


Department of Dermatology, University of Rzeszów, Rzeszów, Poland
Prurigo nodularis is a chronic skin condition that presents significant challenges for treatment and quality of life, with little known about disease prevalence. This study assessed the prevalence of prurigo nodularis in Poland using publicly maintained database case records and diagnostic codes for prurigo nodularis (L28.1) and other prurigo (L28.2). For the period 2016–18, the prevalence of prurigo nodularis increased from 5.82 to 6.52 cases per 100,000 population. The total prevalence of all prurigo diagnoses over the same period remained relatively stable, with a small increase from 9.04 to 9.26 cases per 100,000 population. Regional data largely followed the overall trend. In an analysis of 58 prurigo nodularis cases identified at the Department of Dermatology at the University of Rzeszów, 43.1% of patients were initially misdiagnosed by the referring physician. Thus, more than one-third of patients with prurigo nodularis may initially be misdiagnosed.
Key words: epidemiology; International Classification of Diseases; population surveillance; prurigo.
Accepted May 11, 2020; Epub ahead of print May 18, 2020
Acta Derm Venereol 2020; 100: adv00155.
Corr: Adam Reich, Department of Dermatology, University of Rzeszów, ul. Szopena 2, PL-35-055 Rzeszów, Poland. E-mail: adamandrzejreich@gmail.com
Prurigo nodularis is a chronic skin condition that causes highly pruritic, nodular lesions. Treatment of prurigo nodularis is challenging and quality of life of patients is severely impaired. Awareness of the disease among physicians is often lacking and, therefore, prevalence numbers are likely to be underestimated. This paper describes that the prevalence of prurigo nodularis in Poland increased from 5.82 to 6.52 cases per 100,000 population over the period 2016–18. Patients are often misdiagnosed initially, indicating the need to raise awareness of the disease among physicians in general.
Prurigo nodularis (PN) is a chronic skin condition characterized by highly pruritic, nodular lesions. PN poses significant challenges for treatment and patient’s quality of life (1). Recently, the term “chronic prurigo” has been proposed as an umbrella term for various forms of chronic prurigo, as it covers various clinical presentations of prurigo, including papular, nodular, linear, plaque or umbilicated subtypes of prurigo, indicating that not only nodules, but also other skin lesion types, may be observed in this group of patients (2). However, as the International Classification of Diseases, Tenth Revision (ICD-10) considers PN as a distinct entity, this term is used for the study purpose, as it is used by the Polish physicians for reporting the clinical activities to the National Health Fund (NHF). All age groups (including children) may be affected by PN, but the disease tends to be more prevalent in older patients (3). Reliable data on the incidence and prevalence of PN are scarce, with little knowledge about the disease burden as a result (4). In Poland, where the majority of the population (approxi-mately 91%) have NHF insurance and all dermatology clinics are publicly funded, there is potential to assess the prevalence of PN using publicly maintained database records based on the entry of diagnostic codes for PN and other prurigo. This study aimed to determine the prevalence of PN using such data. A secondary objective was to assess whether there was any discrepancy between the initial diagnosis (i.e. a pre-referral diagnosis made by the referring physician) and any post-referral diagnosis of PN made by a dermatology specialist at a single clinic in Poland.
For this retrospective, observational, epidemiological analysis, data were requested from the NHF relating to the number of patients treated each year for PN or other prurigo for the period 2016–18. Cases were identified based on ICD-10 diagnostic codes, with L28.1 relating to PN and L28.2 to other prurigo. Case numbers were used to calculate prevalence rates. In order to determine the difference in the rates of diagnosis of PN by primary care physicians and specialists, data were accessed for patients who were hospitalized due to PN in the Department of Dermatology at the University of Rzeszów for the period 2016–18, and compared the diagnostic code assigned at the primary diagnosis (i.e. the diagnostic code on the referral letter) with the diagnostic code assigned by the consultant dermatologist after referral. The age of patients who were assigned an L28.1 or L28.2 diagnostic code was analysed using descriptive statistics and compared by sex and diagnosis using a paired t-test. The number of patients assigned either an L28.1 or L28.2 diagnostic code and who were seen by a specialist as an outpatient were compared using a χ2 test with Yates correction.
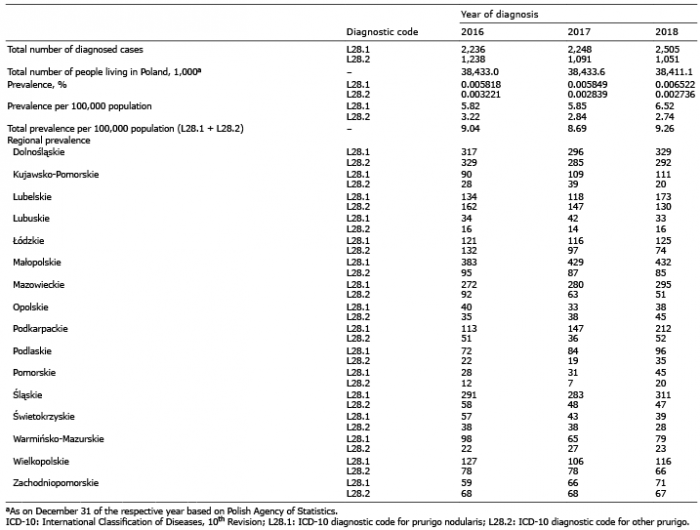
For the period 2016–18, the prevalence of PN in the Polish population increased slightly, from 5.82 to 6.52 cases per 100,000 population (Table I). Over the same period, the prevalence of other prurigo decreased slightly, from 3.22 to 2.74 per 100,000 population. The overall prevalence of prurigo remained relatively stable, with a small increase from 9.04 to 9.26 cases per 100,000 population over the 3-year observation period. Regional data largely followed the overall trend, although it was observed that the Kujawsko-Pomorskie, Ma?opolskie, Mazowieckie, Podkarpackie and ?l?skie voivodships (administrative provinces) had PN diagnosis rates (based on a recorded diagnostic code of L28.1) that were up to 5-fold higher than those for other prurigo (L28.2).
Table I. Prevalence of prurigo nodularis in Poland and breakdown of prevalence according to regional differences
The mean age of patients with PN was significantly higher than that of patients with other prurigo (61.5 vs. 57.6 years, respectively; p < 0.001); overall, females with PN were significantly older than males with PN (mean age 61.9 vs. 60.8 years; p < 0.01), and approximately twice as many females than males were diagnosed with PN or other prurigo (Table II). Of the 6,989 PN cases diagnosed during the observation period, 5,945 (85.1%) cases were outpatients seen by a specialist only, with the remainder seen as inpatients. Of the 3,380 cases of other prurigo diagnosed, only 328 (9.7%) were outpatients seen by a specialist only, with the remainder seen as inpatients (p < 0.001 for PN vs. other prurigo).
Table II. Age of patients with a diagnosis of prurigo nodularis or other prurigo and stratified according to sex (2016–18)
In the Department of Dermatology at the University of Rzeszów, 58 referred patients were diagnosed with PN during the observation period. Of the 58 patients, 33 (56.8%) were referred with a diagnosis of PN on the referral letter, and were thus correctly diagnosed by the referring physician; the remaining 25 patients (43.1%) had an initial diagnosis of a skin disorder other than PN, and were thus initially misdiagnosed. Misdiagnoses included pruritus, unspecified (ICD-10 diagnostic code L29.9; n = 4), encounter for observation for other suspected diseases and conditions ruled out (Z03.8; n = 3), other and unspecified dermatitis (L30; n = 2), and a single patient each diagnosed with dermatomyositis (M33), vitiligo (L80), unspecified dermatitis (L30.9), eczema herpeticum (B00.1), erythema nodosum (L52), mycosis fungoides (C84.0), nummular dermatitis (L30.0), factitial dermatitis (L98.1), hypertrophic lichen planus (L43.0), transient acantholytic dermatosis (L11.1), inflammatory papulous lesions on the skin not otherwise specified, other specified disorders of the skin and subcutaneous tissue (L98.8), non-pressure chronic ulcer of lower limb not elsewhere classified (L97), disorder of the skin and subcutaneous tissue unspecified (L98.9), personal history of other diseases and conditions (Z87), and cutaneous abscess, furuncle and carbuncle of the face (L02.0).
Based on current (2018) data, the estimated prevalence of PN in Poland is 6.52 cases per 100,000 population. Overall, the prevalence of any prurigo diagnosis remained stable in the Polish population between 2016 and 2018, with a slight increase in those diagnosed with PN (based on a recorded diagnostic code of L28.1) and a slight decrease in those diagnosed with other prurigo (based on a recorded diagnostic code of L28.2). It has to be emphasized that the code L28.2 refers to different types of pruriginous conditions, including, but not limited to, chronic prurigo. For instance, such conditions of different pathophysiology as “prurigo simplex subacuta” or “prurigo simplex” might also be reported under this code. It could be also suggested that the higher prevalence of PN observed over time accompanied by a slight decrease of frequency of other prurigo types may be related to the better awareness and better detecting of PN by physicians leaving fewer patients with “other prurigo”.
PN accounted for just 3.7 inpatient visits per 100,000 hospital discharges in the USA in 2016; the investigators believe this to be an underestimation, due to a lack of disease awareness among physicians (5). However, as data, including that for the general population, are limited, we are unable to speculate on this further. The mean age of a patient with PN in Poland (61.5 years) is similar as reported elsewhere for PN (6, 7).
In our analysis, more than one-third of all patients with PN were referred to the dermatology clinic with a diagnosis other than PN. Furthermore, the relative diagnosis rates of PN (based on a recorded diagnostic code of L28.1) and other prurigo (L28.2) were not always consistent across different voivodships (provinces) of Poland, with coding occurring at a similar rate in most voivodships, but up to 5-fold higher for PN vs. other prurigo in 5 further voivodships. Although it is speculative to suggest that case ascertainment for PN is more accurate in those 5 voivodships, it is conceivable that a general lack of disease awareness among physicians overall might contribute to an underestimation of the prevalence of PN (5).
Although use of the NHF database provided a unique opportunity to estimate the prevalence of an uncommon disease for which the burden is not well understood, there are limitations associated with this approach. Clinical coding is used to assign standardized diagnostic codes to a patient’s case notes primarily for billing and hospital reimbursement purposes; analyses of disease prevalence is a secondary purpose. Accurate database reporting is thus essential for analyses of the type reported here, as well as for reimbursement and billing purposes. In Poland, only the primary diagnosis is reported for medical coding; while simplifying clinical coding, this can lead to coding bias and underestimation of the true patient population. Clinical codes are often not assigned by the physician who makes the initial diagnosis, meaning there is potential for coding errors to occur due to misinterpretation of case notes, with the incorrect code subsequently being selected (8–10). There can also be issues with the available codes being unsuitable for recording certain diseases (11), and with coding accuracy differing across a range of diseases (12, 13). Coding omissions may also be higher for diagnoses made at secondary (vs. primary) visits (10). Such findings have implications for the use of national databases, and for the use of clinical coding as the basis for analyses of disease prevalence (8). Moreover, in countries where coding is used for reimbursement, the system is also open to potential misuse in order to record only diagnoses that lead to reimbursement (12), or to “up-coding” in order to increase reimbursement (14). Conversely, Clement et al. (9) reported improved accuracy with a coding proforma, which also resulted in increased billing when surgeons passed the simplified coding list to the coding department.
In conclusion, the present findings characterize the burden of PN in the Polish population. In contrast to other prurigo, which predominantly occurred in the inpatient setting, patients with PN were more likely to be diagnosed as outpatients. More than one-third of patients with PN may be misdiagnosed initially, suggesting ongoing efforts are needed to raise awareness of the disease among physicians in general.
Conflicts of interest and funding: AR has no conflicts of interest to declare. AR: Consultant or Speaker for AbbVie, Bioderma, Celgene, Chema Elektromet, Eli Lilly, Galderma, Janssen, Leo Pharma, Medac, Menlo Therapeutics, Novartis, Pierre-Fabre, Sandoz and Trevi Therapeutics. Principal Investigator or Sub-investigator in clinical trials sponsored by AbbVie, Drug Delivery Solutions Ltd, Galderma, Genentech, Janssen, Kymab Limited, Leo Pharma, Menlo Therapeutics, MetrioPharm, MSD, Novartis, Pfizer and Trevi Therapeutics.


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize