


1College of Physicians and Surgeons, Columbia University Vagelos, New York, USA, 2Department of Dermatology and 4Pathology Department, APHP, Saint-Louis Hospital, Université de Paris, 1 avenue Claude Vellefaux, FR-75010 Paris, and 3Université de Paris, INSERM U976, Paris, France. *E-mail: martine.bagot@aphp.fr
#These authors contributed equally.
Accepted May 18, 2020; Epub ahead of print May 25, 2020
Acta Derm Venereol 2020; 100: adv00158
Mogamulizumab is a first-in-class monoclonal antibody directed against the chemokine receptor CCR4. It is approved for use in relapsed/refractory mycosis fungoides (MF) and Sézary syndrome (SS) following at least one prior systemic therapy (1). Autoimmune reactions after therapy with checkpoint inhibitors and mogamulizumab have been described in the literature and are probably associated with favourable treatment response (2). We describe here a patient with a mucocutaneous lichenoid reaction after treatment with mogamulizumab, who showed improvement in clinical symptoms.
A 60-year-old woman was managed at Hôpital Saint-Louis for plaque-stage MF (T2N0M0B0). Initial treatments included ultraviolet A (UVA) and psoralen, methotrexate, bexarotene extracorporeal photopheresis, and mechlorethamine gel. The patient had disease relapse and, at that time, she had a diagnosis of MF with a modified severity weighted assessment tool (mSWAT) score of 43 and B0 blood involvement.
Mogamulizumab was initiated in January 2019 (mSWAT 26 treatment day 1), due to insufficient response to 5 first-line therapies and the severe involvement of the palms significantly impacting her quality of life. The treatment was well tolerated, leading to improvement in cutaneous disease (mSWAT of 6 at month 7) (Fig. 1). After 8 months of treatment, an isolated striated oral leukoplasia developed on the right inner side of the upper lip (Fig. 2). The lesion was asymptomatic with no pain or pruritus. Histology showed a hyperplastic orthokeratotic epithelium, Civatte bodies and mononuclear epithelial and chorion infiltration, interpreted as lichenoid reaction. There was no change in the medication timing or dosage that could be related to the development of the lichenoid mucosal reaction. Due to good clinical outcomes and low severity, mogamulizumab was continued and treatment with topical corticosteroids was initiated. After a few weeks the lesions improved (Fig. 2). Three months after development of the oral lichenoid lesion, genital lichen planus developed. This lesion was also asymptomatic and resolved completely with topical steroids and continuation of mogamulizumab.
Fig. 1. Clinical images (A) before and (B) after 8 months of treatment with mogamulizumab. mSWAT, improved from an initial score of 43 to 6 after treatment.
Fig. 2. (A and B) Mucocutaneous lichenoid reaction that presented 8 months after initiation of treatment with mogamulizumab. (C and D) Resolution of the mucocutaneous lesions after treatment with topical corticosteroids.
Autoimmune manifestations after mogamulizumab, including autoimmune hepatitis, alopecia areata, autoimmune thyroiditis, and autoimmune haemolytic anaemia have been described (2, 3). These respective patients had long-term disease remission without maintenance therapy, suggestive of an association between autoimmune reactions and durable treatment response. Cutaneous reactions, including one lichen nitidus-like eruption, have also been reported for mogamulizumab in diseases other than MF (4). One case series found improved treatment responses in 6 patients with cutaneous granulomatous drug eruptions (5), and a study of 72 patients with adult T-cell leukaemia-lymphoma found that cutaneous adverse events were a favourable prognostic indicator (3). Mucocutaneous lichenoid reaction may result from a heightened immune response after immunotherapy. Larger studies may examine whether this reaction is also a favourable prognostic indicator to therapy.
Lichenoid reactions have been observed as an adverse event of treatment with various biologic agents (Table SI). They are well described in patients treated with tumour necrosis factor alpha (TNFα) inhibitors (6–8), and TNFα inhibitor biosimilar drugs, such as CT-P13. It has been suggested that lichenoid reactions may be more frequent with TNFα inhibition due to upregulation of interferon α by activated plasmacytoid dendritic cells causing cytokine release and inflammation (6). Lichenoid reactions have also been reported with the CD20-inhibitor rituximab (9). Immune checkpoint inhibitors anti PD-1/PD-L1 alone, or in combination with CTLA-4 antibody, may also be associated with lichenoid reaction (4, 10–13). Case reports have described lichenoid eruptions after treatment with the IL-17A inhibitor secukinumab (14). These lichenoid-type eruptions can be controlled with topical steroids (11). While these drugs have very different targets, similar lichenoid reactions have been observed. We propose that lichenoid reactions are not agent-specific, but rather an adverse event of biologics as a class.
Not all biologic drugs have been associated with lichenoid reactions. These adverse effects have not been published for dupilumab, omalizumab, ustekinumab, and brentuximab vedotin. Omalizumab and ustekinumab have unique mechanisms of action, which may not be associated with the lichenoid reactions. Dupilumab and brentuximab vedotin are newer agents and it is possible that this side-effect has not yet been recognized. In addition, it is possible that the lichenoid reaction may be misinterpreted by non-dermatologists as psoriasis.
This case also shows the utility of mogamulizumab in a patient with B0 blood involvement, although typically the best overall response is demonstrated in patients with stage IV disease (36%) or SS (37%) (1), both of which have >B2 blood involvement. A post-hoc analysis of the same trial examined the efficacy of mogamulizumab in early stage IB and IIA MF patients. Median time to next treatment was longer in the group treated with mogamulizumab compared with vorinostat (IB 11.5 vs 3.1 months; IIA 10.1 vs 4.9 months) and overall response rate was similar in stage IB patients (20% vs 18.5%) and higher in stage IIA patients (19% vs 0%) (15).
This report adds to the current literature of lichenoid reactions following biologic therapy. We believe such eruptions are class-related adverse events common to biologics, rather than drug specific. To our knowledge, mucocutaneous lichenoid reactions have not previously been reported in the context of mogamulizumab treatment for MF. This case shows that mogamulizumab can be an effective treatment in a patient without blood involvement, and that treatment may be continued with mild adverse events, such as mucocutaneous lichenoid reactions. In certain cases, autoimmune reactions under mogamulizumab may be favourable prognostic indicators (2); however, this needs further investigation. Topical management of the mucocutaneous lichenoid reactions may be an important strategy to alleviate symptoms when the reactions are not severe, allowing for the continuation of therapy.


 Click to show fullsize
Click to show fullsize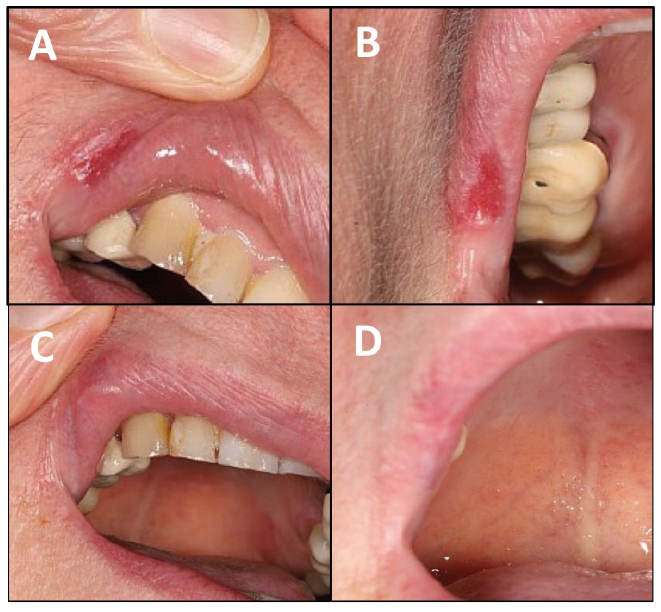 Click to show fullsize
Click to show fullsize