


Departments of 1Dermatology and 2Pathology, CHRU Tours, FR-37044 Tours, 3Department of Infection Diseases, Department of Cardiology, and 4UMR Inserm U1253, University of Tours, Tours, France. *E-mail: machet@univ-tours.fr
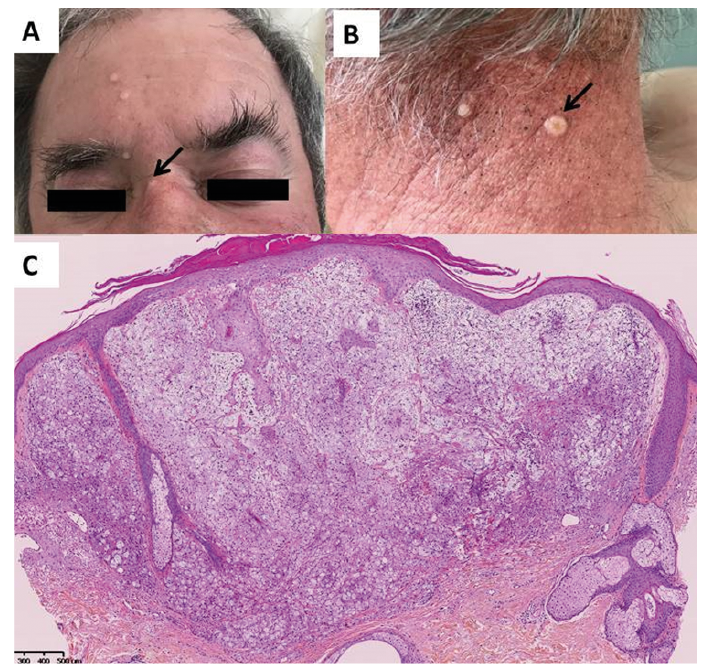
A 62-year-old male farmer presented with fever, rapidly increasing dyspnoea, headache and papules on the face and neck (Fig. 1). The centre of some of the lesions was umbilicated (Fig. 1A, B, arrows). His medical history included ischaemic heart disease, requiring a heart transplant in 2016, that was treated with tacrolimus 1.6 mg/day, everolimus 0.5 mg/day and prednisone 5 mg/day. In 1985, the patient had Hodgkin lymphoma, which was treated with radiation therapy and chemotherapy. A cutaneous biopsy was taken of a papule on the neck (Fig. 1C).
What is your diagnosis? See next page for answer.
Fig. 1. (A, B) Papules on the face and neck of a 62-year-old man. Note the umbilicated surface of some lesions (arrows). (C) Haematoxylin-eosin-stained skin biopsy specimen at low magnification (x20).
Acta Derm Venereol 2020; 100: adv00213.
Diagnosis: Cutaneous cryptococcosis resembling molluscum contagiosum
Histology of a skin biopsy revealed layers of clarified histiocytes with more or less clear limits, containing myriad spherical fungi 4–20 μm in diameter (Fig. 2A). These mycelial structures were stained with periodic acid-Schiff, Alcian blue (not shown) and Grocott’s stain (Fig. 2B). Culture confirmed a diagnosis of infection due to Cryptococcus neoformans.
In addition to skin involvement, the patient presented systemic involvement of the disease: interstitial syndrome of the lung on thoracic computed tomography (CT) scan and isolation of cryptococcus in bronchoalveolar secretion. Cryptococcus was present in cerebrospinal fluid, urine and blood cultures.
Treatment with amphotericin B, 3 mg/kg/day, and flucytosine, 100 mg/kg/day, was initiated but because of renal failure had to be changed to fluconazole, 400 mg/day, which is ongoing.
Cryptococcosis is an infection caused by the encapsulated yeast C. neoformans (1). C. neoformans contains 2 pathogenic varieties: C. neoformans var neoformans and C. neoformans var gatti. C. neoformans is widely distributed, and C. gatti is more prevalent in tropical areas. Cryptococcus neoformans is found in bird droppings and nests and in several tree species. Severe infections mostly concern immunocompromised patients (1–3). Cutaneous lesions occur in 10–20% of patients with systemic cryptococcosis and can precede other systemic manifestations. The presentation of cutaneous cryptococcosis can be polymorphic (4, 5). Cutaneous cryptococcosis mimicking molluscum contagiosum was previously described, initially in individuals with AIDS (6–10), then in other immunocompromised individuals (9). Skin lesions are scattered predominantly over the face and appear as dome-shaped, firm, well-defined, umbilicated papules (9, 10). These lesions usually indicate a disseminated form of the disease, and their identification can lead to the diagnosis.
Fig. 2. (A) Haematoxylin-eosin staining ×200: multiple fungal structures within histiocytes. (B) Grocott’s staining ×400: capsulated yeast cells.


 Click to show fullsize
Click to show fullsize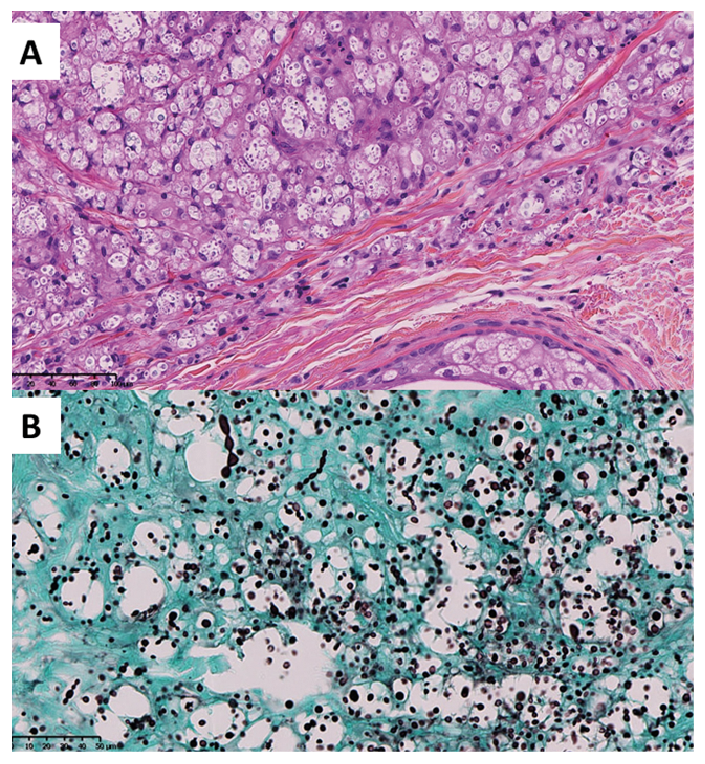 Click to show fullsize
Click to show fullsize