


1Department of Pathology and Molecular Medicine, McMaster Immunology Research Centre, McMaster University, Hamilton, Ontario, Canada, and 2Scientific Affairs (RG) and Chief Medical Officer (JFP), ’Kiniksa Pharmaceuticals Corp., Lexington, Massachusetts, USA
To evaluate cellular response to oncostatin M (OSM) in comparison to interleukin (IL)-31, we analyzed monocyte chemoattractant protein 1 (MCP-1) as a read-out for OSM responses with and without IL-4, IL-13, anti-OSM receptor β monoclonal antibody KPL-716, and anti–IL-31 receptor α antibody in human epidermal keratinocytes and human dermal fibroblasts in vitro. In human epidermal keratinocytes, OSM significantly induced STAT3 or STAT1 phosphorylation and synergized with IL-13 or IL-4 in elevating MCP-1. In human dermal fibroblasts, OSM results were similar, and leukemia inhibitory factor or IL-31 minimally activated STAT3 but not MCP-1. OSM significantly stimulated mRNA for type II IL-4 receptor and type II OSM receptor. KPL-716, not anti–IL-31Rα, significantly attenuated MCP-1 response to OSM and OSM + IL-4 in human epidermal keratinocytes and human dermal fibroblasts. OSM, not leukemia inhibitory factor or IL-31, synergized with IL-4 and IL-13 in human epidermal keratinocytes and human dermal fibroblasts, suggesting therapeutic potential of KPL-716 in inflammatory dermatologic diseases distinct from IL-31 inhibition.
Key words: pruritus; inflammatory skin diseases; interleukins; keratinocytes; signaling.
Accepted May 4, 2020; Epub ahead of print May 6, 2020
Acta Derm Venereol 2020; 100: adv00197.
Corr: Carl D. Richards, MSc, PhD, Professor, Pathology and Molecular Medicine, Director, McMaster Immunology Research Centre, McMaster University, 4016 Michael DeGroote Centre for Learning & Discovery, Hamilton, Ontario, L8S4L8 Canada. E-mail: richards@mcmaster.ca
Oncostatin M, part of the gp130 cytokine family that includes leukemia inhibitory factor, interleukin-6, and interleukin-31, is involved in inflammation, epidermal integrity, and fibrosis. To elucidate the role of oncostatin M in inflammatory diseases, this work characterizes the response of human epidermal keratinocytes and human dermal fibroblasts to oncostatin M. Furthermore, this work characterizes the in vitro effect of KPL-716, a fully human monoclonal antibody that specifically targets the oncostatin M receptor β chain to simultaneously inhibit interleukin-31 and oncostatin M signaling, on oncostatin M-stimulated keratinocytes and fibroblasts. Results demonstrate therapeutic potential for KPL-716 via its oncostatin M signaling inhibitory effect that is distinct from its interleukin-31 inhibition.
Oncostatin M (OSM) is part of the gp130 family of cytokines that includes leukemia inhibitory factor (LIF), interleukin (IL)-6, and IL-31 (1–4). OSM is recognized as a mediator between immune cells and connective tissue/stromal cells (1, 5, 6). Various cell populations produce OSM, including T cells, monocytes/macro-phages, dendritic cells, and neutrophils (1, 2). OSM has been implicated in inflammatory responses, connective tissue remodeling (1, 7), and keratinocyte regulation (8, 9); elevated OSM protein and mRNA levels occur in patients with rheumatoid arthritis, asthma, pulmonary fibrosis, and atopic dermatitis (8, 10–12). Human OSM interacts at either the LIF receptor complex (LIFRα/gp130 chains, the type I OSM receptor) or the specific OSM receptor complex (OSMRβ/gp130 chains, the type II OSM receptor) (1, 2). OSMRβ also forms a complex with IL-31 receptor α (IL-31Rα) to generate the receptor complex for IL-31 (13).
IL-31 is a proinflammatory cytokine involved in skin physiology, and expression of IL-31 is elevated in patients with atopic dermatitis and prurigo nodularis (13–17). KPL-716 (Kiniksa Pharmaceuticals Corp., Lexington, MA, USA) is a fully human monoclonal antibody that specifically targets the OSMRβ chain and simultaneously inhibits both IL-31 and OSM signaling (18). KPL-716 is under investigation as a potential treatment for pruritic, inflammatory, and fibrotic conditions. Notably, KPL-716 does not inhibit critical hematopoietic signaling through the type I OSM receptor (18). In a cynomolgus monkey model, KPL-716 attenuated the scratching response to supra-physiologic doses of IL-31 (19), and in the clinical setting a single-dose of KPL-716 improved pruritus in patients with atopic dermatitis (18). A humanized monoclonal antibody has been developed that targets the IL-31Rα chain, with demonstrated antipruritic effects in animals and patients with atopic dermatitis (20–22).
This in vitro study was designed to characterize the responses of human epidermal keratinocytes (HEK) and human dermal fibroblasts (HDF) to OSM in comparison to the cell responses to LIF and IL-31 using the chemokine monocyte chemoattractant protein-1/C-C motif chemokine ligand 2 (MCP-1/CCL2) as a readout, which recruits monocytes and other cells (e.g., dendritic cells and T cells) to sites of active inflammation (23). The study also assessed KPL-716 regulation of MCP-1/CCL2 responses in HEK and HDF compared with anti–IL-31Rα antibody.
Reagents, cell culture, and assay
Information about sourcing for reagents, cell culture, and assays used in these experiments are reported in Table SI. Protein level quantification by ELISA was completed as per the manufacturer’s instructions.
In vitro cell stimulations
To validate that the HEK and HDF cell lines respond to OSM, and that the response could be measured by expression of a typical chemokine (i.e., MCP-1/CCL2, implicated in inflammatory responses) and signal transducer and activators of transcription (STATs), both cell lines were stimulated with OSM 50 ng/ml and cell lysates were analyzed for mRNA and cell supernatants for MCP-1/CCL2 protein levels. Details of experiments are reported in Table SII (western blot), Table SIII (ELISA), and Table SIV (ELISA synergistic).
In vitro antibody-mediated neutralization
Details of the antibody-mediated neutralization experiment are presented in Table SV. All antibody and cytokine treatments were done in quadruplicate wells.
RNA extraction, real-time PCR, and Nanostring analysis
HEK and HDF cell culture extracts were homogenized using PureLink RNA MiniKit according to the manufacturer’s recommendations (Invitrogen, Life Technologies, Minneapolis, MN, USA). The levels of mRNA for CCL2 and the receptors (R) IL-13Rα1, IL-13Rα2, IL-2Rγ, IL-4R, OSMRβ, LIFR, IL-6ST (gp130), and IL-31Rα were assayed using Nanostring technology (Nanostring Technologies, Seattle, WA, USA) or quantitative real-time polymerase chain reaction (qRT-PCR).
Western blot
Cell lysates were loaded at 20 µg protein per lane onto 12% SDS-PAGE gels and separated by electrophoresis at 120V for 1 h, then transferred onto nitrocellulose membranes at 400 mA for 1 h. Membranes were blocked with Tris-buffered saline (TBS)/Odyssey® Blocking Buffer (LI-COR, Inc., Lincoln, NE, USA) and probed with primary antibodies pSTAT1, pSTAT3, pSTAT6, STAT1, and STAT3 (Cell Signaling Technology, Danvers, MA, USA) overnight at 4°C. Membranes were washed the following day with TBS + 0.15% Tween20 and incubated with secondary antibodies (anti-rabbit; LI-COR, Inc.) for 45 min at room temperature. Membranes were imaged using Odyssey® Imaging Systems (LI-COR, Inc.).
Statistics
Data were analyzed using GraphPad Prism version 7 software and presented as mean ± standard error of the mean (SEM). In vitro experiments shown are representative of a minimum of three separate experiments. One-way analysis of variance (ANOVA) was used to determine the statistical significance, which was defined as maximal p < 0.05 using GraphPad Prism, and p-values of < 0.01, 0.001, or 0.0001 are indicated in the individual figures.
Cell stimulations
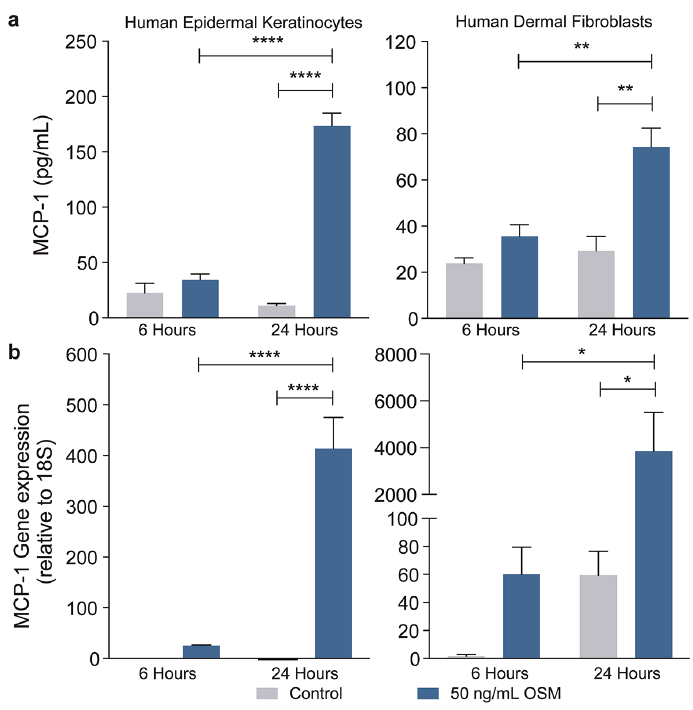
Following stimulation of HEK and HDF cells with OSM, MCP-1/CCL2 protein levels in supernatants were significantly elevated (p < 0.05) at the 24-h time point in both cell lines (Fig. 1a). RNA levels for MCP-1/CCL2 were also markedly elevated at the 24-h time point in both cell lines (Fig. 1b). At 6 h, levels of MCP-1/CCL2 appeared elevated but were not statistically significantly different.
Fig. 1. Oncostatin M (OSM) regulates MCP-1 in human epidermal keratinocytes (HEK) and human dermal fibroblasts (HDF). (a) MCP-1/CCL2 protein levels in supernatants were significantly elevated (p < 0.05) at the 24-h time point in both HEK and HDF cell lines; protein levels appeared elevated but were not statistically significantly different at 6 h (n = 4/treatment). (b) RNA levels for MCP-1/CCL2 were also markedly elevated at the 24-h time point in both HEK and HDF cell lines; RNA levels appeared elevated but were not statistically significantly different at 6 h (n = 3/treatment). Data represent mean ± SEM; two-way ANOVA; *p < 0.05; **p < 0.01; ****p < 0.0001.
To confirm activation of STAT3 by OSM (24–26) in HEK and HDF cells, we assessed activation of STAT3 as well as STAT1 and STAT6 in cell lysates at 30 min of stimulation in HEK (Fig. 2) and HDF (Fig. 3). We also compared OSM stimulus to LIF, IL-31 (also previously shown to signal through STAT3) (13, 27, 28), and IL-13, which activates the canonical STAT6 activation pathway. OSM 50 ng/ml stimulated pSTAT3 and pSTAT1 but not pSTAT6 signals as assessed by Western blot in both HEK (Fig. 2a) and HDF (Fig. 3a). Neither IL-31 nor LIF, used at higher concentrations of 100 ng/ml, induced detectable pSTAT3, pSTAT1, or pSTAT6 in HEK cells (Fig. 2a), whereas HDF showed a detectable increase in pSTAT1 and pSTAT3 in response to LIF or IL-31, but at much lower signal levels than OSM, and no detectable change in STAT6 (Fig. 3a). IL-13 stimulation induced pSTAT6 signals but not pSTAT1 or pSTAT3 in both HEK and HDF cells. TGFβ or LPA did not induce detectable changes in pSTAT1, pSTAT3, or pSTAT6 signals in either cell line. In both cell lines, the combination of OSM and IL-13 induced STAT1, STAT3, and STAT6 signal levels that were comparable with each cytokine alone. TGFβ co-stimulation with OSM did not result in any detectable difference in STAT3 or STAT1 levels from those induced by OSM alone.
Cultures of HEK and HDF cells were stimulated in parallel for these experiments, and 24-h culture supernatants were used for MCP-1/CCL2 protein analysis (Figs 2b and 3b). As in Fig. 1, OSM alone induced MCP-1/CCL2. In comparison, LIF, IL-31, IL-13, TGFβ, or LPA stimulation alone did not induce detectable changes in MCP-1/CCL2 levels. The combination of OSM and IL-13 resulted in a marked increase in MCP-1/CCL2 levels in both HEK and HDF, suggesting synergistic activity. Combinations of OSM with either IL-31 or TGFβ did not result in significantly different levels of MCP-1/CCL2 from those of OSM stimulation alone.
Fig. 2. Oncostatin M (OSM) induces STAT3 activation in human epidermal keratinocytes (HEK). (a) Western blot assessment of HEK showed that 30 min of OSM stimulation resulted in pSTAT3 and pSTAT1 but not pSTAT6 signals. Neither interleukin (IL)-31 nor leukemia inhibitory factor (LIF) induced detectable pSTAT3, pSTAT1, or pSTAT6. IL-13 stimulation induced pSTAT6 signals but not pSTAT1 or pSTAT3. TGFβ or LPA did not induce detectable changes in pSTAT1, pSTAT3, or pSTAT6 signals. The combination of OSM and IL-13 induced STAT1, STAT3, and STAT6 signal levels that were comparable with each cytokine alone. TGFβ co-stimulation with OSM did not result in any detectable difference in STAT3 or STAT1 levels from those induced by OSM alone. (b) ELISA analysis of protein in HEK supernatants showed that 24 h of OSM stimulation resulted in MCP-1/CCL2 induction, whereas LIF, IL-31, IL-13, TGFβ, or LPA stimulation alone did not. The combination of OSM and IL-13 resulted in a marked increase in MCP-1/CCL2 levels in HEK, while combinations of OSM with either IL-31 or TGFβ did not result in significantly different levels of MCP-1/CCL2 from those of OSM stimulation alone. Data represent mean ± SEM; one-way ANOVA; ***p < 0.001 vs control; †p < 0.0001 vs OSM alone.
Fig. 3. Oncostatin M (OSM) induces STAT3 activation in human dermal fibroblasts (HDF). (a) Western blot assessment of HDF showed that 30 min of OSM stimulation resulted in pSTAT3 and pSTAT1 but not pSTAT6 signals. HDF also showed a detectable increase in pSTAT1 and pSTAT3 in response to leukemia inhibitory factor (LIF) or interleukin (IL)-31, but at much lower signal levels than OSM, and no detectable change in STAT6. IL-13 stimulation induced pSTAT6 signals but not pSTAT1 or pSTAT3. TGFβ or LPA did not induce detectable changes in pSTAT1, pSTAT3, or pSTAT6 signals. The combination of OSM and IL-13 induced STAT1, STAT3, and STAT6 signal levels that were comparable with each cytokine alone. TGFβ co-stimulation with OSM did not result in any detectable difference in STAT3 or STAT1 levels from those induced by OSM alone. (b) ELISA analysis of protein in HDF supernatants showed that 24 h of OSM stimulation resulted in MCP-1/CCL2 induction, whereas LIF, IL-31, IL-13, TGFβ, or LPA stimulation alone did not. The combination of OSM and IL-13 resulted in a marked increase in MCP-1/CCL2 levels, while combinations of OSM with either IL-31 or TGFβ did not result in significantly different levels of MCP-1/CCL2 from those of OSM stimulation alone. Data represent mean ± SEM; one-way ANOVA; ***p < 0.001 vs control; †p < 0.0001 vs OSM alone.
To characterize the synergistic action of OSM with LIF or IL-31, we stimulated cells with either no co-treatment or co-treatment with OSM, LIF, or IL-31 with increasing concentrations of typical TH2 cytokines, IL-13, IL-4, and a comparator proinflammatory cytokine IL-17A. When we examined responses of HEK at 24 h (Fig. 4a, b, left panels), IL-4 or IL-13 alone did not induce MCP-1/CCL2 levels at any concentration assessed. Co-stimulation with OSM increased levels of MCP-1/CCL2 and increased concentrations of either IL-4 or IL-13, whereas co-stimulation with LIF or IL-31 did not result in any alterations. IL-17A alone did not induce MCP-1/CCL2, and co-stimulation with OSM did not result in any changes above that of OSM alone (Fig. S1, left panel).
Similar trends were seen in HDF cell production of MCP-1/CCL2 in response to IL-4 or IL-13, and no response was detected with IL-4 or IL-13 alone (Fig. 4a, b, right panels). Co-stimulation with OSM, but not LIF or IL-31, resulted in synergistic elevation of MCP-1/CCL2 released into supernatants. In contrast to HEK cells, OSM co-stimulation of HDF cells did result in elevated levels of MCP-1/CCL2 in response to increasing concentrations of IL-17A (Fig. S1, right panel). However, neither LIF nor IL-31 co-stimulation had a detectable effect.
Fig. 4. Oncostatin M (OSM) synergizes with interleukin (IL)-4 or IL-13 in induction of MCP-1 in human epidermal keratinocytes (HEK) and human dermal fibroblasts (HDF). (a) IL-4 stimulation alone did not induce MCP-1/CCL2 levels at 24 h at any of the concentrations tested. Co-stimulation with IL-4 and OSM increased levels of MCP-1/CCL2 in both HEK (left panel; passage 4) and HDF (right panel; passage 3) at 24 h, whereas co-stimulation with IL-4 and leukemia inhibitory factor (LIF) or IL-4 and IL-31 did not. (b) IL-13 stimulation alone did not induce MCP-1/CCL2 levels at 24 h at any of the concentrations tested. Co-stimulation with IL-13 and OSM increased levels of MCP-1/CCL2 in both HEK (left panel; passage 4) and HDF (right panel; passage 3) at 24 h, whereas co-stimulation with IL-13 and LIF or IL-13 and IL-31 did not. Data represent mean± SEM; two-way ANOVA; *p < 0.05 vs control; †p < 0.05 vs OSM alone.
In order to assess whether the synergistic action of OSM with IL-4 and IL-13 may involve the regulation of receptor components of IL-4 and IL-13 (29–31), we measured expression of the receptor chains for the IL-4 type I receptor complex (IL-4Rα/IL-2Rγ) and the type II IL-4R complex (IL-4Rα/IL-13Rα1) as well as IL-13Rα2. We also included analysis of the components of the OSM receptor (OSMRβ/gp130), the LIF receptor (LIFRα/gp130), and the IL-31 receptor (IL-31Rα/OSMRβ). Nanostring technology analysis was completed for HEK (Fig. 5) and HDF (data not shown). MCP-1/CCL2 levels were used as a quality control for validation of the Nanostring analysis in context of qRT-PCR (Fig. 1) and clearly show the robust elevation of MCP-1/CCL2 in both cell lines. In the HEK cell RNA quantitation, OSM induced IL-13Rα1 at 24 h and IL-4Rα at 6 and 24 h, but there was no significant upregulation of IL-2Rγ or IL-13Rα2 mRNA species. The levels of IL-13Rα2 and IL-2Rγ mRNA were very low (less than 40 relative units [RU], where 10 RU is considered non-detectable/background) and both IL-13Rα1 and IL-4Rα (1,000–2,000 RU) mRNA was upregulated. OSM stimulation elevated OSMRβ mRNA, but not LIFRα (very low RU) or gp130 in HEK cells (Fig. 5b). Finally, IL-31Rα mRNA levels were reduced, although the RU were relatively low (200 or less RU) compared with OSMRβ and gp130 (1,000–3,000 RU).
Fig. 5. Oncostatin M (OSM) stimulates mRNA for the receptor chains of type II interleukin (IL)-4 receptor and type II OSM receptor complexes in human epidermal keratinocytes (HEK). (a) RNA quantitation by Nanostring showed that OSM stimulation in HEK cells resulted in upregulation of IL-13Rα1 at 24 h and IL-4Rα at 6 and 24 h, but not IL-2Rγ or IL-13Rα2 mRNA species. (b) RNA quantitation by Nanostring showed that OSM stimulation in HEK cells resulted in upregulation of OSMRβ mRNA, but not LIFRα (very low RU) or gp130. MCP-1/CCL2 levels were used as a quality control for validation of the Nanostring analysis in context of qRT-PCR and clearly show the robust elevation of MCP-1/CCL2 HEK. Data are shown as Nanostring counts (relative units [RU]) corrected to 3 housekeeping genes (ACTB, PPIB, UBC). Data represent mean ± SEM; one-way ANOVA; *p < 0.05; **p < 0.01; ***p < 0.001; ****p < 0.0001.
The mRNA analysis of HDF cells showed the same trend as HEK in responding to OSM with increased IL-13Rα1 and IL-4Rα mRNA, very low levels of IL2Rγ, and no regulation of IL-2Rγ or IL-13Rα2 (data not shown). HDF cells responded with elevated OSMRβ mRNA, no statistically significant differences in LIFRα, and elevated gp130 mRNA. RU of IL-31Rα were low but did indicate a reduction of mRNA with OSM, similar to that observed in HEK. Collectively, the observations indicate that OSM can induce mRNA for the receptor chains of the type II IL-4 receptor and the type II OSM receptor in these cell types in vitro.
To assess the efficacy of the anti-OSMRβ antibody KPL-716, we compared KPL-716 modulation of MCP-1/CCL2 production in HEK and HDF cells with isotype control antibody and anti–IL-31Rα antibody (Fig. 6a–d; isotype antibody control data not shown). MCP-1/CCL2 levels were elevated similarly in the presence of no KPL-716 or 0.0001 μg/ml KPL-716, but were markedly reduced at KPL-716 concentrations of 0.001 μg/ml or higher (p < 0.01) in both cell types. There was no significant effect of anti–IL-31Rα antibody, and isotype control antibody did not affect MCP-1/CCL2 levels.
We further assessed OSM plus IL-4–stimulated cells to determine if KPL-716 or anti–IL-31Rα antibody would modulate the synergistic actions of OSM and IL-4 on MCP-1/CCL2 production. MCP-1/CCL2 was elevated in the presence of OSM and further elevated in the presence of OSM plus IL-4; MCP-1/CCL2 concentrations increased as the IL-4 stimulus increased from 5 to 20 ng/ml. KPL-716 preincubation reduced MCP-1/CCL2 levels at both levels of OSM plus IL-4 induction with the greatest effect observed at KPL-716 concentrations of 0.01 μg/ml and 0.1 μg/ml (p < 0.01 in HEK and p < 0.001 in HDF; Fig. 6e, g). No statistically significant effects were observed for any concentration of anti–IL-31Rα antibody (Fig. 6f, h) or control isotype antibody (data not shown).
Fig. 6. KPL-716 inhibits Oncostatin M (OSM)-induced and OSM + interleukin (IL)-4–induced MCP-1/CCL2 in human epidermal keratinocytes (HEK) and human dermal fibroblasts (HDF). (a) In HEK cells stimulated with OSM, those exposed to no or 0.0001 μg/ml KPL-716 had elevated MCP-1/CCL2, whereas those exposed to higher KPL-716 concentrations had markedly reduced responses. There was no significant effect of anti-IL-31Rα antibody (b). Similar results were seen in HDF cells (c, d). (e) In HEK cells stimulated with OSM plus IL-4, the MCP-1/CCL2 response was further elevated compared with OSM alone. MCP-1/CCL2 concentrations increased as the IL-4 stimulus increased. KPL-716 exposure reduced MCP-1/CCL2 levels at both levels of OSM plus IL-4 induction with the greatest effect observed at KPL-716 concentrations of 0.01 μg/ml and 0.1 μg/ml. No statistically significant effects were observed for any concentration of anti–IL-31Rα antibody (f). Similar results were seen in HDF cells (g, h). Data are mean ± SEM; two-way ANOVA; HEK: **p < 0.01, no antibody (not shown) or KPL-716 at 0.0001 µg/ml vs KPL-716 (0.001, 0.01, or 0.1 µg/ml). HDF: †p < 0.05 KPL-716 0.001 µg/ml vs 0.01 µg/ml; ‡p < 0.01 KPL-716 0.001 µg/ml vs 0.1 µg/ml. ***p < 0.001 KPL-716 0.0001 µg/ml vs 0.01 or 0.1 µg/ml.
This study demonstrated that OSM regulates expression of the proinflammatory chemokine MCP-1/CCL2 by HEK and HDF cells, and that OSM combination with typical TH2 cytokines, IL-4 and IL-13, produced a synergistic MCP-1/CCL2 response in both cell types. Furthermore, the anti-OSMRβ antibody KPL-716 inhibits these responses effectively and at low concentrations (Fig. 6). KPL-716 (0.0001 μg/ml) reduced both OSM induction and synergistic induction (0.01 μg/ml) of MCP-1/CCL2 protein production by OSM plus IL-4. The activity of KPL-716 compared with that of anti–IL-31Rα antibody on OSM-induced MCP-1/CCL2 reveals differential specificity of KPL-716 for the OSMRβ chain in HEK and HDF cells. The clinical efficacy and safety of KPL-716 inhibition of OSMRbeta were investigated in a phase 1b clinical trial where single-dose KPL-716 reduced pruritus in patients with moderate to severe atopic dermatitis as defined by a score of 7 or higher on the WI-NRS at screening (18). Improvement in WI-NRS began as early as week 1, evidenced by a reduction of 33% for patients who received KPL-716 and 18.5% for patients who received placebo. WI-NRS improvement increased through week 4 (43.8% and 21.2%, respectively). Patients receiving KPL-716 also reported reduced sleep loss compared with patients receiving placebo. These preclinical findings may provide rationale for the initial evidence of an anti-pruritic effect of KPL-716 in humans, and clinical development of this anti-OSMRβ antibody is ongoing as a potential treatment for chronic pruritic conditions. Thus, the current results here suggest that in addition to targeting the IL-31 receptor through OSMRβ, KPL-716 appears to have expanded effects on markers of inflammation mediated by OSM including MCP-1/CCL-2.
In comparison to OSM, LIF and IL-31 showed a lack of robust STAT1/3 activation and a lack of MCP-1/CCL-2 induction either alone or with IL-4/IL-13 combinations. This is consistent with the relatively low expression of receptor subunits LIFR and IL-31Rα at the mRNA level (Fig. 5) [compared to high OSMRβ and associated OSM-induced STAT1/3 signaling (Figs 2, 3)] and thus a lack of sufficient LIF and IL-31 receptor complexes available on these cells in this system. On the other hand, both cell types responded to IL-13 as shown by pSTAT6 activation (Figs 2 and 3). Since both cell lines showed very low expression of IL-2Rγ (component of the Type I IL-4 receptor) it is likely responses observed to IL-4 and IL-13 were the result of interaction of IL-4/13 through the type II IL-4R complex (IL-4Rα and IL-13Rα1). Since IL-4/IL-13 could not induce MCP-1/CCL2 protein release, this suggests that STAT6 activation alone was not sufficient to drive MCP-1/CCL2 expression in these conditions.
The combination of OSM and either IL-4 or IL-13 generated synergistic elevation of MCP-1/CCL2 expression and simultaneously activates the phosphorylation of STAT1, STAT3, and STAT6. Further study is required to determine if MCP-1/CCL2 mRNA levels and transcription are synergistically elevated with these combinations, and raises the question of whether the MCP-1 gene promoter contains response elements for either/all of these STAT transcription factors. The synergy may also be related to OSM induction of mRNA expression for type II IL-4 receptor chains, where both IL-4Rα and IL-13Rα were elevated. This effect may enhance the sensitivity of either HEK or HDF responses to TH2 cyto-kines, however confirmation of receptor chain protein induction awaits further analysis. Alternatively, other post-transcriptional regulating mechanisms, such as those affecting translation of proteins, are possible but this is currently unknown. In other experimental systems, OSM has been shown to increase IL-4 and IL-13 expression and upregulate their corresponding receptors IL-4Rα and IL-13Rα (9, 12, 29, 30, 32, 33, 34). Specifically, in fibroblasts and airway smooth muscle cells, OSM synergized with IL-4 and IL-13 to increase eotaxin production (30, 31, 33). Furthermore, induction of the type II OSM receptor chains suggests that OSM may also induce its own receptor expression (35, 36). Analysis of OSMRβ and gp130 protein levels and subsequent increased sensitivity to OSM stimulation awaits further study.
In conclusion, OSM induced MCP-1/CCL2 and synergized with IL-4 and IL-13 to further enhance the chemokine’s production by HEK and HDF cells. These functions suggest that OSM acts via the type II OSMR to contribute to keratinocyte and fibroblast involvement in inflammatory conditions. Since KPL-716 has specific and potent effects in regulating OSM-induced effects as shown here, blocking OSMRβ with KPL-716 has therapeutic potential in inflammatory disease including, but not limited to, those associated with IL-31.
This study was sponsored by Kiniksa Pharmaceuticals Ltd. Medical writing assistance was provided by Emily Plummer, a Kiniksa Pharmaceuticals Corp. employee, and in part by Peloton Advantage, LLC, an OPEN Health company, Parsippany, NJ, and funded by Kiniksa Pharmaceuticals Ltd.
Preliminary data from these studies were presented at the 77th Annual Meeting of the Society for Investigative Dermatology, May 8–11, 2019, Chicago, IL.
Conflicts of interest: CDR: This experimental work in CDR’s laboratory was funded by Kiniksa Pharmaceuticals Ltd. through a Research Agreement with McMaster University. FB and LH: None declared. JFP and RG are employees (current and past, respectively) of Kiniksa Pharmaceuticals Corp.


 Click to show fullsize
Click to show fullsize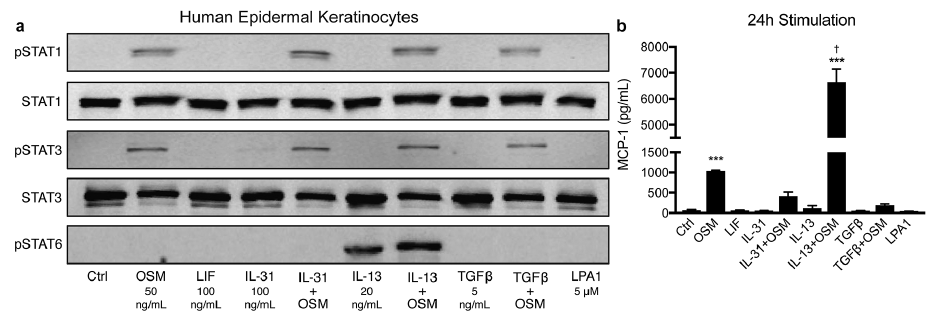 Click to show fullsize
Click to show fullsize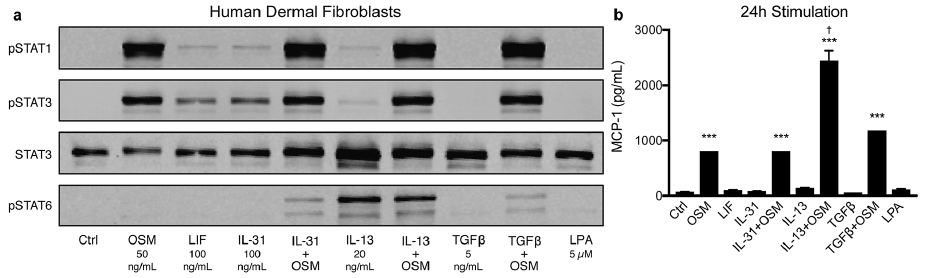 Click to show fullsize
Click to show fullsize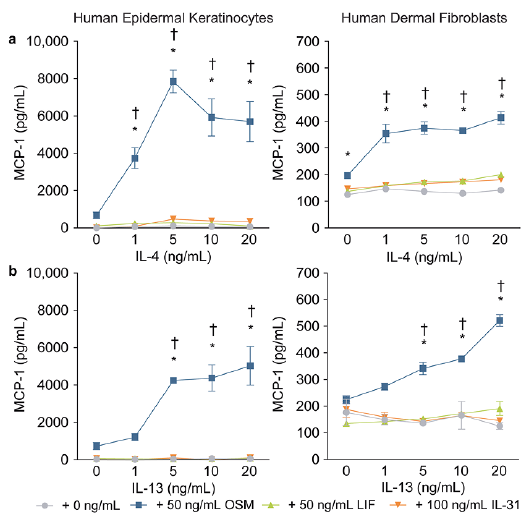 Click to show fullsize
Click to show fullsize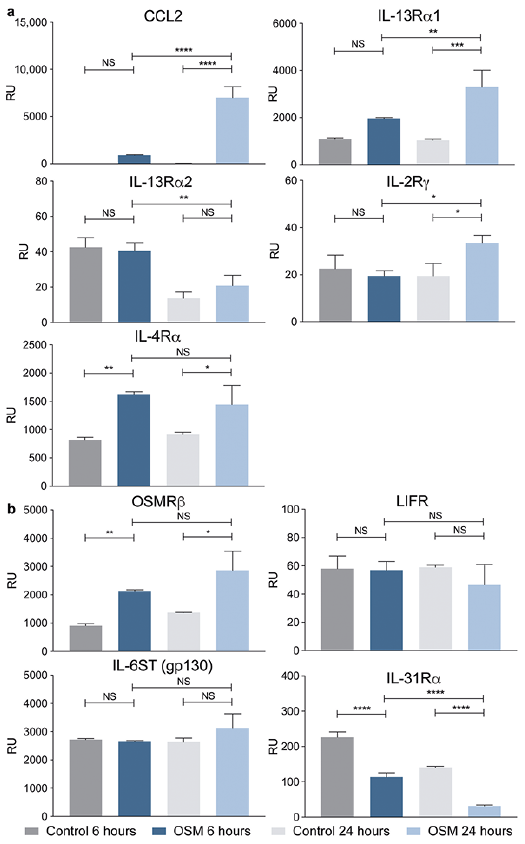 Click to show fullsize
Click to show fullsize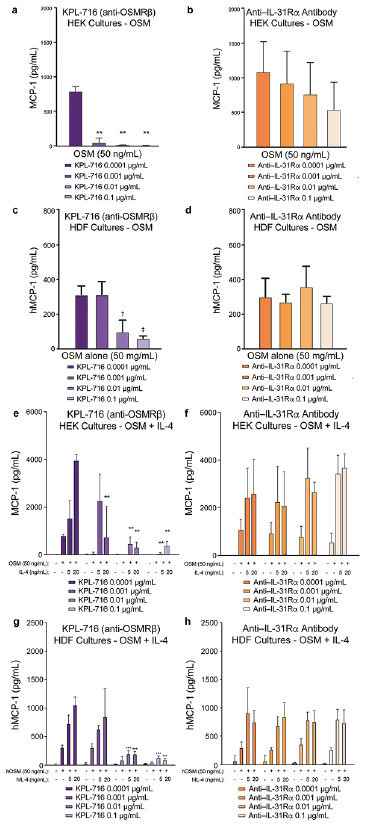 Click to show fullsize
Click to show fullsize