and girls have more naevi on the limbs, especially the legs. There is therefore some sex specific melanocyte migration which does not appear to be related to sun exposure. A recent study showed that genes/loci already known to predict naevi numbers such as IRF4, DOCK8, MTAP, 9q31.2, KITLG and PLA2G6 have different effects on naevi numbers on the torso versus limbs versus head (41). It is likely that epigenetic effects with X inactivation in females explain, in part, some of these sex differences for naevi and melanoma. Females with Turner syndrome with a XO genotype have large number of naevi on the limbs and are also more prone to melanoma and brain tumours (42).
It is evident for dermatologists that some type of naevi have a predilection for specific body sites. Intradermal naevi are more common on the face and rarely seen on distal limbs. Atypical naevi are more common on the central body and rarer on distal limbs and extremely rare on the face. This again most probably relates to specific genetic signals for melanocyte migration and growth at different body sites. Unfortunately, not many studies counting naevi have, so far, differentiated between different types of naevi (intradermal versus compound versus junctional). One twin study in Australia, has collected clinical subtypes of naevi. They have shown that SNPs in the IRF4 gene, which was the strongest signal for their Australian naevi GWAS based on more than 1,800 adolescent twins, was having opposite effects on flat versus raised naevi. Gene may also have divergent effects according to age when comparing adolescent twins to adult twins (mean age 40–50 years) (11). The different gene effect size according to age groups shows that having very large sample size for GWAS with wide age ranges can identify differential gene expression with age. IRF4 is also a gene linked to freckling, fair skin and tanning ability which shows that skin pigmentation is tightly linked to types and number of naevi (43, 44). It is well known that the atypical mole syndrome with many junctional and intradermal naevi is rare in dark skin phototypes so pigmentation genes not only govern naevi colour, but they also have an effect on size, numbers and clinical subtypes of naevi. Visconti et al. (41) have confirmed in a recent study that body site specific genetic effects exist in females for quite a few known naevi genes/loci such as IRF4, DOCK8, MTAP, 9q31.2, KITLG and PLA2G6. In this large collaborative study, based on many cohorts, the analyses of 3,000 UK twins showed that the heritability of naevus number in females (assessed by comparing MZ to DZ female twin pairs) was the highest on the legs (69%) compared to torso (26%). Leg is also the body site where females have more naevi and a predilection for melanoma, so it is interesting to find that this site is under the strongest genetic control for naevi number.
In high risk melanoma families with the atypical mole syndrome phenotype, it is not uncommon to see large atypical naevi in the parietal area of the scalp and rarely at any other sites on the scalp (Fig. 2). In embryogenesis, the head development goes through successive phases which may explain the specific behaviour of naevi on specific part of the head and neck. These scalp naevi often are the first ones to appear in children in high-risk families. It is also observed that in patients with the atypical mole syndrome phenotype, atypical naevi increase in size from the upper back to the lower back especially in males which, again, is likely to be governed by genes differentially expressed at different body sites. However, what is puzzling is that many genes involved in melanocyte migration and differentiation in embryogenesis are not found in melanoma/naevi GWAS. It is likely that these early melanocyte genes interact with other gene pathways. One example for this, is the MITF gene, a very important gene early on in embryogenesis for melanoblast/melanocyte migration. Many melanoma genes have MITF binding sites so the discovery of new melanoma genes will need to look at all these gene-gene interactions (44).
Fig. 2. Large atypical naevi in the parietal scalp. These are usually very stable as scalp melanoma is very rare. They are often found in patients with the atypical mole syndrome and just need monitoring and not prophylactic excision.
Naevi distribution have an inverse distribution to vitiligo. Vitiligo develops often in folds such as axillae, groins but also on the face around the eyes and mouth as well as on the hands and feet (45). Melanoma and naevi are very rarely found in vitiligo predilection sites. Vitiligo patients also have a reduced risk of melanoma. Melanoma is one of the most immunogenic cancer. It is therefore possible that immunological signals which are inhibitory for melanocyte growth explain this inverse body distribution between vitiligo and naevi/melanoma. Quite of few of the vitiligo genes are shared with melanoma and most of these are related to skin pigmentation. The same SNPs have been reported but have opposite effects in vitiligo versus melanoma which is interesting as it supports the protective effect of vitiligo on melanoma risk. However, how do the same SNPs do offer protection from melanoma in vitiligo patients is unclear (46). Immune-related genes amongst others are likely to affect these divergent associations as CTLA4, a target for the most successful melanoma therapy, is also a vitiligo gene.
Another observation is the lower number of naevi and lower incidence of melanoma in eczema cohorts and this, again, supports the fact that immunological signals in atopic patients may have an inhibitory effect on melanocytes in the skin (47).
Naevi disappear with age, especially junctional and compound naevi and the mechanisms for this process is not fully understood but senescence via genes such as p16, p21 and p53 as well as telomere genes and immune surveillance are likely to all play a role (2, 48). Patients with the atypical mole syndrome phenotype, especially within high risk families, are more likely to present with halo naevi phenomenon than controls. They also show a delayed senescence of naevi with age with large number of naevi persisting well after the age of 50 years. The presence of multiple junctional and atypical naevi after the age of 50 is a reliable sign for dermatologists that an individual is at an increased risk of melanoma.
Naevi originates from the neural crest and it has long been observed that melanoma and Parkinson disease can cluster in some families. Many melanoma genes were later found to be Parkinson genes such as PLA2G6, BAP1, DCC, ERBB4, KIT, MAPK2, MITF, PTEN, and TP53 (49). Pigmentation may also be important in the link between Parkinson and melanoma as fair skin is more prevalent in Parkinson cohorts and, so far, the MC1R gene has been implicated (50).
Charcot Marie Tooth and amyotrophic lateral sclerosis (ALS) are also neurological diseases linked to melanoma (51). The association between these neural diseases and cancer risk is puzzling as Parkinson disease and ALS have, in fact, an overall reduced risk of cancer so the link to melanoma may be because of the neural connection (51).
The NF1 gene is an important prognostic factor for melanoma at the somatic level and patients with neuro-fibromatosis have an increased risk of melanoma (52). NF1 positive tumours are more likely to be found in the elderly and often have a desmoplastic histology (52). Neurofibromatosis, is part of a group of diseases called Rasopathies such as Noonan syndrome, Leopard syndrome and Leguis syndromes. All these disorders are characterised by the activation of the MAP kinase pathway which is highly relevant in melanoma (26).
In summary, many risk factors for melanoma are non-UV-related and progress in the last 20 years have been instrumental in discovering melanoma genes which are involved in telomere biology, naevi number, pigmentation, body composition, energy expenditure, neural and melanocyte differentiation. Melanoma behaves in a very similar way all over the world in all Caucasian populations and many host factors are under tight genetic control. Research in these areas is important as it sheds new light on genetic and epigenetic factors which are often set early on in life and less likely to be influenced by sun exposure in adulthood. It is also unravelling pathways which could be exploited for future therapies. Although excessive sun exposure is associated with melanoma risk, research on non-sun-related risk factors is important to redress the balance. The collection of good phenotypic and familial data as well as tumour and blood DNA is crucial for future genetic-epidemiological studies.


 Click to show fullsize
Click to show fullsize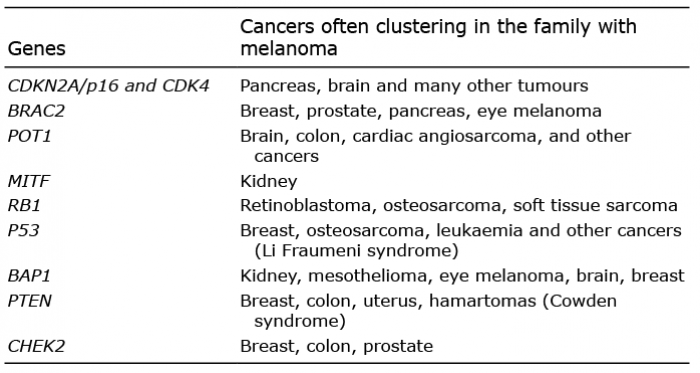 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize