


Department of Dermatology, University of Groningen, Center for Blistering Diseases, University Medical Center Groningen, Hanzeplein 1, NL-9700 RB Groningen, The Netherlands. E-mail: m.a.lamberts@umcg.nl
Accepted May 11, 2020; Epub ahead of print May 19, 2020
Acta Derm Venereol 2020; 100: adv00156
Lichen planus pemphigoides (LPP) is a rare disease combining clinical and immunological features of lichen planus and bullous pemphigoid (BP) (1). Patients clinically present with intense pruritus, lichenoid papules and plaques, and tense blisters that occur on and outside of lichenoid lesions. Histopathology of a lichenoid lesion shows typical features of lichen planus, such as a band-like lymphocytic infiltrate, focal hyperkeratosis, hypergranulosis, and interface dermatitis with vacuolar changes at the basement membrane zone (BMZ) (2). In contrast, histopathology of skin taken at the edge of a blister reveals a subepithelial split, and perivascular infiltrate commonly including eosinophils and lymphocytes, compatible with a diagnosis of BP (3). Positive direct immunofluorescence (DIF) microscopy is a requirement for the diagnosis LPP, and shows skin-bound immunoglobulin (Ig)G, IgA or C3c in a linear pattern along the BMZ (3). Serum autoantibodies against BP180 and its non-collagenous 16A domain can be identified in the majority of patients with LPP, but also BP230 reactivity has been reported (1). These anti-BP180 and anti-BP230 autoantibodies can also be detected in serum and skin of patients with non-bullous pemphigoid, a pemphigoid variant that clinically lacks skin blisters (4). We report here a case of LPP without blisters, and introduce the term non-bullous LPP.
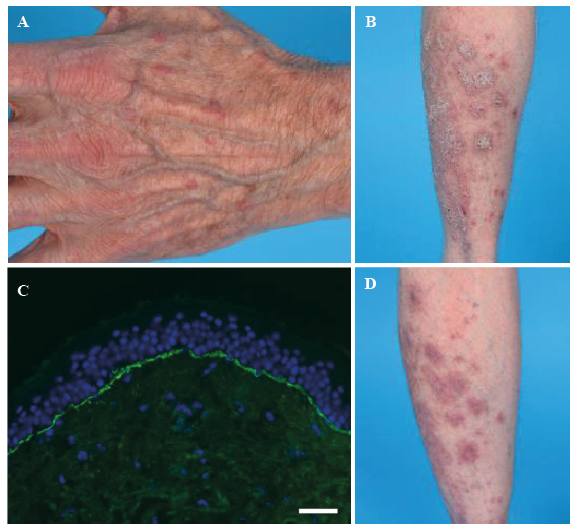
A 62-year-old man with a history of chronic obstructive pulmonary disease (COPD) and type II diabetes mellitus was referred to our tertiary centre with intense generalized pruritus, causing sleep deprivation in the last 2 years. The onset of pruritus was possibly related to the start of metformin. Skin examination showed nummular erythematous hyperkeratotic plaques with secondary excoriations, located mainly on both lower legs and, less extensively, at the upper legs. Moreover, we observed polygonal flat erythematous papules distributed over the whole body except the face (Fig. 1A,B).
Fig. 1. (A) Livid erythematous polygonal papules on the dorsal side of the hand. (B) Hyperkeratotic papules and plaques on the back of the left calf. (C) Immunoglobulin A (IgA) deposits linear along the basement membrane zone by direct immunofluorescence microscopy. White bar: 500 μm. (D) Reduction of hyperkeratotic lesions on the left calf after whole-body application of super potent corticosteroids for one month.
The hyperkeratotic plaques on the lower extremities were suggestive of a diagnosis of lichen planus, while the intense pruritic erythematous papules over the whole body suggested a diagnosis of non-bullous pemphigoid. Therefore, one lesional biopsy was taken for histopathology, and one perilesional biopsy for DIF microscopy.
Histopathological examination of a papule on the upper leg showed compact hyperkeratosis, a widened granular layer, and a band-shaped lymphocytic infiltrate resembling lichen planus. No microscopic blister formation was objectified. DIF microscopy demonstrated linear depositions of IgG (1+) and IgA (3+) in an n-serrated pattern along the BMZ (Fig. 1C). Serological tests detected circulating IgG against the non-collagenous 16A domain of BP180 (immunoblot 180 kDa positive; ELISA NC16A index 23 (MBL, Nagoya, Japan)). Based on these findings the diagnosis of non-bullous LPP was made.
Metformin was discontinued and replaced by gliclazide. Lesional topical steroids were previously not effective; therefore, whole-body application of clobetasol 30 g per day was started according to the guideline for management of BP (5). Initially, there was a good and rapid response with regard to the pruritus and skin lesions (Fig. 1D). However, the pruritic symptoms relapsed during tapering of whole-body application of clobetasol. Systemic therapy with methotrexate, 7.5 mg/week, was prescribed, with an excellent response with complete remission. Despite discontinuation of methotrexate 9 months later, due to recurring pneumonia, the patient remained in complete remission off therapy.
Lichenoid lesions, together with blisters, are considered the clinical hallmark of LPP, a disease linking pemphigoid and lichen planus (1). The current case report presents a patient with LPP lacking blisters, a disease termed non-bullous LPP. This entity was first published by Tan & Vaidya (6), describing a 42-year-old man with violaceous lichenoid papules located on both shins, possibly induced by venlafaxine (6). Remarkably, in both cases skin lesions were predominantly localized at the lower extremities, and the onset of symptoms were possibly related to the start of a new drug. Differences between the cases include the finding of a microscopic subepithelial split by Tan & Vaidya, which we did not observe. Moreover, Tan &Vaidya did not detect any circulating autoantibodies, while in the current case anti-BP180 autoantibodies were identified by immunoblot and ELISA.
The pathogenesis of LPP is not completely elucidated. In most reported cases lichenoid lesions precede blister formation (1). It is hypothesized that the T-cell driven lichenoid interface dermatitis by lichen planus “exposes” immunologically “hidden” epitopes to the immune system, provoking a B-cell driven autoimmune response (1, 7). This phenomenon is referred to as epitope spreading (8). LPP should not be mistaken with bullous lichen planus, in which blisters are exclusively located on lichenoid lesions (9). In bullous lichen planus, blisters are formed by extensive inflammation, causing degeneration of cells around the epidermal-dermal junction. Anti-BMZ autoantibodies in skin and serum are absent.
In our patient, the onset of disease was possibly related to the start metformin; however, cessation of the drug did not stop the pruritus. Several drug-induced cases of LPP have been published previously, with angiotensin-converting-enzyme inhibitors as the most reported culprit (10). Single reports on drug-induced LPP have also implicated psoralen, cinnarizine and simvastatin, but not metformin (10). Interestingly, one report describes metformin-induced lichen planus (11). In contrast, BP was associated with dipeptidyl peptidase IV inhibitors in several studies, but not with metformin monotherapy (12).
The exact prevalence of subepidermal auto-immune blistering diseases, such as cutaneous or mucous membrane pemphigoids, resembling or accompanying lichen planus is unknown. A recent case series describes 12 patients with mucous membrane pemphigoid, clinically and histologically resembling oral lichen planus (13). The diagnosis of such cases is greatly dependent on the performance of DIF by clinicians. This may also apply to non-bullous LPP, and more research is needed to determine its true incidence. Interestingly, mucosal lichen planus was previously associated with low titres of circulating anti-BP180 autoantibodies and, more recently, with reactivity of T helper 1 and T helper 17 cells against both desmoglein 3 and BP180 (1, 14, 15). Yet, the relevance of these findings and the likelihood that these patients develop pemphigoid remains unknown.
This case highlights that non-bullous LPP can be a cause of pruritus in patients with lichenoid lesions, and illustrates that systemic therapy might be required to achieve long-term remission. We advise clinicians to perform pemphigoid diagnostics in patients with pruritic lichenoid lesions refractory to topical steroids, in order to examine whether non-bullous LPP could be diagnosed.


 Click to show fullsize
Click to show fullsize