


Department of Dermatology, Universite Paris 7, Hôpital Saint-Louis, 1 avenue Claude Vellefaux, FR-75010 Paris, France. E-mail: nicole.basset-seguin@aphp.fr
Basal cell carcinomas are the most frequent skin cancers in the fair-skinned adult population over 50 years of age. Their incidence is increasing throughout the world. Ultraviolet (UV) exposure is the major carcinogenic factor. Some genodermatosis can predispose to formation of basal cell carcinomas at an earlier age. Basal cell carcinomas are heterogeneous, from superficial or nodular lesions of good prognosis to very extensive difficult-to-treat lesions that must be discussed in multidisciplinary committees. Recent guidelines have updated the management of basal cell carcinoma. The prognosis is linked to the risk of recurrence of basal cell carcinoma or its local destructive capacity. Characteristic molecular events in these tumours are: (i) activation of the hedgehog pathway, which has allowed the development of hedgehog inhibitors for difficult-to-treat lesions that are not accessible to surgery or radiotherapy; (ii) high mutational burden, which suggests that hedgehog inhibitor refractory tumours could be offered immunotherapy; some trials are ongoing. The standard treatment for most basal cell carcinomas is surgery, as it allows excision margin control and shows a low risk of recurrence. Superficial lesions can be treated by non-surgical methods with significant efficacy.
Key words: basal cell carcinoma; treatment; prognosis; surgery; radiotherapy, hedgehog inhibitors.
Accepted Apr 27, 2020; Epub ahead of print Apr 28, 2020
Acta Derm Venereol 2020; 100: adv00140.
Corr: Nicole Basset-Seguin, Department of Dermatology, Universite Paris 7, Hôpital Saint-Louis, 1 avenue Claude Vellefaux, FR-75010 Paris, France. E-mail: nicole.basset-seguin@aphp.fr
Basal cell carcinoma is the most frequent cancer in fair-skinned adults. The molecular background to these tumours includes activation of a cellular pathway called the “sonic hedgehog pathway”. Basal cell carcinomas are induced by ultraviolet light and occur more frequently on areas of skin that are exposed to the sun. Basal cell carcinomas rarely spread to other sites in the body, although there is a risk that they will recur. There are different subtypes of these tumours with different potential to relapse. This paper gives an update of what is known about basal cell carcinomas and their treatment. The standard treatment is surgery. The prognosis for advanced basal cell carcinomas that cannot be operated on has improved with the development of systemic drugs targeting the hedgehog pathway.
Basal cell carcinoma (BCC) is a slow-growing skin tumour, which is commonly seen in dermatology. BCCs rarely metastasize, but are frequently multiple and recurrent on sun-exposed skin, with some morbidity. BCCs are a heterogeneous group of tumours, with histopathological and clinical characteristics ranging from superficial lesions to very extensive and destructive tumours. The standard treatment for BCC is surgery, but non-surgical options (medical, systemic or physical) have been developed in recent years for each end of the spectrum of these tumours: superficial lesions (sBCC) and advanced BCC (aBCC). Guidelines have been updated to help physicians with these different therapeutic strategies (1).
BCC is the most frequent skin cancer in fair-skinned adult patients (2). The estimated lifetime risk in this population is approximately 30% (3). The worldwide incidence of BCC is increasing continuously, but it cannot be estimated precisely as this tumour is not consistently registered. Marked geographical variations have been reported. The highest incidence is reported in Australia (up to 1,000/100,000 inhabitants per year, followed by the USA (212–407/100,000 female and male inhabitants respectively/year) and Europe (mean range from 76.21 /100,000 person-years in the UK to 157 per 100,000 person-years in 2009 in the Netherlands). This is within the range found in other European countries, such as Germany, France, Italy and Spain (4, 5). The lowest incidence is observed in Africa (<1/100,000 persons years).
BCC is most frequently seen after 50 years of age, with a female/male ratio of 2:1 (6). However, some patients develop BCC at an earlier age (<40 years). Patients with genetic predisposition syndromes, such as xeroderma pigmentosum (XP) or basal cell naevus syndrome (BCNS) can develop BCC earlier, even before 20 years of age (see the section on genetics, below). In the USA the ratio of cases of BCC to that of squamous cell carcinoma (SCC) was estimated at 4:1 and changed to 1:1 in 2012, but this is probably due to earlier SCC lesions being removed, which may have previously been treated non-surgically (7, 8).
The most significant risk factor for development of BCC is sun exposure, both in childhood and recreationally or occupationally in adult life (9). UVA, and mostly UVB, is implicated. This explains why most tumours are located on sun-exposed skin and are more frequent in fair-skinned people. BCC is the most highly mutated human tumour (65 mutations/megabase) (10). Another risk factor is immunosuppression, with a greater than 10-fold increase in BCC, especially in kidney transplant recipients (11).
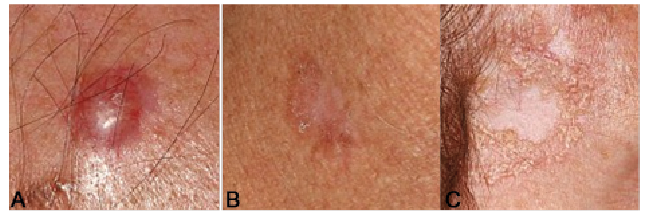
BCC develops from follicular and interfollicular keratinocyte stem cells (12, 13). Different clinical and histological types have been described with increasing invasiveness from superficial, nodular, morphoeic and basosquamous tumours (Fig. 1). Nodular lesions represent 60% of all BCCs and appear as nodules or papules with telangiectasia. Superficial lesions are flat, erythematous, and scaly with well-demarcated edges; more frequently found on the trunk of younger adults; and represent 20% of all BCC. Morphoeic lesions are scar-like whitish plaques with indistinct borders. These tumours can also be ulcerated and pigmented.
Fig. 1. Various basal cell carcinoma (BCC) clinical subtypes. (A) Nodular BCC. (B) Superficial BCC. (C) Morpheiform BCC.
In a review of 1,039 consecutive cases, Sexton et al. have found that most BCC are mixed (14). In these cases the most aggressive form defines the prognosis of the tumour. Basosquamous tumours are often found in advanced or difficult-to-treat lesions, which have been left without treatment for many years and are seen at an advanced stage. These lesions are classified as difficult-to-treat, in contrast to the former, which fall into the category of common BCC or easy-to-treat tumours unless they have specific management difficulty (1). In fact, these forms of difficult-to-treat BCC are heterogeneous and a classification system has been proposed by the European Association of Dermato-Oncology (EADO) and is under revision. These difficult-to-treat lesions often require imaging, with magnetic resonance imaging (MRI) or tomodensitometry, to determine the tumour extension.
Dermoscopy is useful to help with the diagnosis of BCC, revealing ovoid nests and globules, leaf-like areas, arborizing and superficial telangiectasias, erosions, pigmentation, but absence of pigment network. A recent study has shown that, in a comparison of naked eye examination and dermoscopy, the diagnosis sensitivity and specificity improved from 66.9% to 85% and 97.2% to 98.2%, respectively, with dermoscopy (15). Dermo-scopy may also help to recognize the histopathological subtype of BCC (16).
The diagnosis of BCC requires a biopsy, unless the lesion is small or clinically and dermoscopically typical, especially in non-high risk locations (trunk). A biopsy is recommended before proceeding to complex surgery or systemic treatment (1). The biopsy can confirm the diagnosis of BCC, but may not be adequate to appreciate the histological subtype in view of the heterogeneous histology.
Twenty years ago, the candidate gene (germline mutation) for patients with BCNS syndrome (a genodermatose predisposing to multiple BCCs and developmental defects) was reported to be the PTCH1 gene, leading to activation of the hedgehog pathway (Hh) (Fig. 2), which is a crucial event in the pathogenesis of BCC (17). PTCH1 (located on human chromosome 9q22) encodes a transmembrane protein negatively regulating smoothened (SMO), another transmembrane protein of the pathway. When PTCH1 binds to an extracellular ligand, such as sonic hedgehog, its negative control on SMO is relieved, allowing SMO to migrate in the cilium and activate Gli transcription factors (18, 19). Since then other germline mutations have been described in Gorlin’s syndrome, targeting PATCH2 and SUFU genes (20).
Fig. 2. Schematic view of the hedgehog (HH) pathway. When HH ligand binds to the transmembrane receptor PTCH1 it releases its inhibitory activity toward smoothened (SMO), which inhibits another negative regulator of the pathway SUFU leading to activation of GLI and GLI target genes. Hedgehog inhibitors are anti-SMO molecules. GLI is a transcription factor activated by SMO.
Activation of the Hh pathway has also been demonstrated in sporadic BCC, with 90% of the tumours bearing inactivating mutations of PATCH and 10% activation of SMO (21). These mutations are most often UV-induced: C>T transitions at dipyrimidines sites or even more specific CC>TT tandem mutations.
Inactivating the Hh pathway has been a major therapeutic goal for difficult-to-treat lesions and 2 oral-targeted therapies (hedgehog inhibitors or HhI) are currently available: vismodegib and sonidegib (1).
If the occurrence of mutations in the Hh pathway is considered to be the driver event toward formation of BCC, secondary drivers have been found in cancer genes, such as MYCN, PPPC, SK19, LATS1, ERBB2, PIK23C, N-RAS, K-RAS, H-RAS, PTPN14, RB1, and FBX7 (22). Other pathways that increase the transcription factor of GLI include a recently described loss-of-function mutation in SUFU in sporadic BCC and a variety of non-canonical hedgehog signalling pathways (the mammalian target of rapamycin (mTOR), insulin-like growth factor (IGF)–PI3K–AKT, epidermal growth factor receptor (EGFR)–MEK–ERK, and Hippo pathways) that are independent of ligand–PTCH1 binding and SMO activation (23).
The impact of these other mutations on the histopatho-logical characteristics and evolution of BCC or their response to systemic treatment is unknown.
Other genetic diseases can predispose patients to the formation of BC: XP due to germline mutations in DNA repair genes (24), which predispose to multiple skin tumours, including BCC, but also melanoma and squamous cell carcinoma (SCC), at an early age, as well as the Bazex-Dupre-Christol syndrome, and dominant X-linked cancer-prone genodermatosis, in which recent studies have reported mutations in the ACTRT1 gene and its enhancer, leading to activation of the Hh pathway in certain families (25).
BCC very rarely metastasizes; it estimated incidence of metastasis is 0.0028–0.55% (1). A recent review of published cases showed that median survival in case of distant metastases was 24 months, and 36.2% of those had systemic chemotherapies. Regional metastasis were shown to have a median survival of 87 months (26).
The major issues with BCC are local destruction and recurrence. Mortality is low. Risk of recurrence is influenced by the location of the tumour (H zone of the face), the histological subtype, perineural invasion, immunosuppression and prior recurrences. Severe forms of BCC are heterogeneous and rare. A retrospective study from the USA reported that the severe form of BCC accounted for approximately 0.8% of all cases of BCC (27), while another reported 10/100,000 persons (28). No TNM classification is available and a grading method to classify these difficult-to-treat BCC is currently being developed by the EADO group. These advanced tumours are often not measurable by Response Evaluation Criteria of Solid Tumors (RECIST criteria) and can destroy large anatomical surfaces without affecting survival (1).
Surgery
Surgery is the standard treatment for the majority of BCC (Fig. 3). Standard excision (SE) or micrographic surgery (Mohs) can be used according to the characteristics of the tumour (size, location, previous recurrences, histology) and the skills of the surgeon. Mohs is reserved for high-risk tumours, in recurrent BCC or BCC in critical anatomical sites. A prospective randomized trial comparing SE and Mohs showed a 10-year cumulative probability of recurrence for primary BCC of 12.2% for SE and 4.4% for Mohs and for recurrent BCCs of 13.5 for SE and 3.9% for Mohs (29).
Fig. 3. Schematic landscape of treatment options for basal cell carcinoma (BCC).
The margins used for SE depend of the BCC recurrence risk profile. Current guidelines suggest a range of peripheral margins between 2 mm and 5 mm in low-risk tumours and between 5 mm and 15 mm in high-risk lesions (1). It has been reported that the size of the BCC also correlates with the risk of subclinical extension with a 4 mm lateral margin sufficient to excise a < 2 cm BCC, while a tumour of > 2 cm and additional risk characteristics may need a minimal lateral margin of 13 mm for complete removal. Deep margins recommend excision to level of the fat or, in the face, to the level of fascia, perichondrium or periosteum (30).
Clinical and histological margins do not correlate, as tissue shrinkage is observed after fixation. There is no specific recommendation nor evidence-based data to re-excision in case of complete excision with narrow margins (1).
What to do in cases of incomplete excision?
Incomplete excision can be reported in 4.7–24% of SE (31), and can lead to recurrence in 26–41% after 2–5 years of follow-up. If incompletely excised lesions recur, it is recommended to re-excise with wider margins, as the risk of multiple recurrence can be as high as 50% once a positive-margin BCC has recurred after surgery (32).
Radiotherapy
Radiotherapy is a good alternative to treat BCC, especially in elderly patients. It is recommended for patients who are not candidates for surgery (due to morbidity, patient’s choice, advanced disease, etc.). Radiotherapy can use external beam radiotherapy, or brachytherapy or contact therapy, and this will depend on the size, location of the tumour, the team expertise and resources. It can also be considered, but has never been evaluated, as adjuvant therapy when re-excision of incompletely excised lesions is not possible or when there is perineural evasion.
Recent meta-analysis has reported an estimated recurrence rate of 3.5% with radiotherapy similar to that reported for surgery (1). Radiotherapy is contra-indicated in patients with BCC nevus syndrome (BCCNS), as it may cause further tumours in the field of irradiation
Medical treatments alternative to surgery in superficial lesions
Imiquimod. Imiquimod is an immune-response modifier, which is indicated for the treatment of superficial BCC and small nodular BCC in immunocompetent adults. It must be applied 5 times per week for 6 weeks. The major biological effects of imiquimod are mediated through agonistic activity towards toll-like receptors (TLR) 7 and 8 and consecutively, activation of nuclear factor kappa B (NFkB). The result of this activity is the induction of pro-inflammatory cytokines, chemokines and other mediators, leading to activation of antigen-presenting cells and other components of innate immunity and, finally, the mounting of a profound T-helper (Th1)-weighted anti-tumoural cellular immune response (33). Randomized comparative trials comparing 5% 5-fluorouracil (5-FU) with imiquimod 5% cream and MAL-PDT in patients with sBCC showed a treatment success of 72.8% for MAL-PDT, 83.4% for imiquimod, and 80.1% for 5% 5-FU at 1 year and 62.7%, 80.5% and 70%, respectively, at 5 years (31, 32).
The efficacy of imiquimod was also compared with surgery (S) for low-risk BCC and showed a successful response at 5 years, of 82.5% for imiquimod vs. 97.7% for surgery (34), confirming that imiquimod represents a good alternative to surgery for the treatment of sBCC.
Some local and general reactions can be observed with imiquimod, and patients should be informed of these.
5-Fluorouracil. 5-FU 5% is indicated for the treatment of sBCC (2 applications/day for 2–4 weeks), but very few studies have looked at long-term results. In the trial comparing 5-FU with imiquimod and PDT for the treatment of sBCC, 5-FU was shown to be inferior to imiquimod, but equivalent to MAL-PDT after 3 and 5 years (35).
Physically destructive treatments
Destructive treatments must be reserved for sBCC or small nodular BCC, as they evaluate the complete eradication of the tumour.
Photodynamic therapy. PDT with 5-aminolaevulinic acid (ALA) or its methyl ester (MAL) is indicated for sBCC and small nodular BCC (nBCC) less than 2 mm thickness. MAL-PDT gave clearance rates for sBCC of 92–97% and a recurrence rate at 1 year of 9%, which increased to 22% at 3 years and remained at the same rate at 5 years (36). MAL-PDT was also used and compared with surgery in nBCC and showed 91% clearance at 3 months and a sustained clearance rate of 76% at 5 years, inferior to surgery, but with cosmetic superiority. PDT with ALA nanoemulsion gel was shown to be as efficient as MAL-PDT in low-risk BCC (37).
PDT is a good option for patients with multiple superficial lesions, especially for lesions located on the back, on which application of imiquimod can be difficult.
Cryotherapy. Cryotherapy is indicated for low-risk BCC and has been shown to be as efficient as PDT in clinical trial (35). Its main advantage is the fact that it is an immediate procedure performed during the consultation. Its disadvantages are pain and the cosmetic results, as the treatment often leaves hypopigmented spots, which can last for years. Medical and physical treatments can be combined (i.e. PDT + imiquimod, rituximab and HhI, for example) (1).
Systemic treatments of difficult-to-treat or aBCC
Treatment of aBCC must be discussed in multidisciplinary committee.
Chemotherapy. No clinical trial has evaluated chemo-therapy for BCC. Most chemotherapies are platinum-based. The response rate is approximately 20–30%, but the duration of response does not exceed 2–3 months (26).
In addition, in elderly patients, chemotherapy can have life-threatening adverse effects. It is usually proposed as a second- or third-line treatment after failure of HhI.
Hedgehog inhibitors. Major progress has been achieved for the treatment of difficult-to-treat BCC with HhIs (35). Two molecules, with different pharmacokinetics, but targeting the same molecule, SMO, are available: vismodegib and sonidegib. No hed-to-head comparative studies are available. Vismodegib is indicated for laBCC (i.e. not a candidate for surgery or radiotherapy) and symptomatic metastatic BCC (mBCC) at a dose of 150 mg/day, while sonidegib is indicated for laBCC only, at a dose of 200 mg/day.
Vismodegib. Vismodegib was the first approved Hh inhibitor. The ERIVANCE study, an open-labelled non-randomized study, including 104 patients, showed, in the primary analysis, (using independent reviewer assessment) a 43% overall response rate (ORR) for a laBCC cohort, with 20.6% complete response (CR) and 22.2% partial response (PR). The response rate was 30.3% for the metastatic cohort (mBCC) (38). The median duration of response (DOR) was 9.5 (laBCC) and 7.6 months (mBCC). The 30-month update of ERIVANCE showed (using investigator assessment), an ORR of 60.3% for the laBCC (including 33 CR) and 48.5% for mBCC (only PR) and a DOR of 26.2 and 14.8 months, respectively (39). The median survival was 33.4 months for mBCC and was not reached for laBCC.
The STEVIE (SafeTy Events in VIsmodEgib) study, which enrolled the largest amount of patients (1,215, with 1,119 laBCC and 96 mBCC) had a main objective on safety. The secondary objective was efficacy and confirmed results obtained with the ERIVANCE study, with 68.5% of investigator-assessed objective response including 33.4 with CR for laBCC, and a median DOR of 23 months. For mBCC the ORR was observed in 36.9%, mostly PR, and a duration of response of 13.9 months (40). A subgroup analysis showed that BCCNS patients responded better to vismodegib. This was also observed in a clinical trial (41), which objective was to study the efficacy of vismodegib to shrink existing tumours and prevent formation of new BCC, both confirmed. However, long-term follow-up shows that all patients relapse after drug interruption (41).
In a recent report looking at long-term maintenance of CR after drug interruption, it was shown that 60% of patients have relapsed after 3 years of follow-up, with 40% (when BCCNS cases are excluded) having not relapsed at the time. Among relapsing patients, 48% had become eligible for surgery and 50% were vismodegib re-challenged and showed an ORR of 85% (42).
Sonidegib. The second HhI is sonidegib. The pivotal clinical trial Basal Cell Carcinoma Outcomes with LDE225 Treatment (BOLT) was a prospective randomized double-blinded trial comparing a once-daily dose of 200 mg with 800 mg. The 200 mg dose was approved based on the risk/benefit ratio. Evaluation used very stringent modified RECIST criteria showed a response rate of 36% (43). In the 12-month update analysis of the BOLT trial, the response rate for the 200 mg group improved to 57.6% for laBCC and 7.7% for mBCC (44). The Bolt follow-up of 30 months (45) reported a response rate of 56.1% (central review) and 71.2% (investigator review) for laBCC and 7.7% and 23.1% for mBCC. The median duration of responses was 26.1 months (laBCC) and 24.0 months (mBCC). The median survival has not been reached in the 2 groups.
Both vismodegib and sonidegib, which belong to the same class of drug, share common adverse events (most frequent: muscles cramps, dysgeusia, fatigue, hair loss and weight loss). These adverse events are observed in the majority of patients and lead to drug discontinuation in 30% of cases. No treatment-related deaths were reported. Different strategies have been proposed to prevent or manage the side-effects (46). Adverse events with sonidegib seem to be slightly less frequent and less severe, but this has not been evaluated in a comparative study. Some drug holidays have been proposed to overcome these side-effects (1)
The MIKIE trial has reported efficacy results of 2 intermittent regimens of vismodegib, and showed that it did not decrease efficacy (47). The neoadjuvant use of vismodegib has been reported in a small series, and showed that, among patients treated with vismodegib 3–6 months before surgery, only one recurred after 22 months (48). Some clinical trials are ongoing into HhI in the neo-adjuvant setting: Vismoneo (NCT02667574) and NICCI (NCT03035188).
Topical treatment. Earlier attempts with treatment at topical HhI failed, but a study is currently ongoing to evaluate the interest of a topical application of HhI on the face of patients with BCNS (NCT02828111).
According to the type of BCC observed, the follow-up can vary. Most BCCs are discharged after confirmation of diagnosis and completeness of excision. Some high-risk patients (multiple tumours, high-risk histological subtypes, high-risk anatomical sites, immunosuppression) will need to be followed up at least each year for up to 3–5 years. Difficult-to-treat BCC, which necessitated treatment other than surgery, are followed more carefully at a rhythm decided by the multi-disciplinary board (1).
BCC, being one of the most highly mutated tumours, could represent a good indication for immunotherapy.
Some isolated reports have shown response to anti-PD1 in treatment-naïve or HhI-refractory patients. In addition, a proof-of-concept study showed that pembrolizumab was efficient in patients with aBCC, but showed no increase efficacy when associated with vismodegib (49).
The efficacy of nivolumab, alone or in combination with ipilimumab, and of cemiplimab (REGN2810) is currently being investigated in patients with laBCC and mBCC in 2 independent phase 2 clinical trials (https://clinicaltrials.gov).
BCCs are the most frequent skin cancers, and their management has been thoroughly reviewed in recently published guidelines. Most BCCs have an excellent prognosis and do not need long-term follow-up. For high-risk tumours, the follow-up schedules may need to be adapted to each clinical presentation.
The standard treatment for BCCs is surgery. The understanding of molecular events implicated in their development has allowed the development of new strategies, such as HhI and, more recently, immunotherapy, for difficult-to-treat tumours.


 Click to show fullsize
Click to show fullsize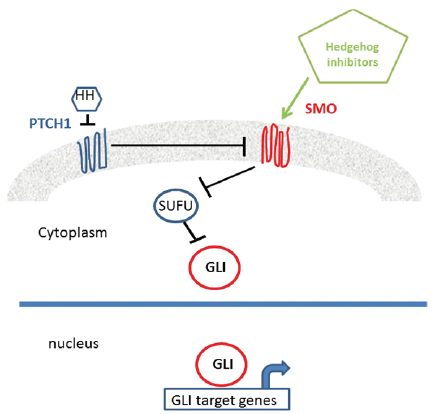 Click to show fullsize
Click to show fullsize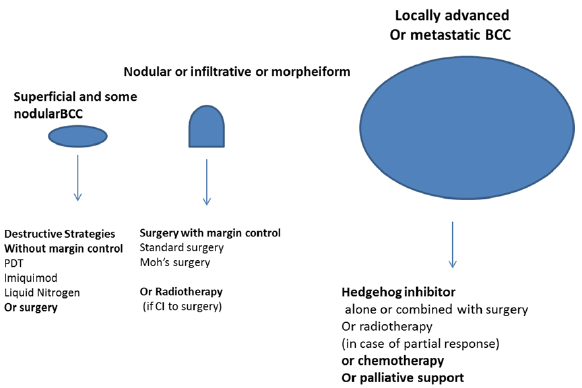 Click to show fullsize
Click to show fullsize