


1Technical University of Munich, School of Medicine, Department of Dermatology and Allergy, and 2Ludwig-Maximilians-University, Munich Medical Research School, Munich, Germany
Patients with genital psoriasis show poorer outcomes regarding quality of life and sexual distress than those without. This study aimed to assess the occurrence of genital psoriasis and to determine factors associated with the avoidance of sexual activities due to psoriasis in a non-clinical setting. A cross-sectional, person--centered, and online-based nationwide survey was conducted in Germany between March and June 2019. A multiple logistic regression model was used to analyze the data. Furthermore, free-text answers were provided. Overall, 344 individuals with psoriasis participated. Of these, 198 (57.6%) reported having genital psoriasis and 261 (75.9%) currently received medical care. Duration of psoriasis, subjective overall severity, and pain during sex were associated with the avoidance of sexual activities. Most prevalent rea-sons to avoid sexual activities were ‘shame,’ ‘pain,’ and ‘fear of rejection.’ Sexual distress was high in this sample and a person-centered care approach needs to be further promoted.
Key words: genital psoriasis; sexual behavior; sexual health; avoidance; people-centered; person-centered.
Accepted May 4, 2020; Epub ahead of print xx
Acta Derm Venereol 2020; 100: adv00151
Corr: Alexander Zink, MD, MPH, PhD, Department of Dermatology and Allergy, School of Medicine, Technical University of Munich, Biedersteiner Str. 29, DE-80802 Munich, Germany. E-mail: alexander.zink@tum.de
Patients with genital psoriasis have a poorer quality of life and more sexual distress. Therefore, we conducted an online-based nationwide survey across Germany addressing persons living with psoriasis. Overall, we had 344 participants. Of these, 198 (57.6%) stated to have genital psoriasis and 83 (24.1%) did not see a doctor at the moment. Most prevalent reasons to avoid sexual activities were ‘shame,’ ‘pain,’ and ‘fear of rejection.’ Avoidance of sexual contact is high in individuals reached via this online-survey and needs to be further addressed. Furthermore, the approach of reaching out affected individuals, not only patients, could represent a great asset for future health care.
Psoriasis affects approximately 2% of individuals in Europe, with an enormous psychosocial component among affected individuals and their families (1–4). Psoriasis can affect all parts of the body, including the genital area (3). The reported exam-based point prevalence of genital psoriasis ranges from 12 to 42% in patients with psoriasis. However, definitions of genital psoriasis vary between the studies (5). With growing knowledge about psoriasis (6, 7), its treatment is constantly progressing, and availability of highly effective treatment is increasing (8–10). When appropriately recognized, genital psoriasis can be treated specifically and sufficiently (11, 12).
Psoriasis is associated with many comorbidities, such as depression and anxiety (1, 13, 14). Additionally, mental health might be impaired due to negative influences on sexual health (15). According to the World Health Organization (WHO), the reduction of mental health comorbidities is important to improve people’s overall health (16, 17). Particularly, psoriasis patients whose genital area is affected showed an increased mental burden, poorer disease-specific quality of life, and higher sexual distress when compared to psoriasis patients without genital involvement (18–20). Although it is important that physicians assess the occurrence of genital psoriasis to prevent possible impairment of patients’ sexual heath (19,20), genital involvement often remains unnoticed (20). Another problem is that not all affected individuals seek medical healthcare from a physician (21–24). Therefore, the WHO encourages the concept of people-centered care, not patient-centered care, in order to broaden the scope of research and promote public health (21, 25). Additionally, the link between genital psoriasis and the avoidance of sexual activities has not been addressed sufficiently in the existing literature (19, 26, 27).
The aims of this study were (i) to assess the occurrence of genital psoriasis in a non-clinical setting, and (ii) to determine factors associated with the avoidance of sexual activities due to psoriasis from the perspective of affected individuals.
Study design
This cross-sectional study was designed as an online survey and carried out among individuals with psoriasis across Germany between March 2019 and June 2019. The survey was promoted on different channels (social media channels, webpages, and newsletters) by patient organizations, including “Psoriasis-Netz,” “Farbenhaut,” and a campaign of the Association of the German Dermatologists (BVDD), with different frequency of promotion and timespan of recruitment by each organization. Most people participated via “Psoriasis-Netz,” which is a patient organization website providing relevant and up-to-date information for individuals affected by psoriasis or interested in psoriasis treatment. The survey was shared within their monthly e-mail newsletter, which reaches up to 2,296 registered individuals across Germany. Additionally, they shared the link for the questionnaire on their webpage and social media accounts. “Farbenhaut” and the BVDD shared the link to the questionnaire on their social media pages one month before the survey was closed. Inclusion criteria were self-reported psoriasis diagnosed by a physician (all sub-types of psoriasis) and age at time of participation of 18 years or older. The only exclusion criterion was inability to fill out a German questionnaire. Prior to participation, all individuals provided electronic informed consent. Only individuals reported having a diagnosis of psoriasis made by a physician were included in the analysis. Entries with non-plausible values or with < 80% of questions answered were excluded. After completing the questionnaire, participants were directed to a page with web links that provided information about psoriasis, its comorbidities, and treatment options, as well as links to several local self-help groups across Germany. The study was approved by the local ethical committee of the Medical Faculty of Technical University of Munich (Reference: 25/19 S).
Questionnaire
The questionnaire was developed at the Technical University of Munich. Detailed information can be found in Appendix S1.
Statistical analysis
Data were collected using SoSci survey online tool (Version 3.2.02-i) (28). Descriptive statistics were provided for all variables. Differences between participants with or without genital psoriasis were analyzed using an unpaired t-test for continuous variables and a chi-square test for categorical variables. To assess factors influencing participants’ tendency to avoid sexual contact due to their psoriasis, univariate and multivariate logistic regression analyses were performed. First, the role of participant characteristics (age, sex, duration of psoriasis, severity of psoriasis in general and at time point of interrogation) and specific characteristics of participants’ sexual life (occurrence of genital psoriasis, relationship status, pain during sexual activities due to psoriasis) for the tendency to avoid sexual contact were tested. Second, all factors showing a significant association in univariate regression were included in the multivariate backward selection model. Odds ratios (ORs) and 95% confidence intervals (CIs) were calculated for both models. To avoid multicollinearity, correlations of all variables were calculated using Spearman correlations (rs) before inclusion in the multivariate model. Data management and analyses were performed using IBM SPSS Statistics 25 (IBM Corporation, Armonk, NY, USA). The level of significance (p-value) was set at 0.05.
Free text answers
To analyze, paraphrase, and categorize free-text answers to the question, why sexual contact was avoided, an inductive analyzing procedure using MAXQDA Analytics Pro software, version 18.0.0 (VERBI Software GmbH, Berlin, Germany) was conducted. Reasons given were subsequently categorized using an inductive approach, and categories were described quantitatively. Additionally, word counts were given for all specific words in this context, excluding non-specific words such as “the,” “and,” or “I.”
Study population
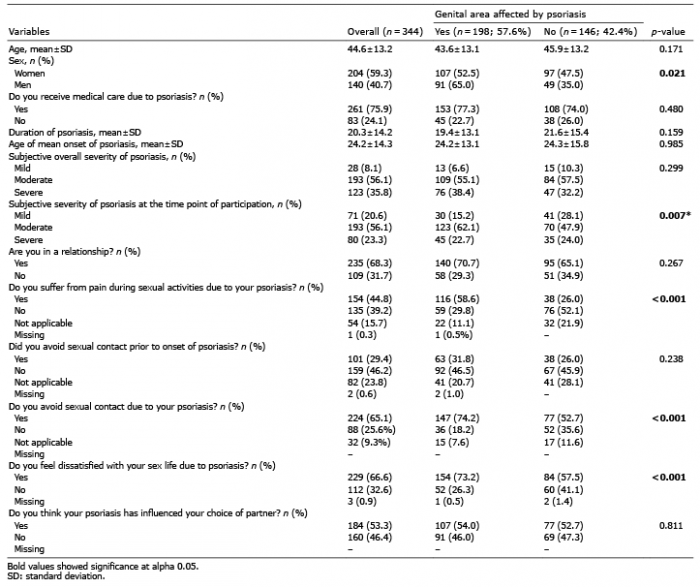
A total of 351 individuals with psoriasis completed the survey and 344 were included in the presented data (Fig. S1). The response rate of the institution including the most participants (“Psoriasis-Netz”) was 13.9%, when considering their e-mail newsletter. The participants’ mean age was 44.6 ± 13.2 years, and 59.3% of participants were women (Table I). Overall, 261 of 344 (75.9%) stated that they currently saw a physician due to psoriasis.
Table I. Baseline characteristics of total study population (n=344) and stratified by psoriasis involvement of genital area
Genital psoriasis and impact on sexual activities
More than half of the participants (n = 198; 57.6%) stated that their genital area was affected by psoriasis. Genital psoriasis was more prevalent in men than in women (65.0% vs. 52.5%; p = 0.021), and individuals with genital psoriasis were less likely to report subjectively mild psoriasis at the time point of participation (15.2% vs. 28.1%; p = 0.007). Overall, individuals reported an increased avoidance of sexual activities after onset of psoriasis (29.4% vs. 65.1%; Table I). No significant difference was observed between participants who later were or were not affected by genital psoriasis prior to psoriasis onset (31.8% vs. 26.0%; p = 0.238); however, more individuals with genital involvement tended to avoid sexual activities after psoriasis onset (74.2% vs. 52.7%; p < 0.001; Table I). The proportion of individuals stating that the question on avoidance was not applicable decreased after onset of psoriasis (23.8% vs. 9.3%). Of those participants avoiding sexual activities due to psoriasis, those with genital involvement more frequently reported to have changed their behavior from non-avoiding to avoiding (40.0% vs. 31.2%; Fig. 1). Of those reporting not to avoid sex due to psoriasis, most did not avoid sexual activities prior to onset either, regardless of the genital involvement (78.8–80.6%; Fig. 1). Individuals with genital psoriasis stated more often to “always” avoid sexual contact (13.6% vs. 5.5%, p = 0.001). Furthermore, participants with genital psoriasis more frequently expressed dissatisfaction with their sex life (73.2% vs. 57.5%; p < 0.001). More than half of all participants (n = 184; 53.3%) stated that psoriasis influenced their choice of partner, but no significant differences were observed between the sub-groups regarding genital psoriasis.
Fig. 1. Proportion of individuals avoiding sexual activities before and after onset of psoriasis. Additionally, avoidance after onset is stratified for involvement of genital area (n = 344).
Overall, 201 participants (71.8%) reported to avoid sexual contact at least sometimes due to their psoriasis. Correlation analysis showed fair correlations between higher age and longer duration of disease (rs 0.39; p < 0.001) as well as between genital involvement and pain during sex (rs 0.33; p < 0.001; Table SI). Univariate analyses revealed several factors that were significantly associated with avoidance. For example, people with a longer history of psoriasis were less likely (OR 0.98, 95% CI 0.96–0.99), whereas individuals with genital psoriasis (OR 2.76, 95% CI 1.66–4.58) or individuals who did not receive medical care (OR 1.85, 95% CI 1.07–3.20) were more likely to avoid sexual contact due to psoriasis. After using backward selection in the multiple logistic regression model, the remaining factors for the avoidance of sexual activities due to psoriasis were duration of psoriasis (OR 0.97, 95% CI 0.95–0.99), subjective overall moderate (OR 3.49, 95% CI 1.35–9.04) or severe psoriasis (OR 5.35, 95% CI 1.93–14.79), and pain during sexual activities due to psoriasis (OR 3.41, 95% CI 1.90–6.13) (Table II).
Table II. Factors associated with avoidance of sexual contact due to psoriasis in 312 study participants
Reasons to avoid sexual activities
Overall, approximately half of the participants stating to avoid sexual activities gave a reason for doing so as free-text answers (135 of 244; 55.3%). Categorization of reasons resulted in 180 classifications within 10 categories. Double categorization was possible in cases such as “Dandruff that falls out of the hair, itchiness.” Most prevalent categories were ‘Shame’ (n = 54; e.g., “Sometimes I don’t feel comfortable in my skin” or “I feel ashamed”); ‘Pain’ (n = 35; e.g., “The painful open wounds around the genital area” or in many cases just “Pain”); ‘Fear of rejection’ (n = 20; e.g., “I believe that my psoriasis is repulsive for others” or “I don’t want to see other people’s disgusted/deterred facial expressions”); and ‘Genital psoriasis’ (n = 14; e.g., “My penis really hurts when my skin cracks from the psoriasis,” and “Ashamed due to severe attack of the genital area”, Fig. 2a). Furthermore, statements were made on stigmatization during youth (e.g., “I believe that the exclusion due to psoriasis in my childhood still negatively impacts my body image or at least negatively impacted it for a while.”) and the need to explain the disease repeatedly (e.g., “The need to constantly explain my disease”). Most prevalent words used were “psoriasis” (n = 28), “shame” (n = 25), and “pain” (n = 24; Fig. 2b).
Fig. 2. Free text answers of affected individuals regarding the question for personal reasons for avoidance of sexual contact due to psoriasis. Font size in proportion to frequency of entries (actual font size equals square root of proportion times largest font size). (a) categories of reasons individuals mentioned as a reason to avoid sexual activities due to their psoriasis. Maximal mentioning: Shame, n = 54. (b) quantitative visualization of 20 most common words individuals mentioned during giving a reason to avoid sexual activities due to their psoriasis. Maximal mentioning: Psoriasis, n = 28.
The aims of the study were to assess the occurrence of genital psoriasis in a non-clinic setting and to determine factors influencing the avoidance of sexual activities due to psoriasis from the perspective of affected individuals. Of 344 participants with psoriasis, 198 had genital involvement. Individuals with genital psoriasis more frequently reported pain and avoidance of sexual activities due to their psoriasis than those without genital involvement. Furthermore, a shorter duration of psoriasis, an overall more severe psoriasis, and pain during sex were associated with the avoidance of sexual activities, which further led to sexual distress. Additional reasons included shame, pain, and the fear of rejection.
The occurrence of genital involvement was 57.6%, which is considerably higher than the rates reported previously (between 7% and 42%) (29–32). The high prevalence rate underlines the recommendation by Meeuwis et al. (19) that physicians should check for genital involvement in patients with psoriasis and pay attention to the impact of psoriasis on psychosocial aspects and sexual health. On one hand, prior studies conducted in medical settings may have underestimated the prevalence, as they did not include individuals who are not seeing a physician for the treatment of their psoriasis, which might be due to shame caused by genital involvement. Alternatively, the high prevalence in this study could stem from selection bias, as affected individuals might be more interested in taking part in a study about genital psoriasis. Nonetheless, in line with previous studies that have shown a prevalence of up to 42%, the prevalence in the present study may also indicate a vulnerable subgroup of individuals identified through patient organizations and non-healthcare professional settings. Additionally, the present results are in line with previous studies that report that men are more likely to develop genital psoriasis than women (20). These findings are important for dermatologists, as therapy can be optimized if knowledge of involvement of this hard-to-treat area is present. Therefore, communication with the patient about this topic is essential and barriers need to be minimized. Possible first approaches could include an improvement of physician-patient relationships or patient information on the frequency of genital psoriasis.
When considering the avoidance of sex before and after psoriasis onset, a clear change in participants’ behavior occurred (Fig. 1). Interestingly, the opinion that the question on avoidance of sexual activities was not applicable decreased after the onset of psoriasis. The reason for this might include individuals not having a partner before the onset of psoriasis, or participants not thinking of avoidance before onset and therefore, stating that they could not recall. Since these are interesting points, qualitative interviews or patient journey mapping could help to better understand these highly personal transitions.
An association between disease duration and the avoidance of sexual contact was found in this study, which is contrary to the findings of Zalewska et al., who did not find this association (33). This result indicates specific coping mechanisms that may have developed during the course of disease. The implications of such mechanisms should be further investigated.
Another important point regarding avoidance of sexual activities was the perceived pain during sexual activities, which was significantly correlated with genital involvement of psoriasis. Thus, genital psoriasis could be an important indicator of sexual avoidance, even when excluded due to backward selection (34). In a previous study, Ryan et al. also showed that people with genital involvement showed impaired quality of life and sexual health (29).
Interestingly, we found that the severity of psoriasis in general was significantly associated with the avoidance of sex, while the severity at the time of study participation was not. This indicates that participants might have interpreted the question “Do you avoid sexual contact due to psoriasis?” as a general tendency rather than a current behavior; this may be why there is an association with general disease severity, but not with current disease severity. Accordingly, the avoidance of sexual contact might be a coping mechanism applied by psoriasis patients (especially those with genital involvement) which helps them to avoid feeling shame or having to explain the disease to a sexual partner (which were reasons for the avoidance of sex mentioned in free text). However, it might also indicate the importance of people’s course of disease and the personal burden due to high severity, even though therapy may reduce visible symptoms. Accordingly, an additional measure of disease severity proposed by Zink et al., the lifetime highest Psoriasis Area and Severity Index (PeakPASI), may allow for more effective treatment (35). To evaluate the potential effect of this measure, more detailed and broader studies are necessary.
Free-text reasons given for the avoidance of sexual activities due to psoriasis were in line with the reasons previously reported in literature (19, 29, 36). Prior qualitatively gathered reasons like “Definitely the embarrassment… I’ve had one boyfriend make a comment, is that, what’s this?” or “The stinging during sex, it is just a terrible feeling” seem to be confirmed by aggregated data (36). However, the inclusion of ‘shame’ as the most prevalent category represents the importance of internal and external stigmatization in the context of visible skin conditions (2, 37).
Study limitations and strengths
When considering generalizability of study findings, several factors should be considered. One main limitation might be a potential selection bias, including a self-selection bias. Mainly individuals who actively searched for health information regarding psoriasis, or received a newsletter or updates on social media by multiplier institutions might have participated in this survey. Additionally, a self-selection bias could have occurred as individuals with an impairment of sex life or those with genital psoriasis could react more frequently to a survey on this topic. Furthermore, study promotion via patient organization web-pages, social media accounts, and mailing systems could have led to a highly vulnerable sub-group of individuals with psoriasis. This approach might increase diversity in individuals being described in the literature as accessibility of different populations can be challenging (23). To achieve high acceptance and unbiased free-text answers, we did not use validated and extensive questionnaires to measure sexual avoidance. This might have reduced comparability and generalizability. Additionally, the response rate of the most prevalent multiplier institution was only 13.9%, when considering all individuals receiving the monthly newsletter of the patient organization, which led the most individuals to participate. This response rate seems considerably low and could have been improved by directly addressing affected individuals, instead of only mentioning it on web pages, social media, or e-mail newsletters (38). However, it is unclear how many newsletter recipients fulfilled criteria for inclusion since subscribers also include minors, significant others or people with general interest in psoriasis. Therefore, interpretation of the response rate remains rather vague and should be considered with caution.
Furthermore, as the study was conducted online and participants stated to be diagnosed with psoriasis without control of this information, some individuals could have made incorrect statements. Even though statements were checked for plausibility by logical and time-wise criteria, the possibility of incorrect statements cannot be excluded with certainty but has to be accepted to widen the public health related horizon of populations with psoriasis. However, potential social desirability bias could have been minimized by the anonymous nature of this study. In the context of sexual content, the direct contact to a physician could have impeded participants’ willingness to answer questions freely out of shame or fear to feel judged or exposed (39). Therefore, the use of an anonymous online tool might have been highly beneficial. For comparison, German individuals frequently searched for “anal itch” as a localization for occurring pruritus (20% of search queries on localized pruritus) on Google. This online search for help or information seems to be due to social norms and does not reflect patient presentations in daily clinical routine (40). Additionally, 25% of participants are highly unlikely to have been reported in literature, as they do not see a physician for their psoriasis. This result is promising and could broaden the spectrum of epidemiological descriptions.
Conclusion
The occurrence of genital psoriasis was considerably higher in this potential vulnerably subgroup of individuals with psoriasis compared to other studies, and avoidance of sex due to self-given reasons like shame, pain and fear of rejection was high. This emphasizes the importance of patient organizations when reaching out for highly vulnerable groups and individuals who do not seek medical help. Furthermore, the subjective overall severity of psoriasis was significantly associated with the avoidance of sexual activities and the inclusion of PeakPASI could be a promising influencing factor for assessing the individuals’ mental impact or sexual impairment of psoriasis.
We want to thank all participants for their contribution. Furthermore, we want to acknowledge the role of Psoriasis-Netz (namely C. Liebram and R. Blaga) in the conceptual design of the study questionnaire and all help provided within the whole process of study implementation. Furthermore, we want to thank Psoriasis-Netz, Farbenhaut, and “Bitte Berühren”, a campaign of the Association of the German Dermatologists (BVDD), for sharing the link to the study questionnaire within their communities. We also want to thank S. Windels for bilingual translations of quotes given in the free text answers.
Conflict of interest: MCS received speaker’s honoraria and/or was financially supported for the presentation of scientific posters by Janssen-Cilag, Novartis. LT, BS and SZ were financially supported for the presentation of scientific posters by Novartis Pharma GmbH. TB provided advice to or received an honorarium for talks or research grant from the following companies: Celgene, Novartis, Lilly. AZ was an advisor and/or received speaker’s honoraria and/or received grants and/or participated in clinical trials of the following companies: AbbVie, Almirall, Celgene, Eli Lilly, Janssen-Cilag and Novartis.


 Click to show fullsize
Click to show fullsize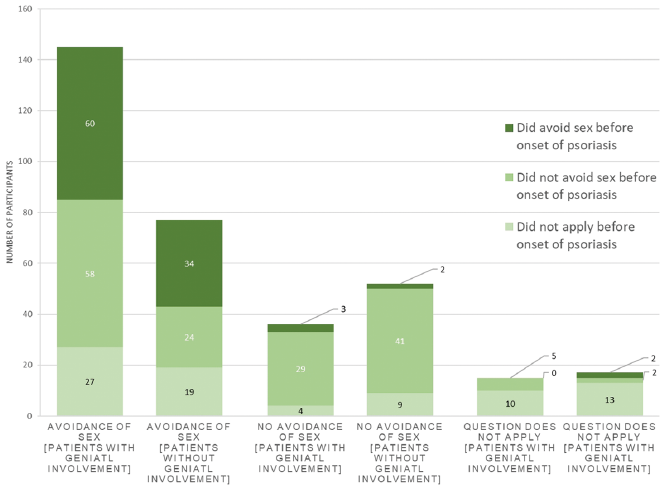 Click to show fullsize
Click to show fullsize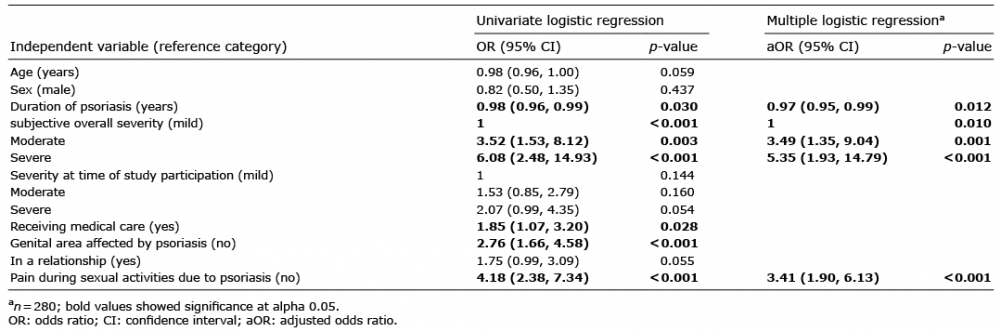 Click to show fullsize
Click to show fullsize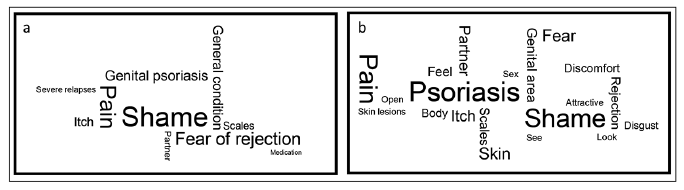 Click to show fullsize
Click to show fullsize