


1Psoriasis Research and Treatment Center, 2Interdisciplinary Group of Molecular Immunopathology and 4Berlin-Brandenburg Center for Regenerative Therapies, Dermatology/Medical Immunology, Charité-Universitätsmedizin Berlin, and 3Dermatology Practice Nußbaum und Grunow, Berlin, Germany
Psoriatic nail symptoms are frequent in psoriasis, affecting up to 80% of patients. Therapy responses to nail symptoms are often limited. In this multicentre non-interventional prospective study, 267 patients with nail involvement were treated with adalimumab for a period of 24 months. The efficacy of adalimumab for nail psoriasis was evaluated and predictors for better response were identified. For statistical analysis Kolmogorov-Smirnoff, Mann-Whitney U, Wilcoxon, χ2 and two-tailed Spearman’s rank correlation tests were applied. After 3 and 6 months, reductions in Nail Psoriasis Severity Index (NAPSI) of 32.8% (p < 0.001) and almost 50% (p < 0.001), respectively, were observed, compared with baseline scores (mean NAPSI score, 34.2 ± 1.3). In 6 months, 60.0% of patients achieved NAPSI50, 36.4% NAPSI75, and 21.7% NAPSI90. Approximately 42% and 60% of patients achieved NAPSI90 after 12 and 24 months, respectively. At month 12, reduction in NAPSI significantly correlated with improvement in Dermatological Life Quality Index. Stratification by age, sex, and body mass index indicated that treatment was more effective in younger patients and those with higher body mass index. Adalimumab is an effective long-term therapy for nail psoriasis. The amelioration of nail symptoms correlates with an improvements in the skin disease and quality of life.
Key words: psoriasis; nail psoriasis; nail psoriasis severity index; Dermatology Life Quality Index; adalimumab.
Accepted May 28, 2020; Epub ahead of print Jun 8, 2020
Acta Derm Venereol 2020; 100: adv00214.
Corr: Georgios Kokolakis, Psoriasis Research and Treatment Center, Clinic of Dermatology, Venereology and Allergology, Charité-Universitätsmedizin Berlin, Charitéplatz 1, DE-10117 Berlin, Germany. E-mail: georgios.kokolakis@charite.de
Adalimumab improves nail psoriasis and the quality of life of patients within 4 months. In this study of 267 patients, a long-term improvement in nail psoriasis maintained over 24 months of therapy was observed. Improvement in nail psoriasis and dermatological quality of life significantly correlate after one year of treatment. Younger patients and patients with a higher body mass index respond better to therapy.
Psoriatic nail symptoms are quite frequent among patients with psoriasis; their prevalence was estimated to be up to 50% (1). Exclusive impairment of the nail unit without cutaneous manifestations of psoriasis is, however, rare and occurs in 1–10% of patients with psoriasis (2). In patients with psoriatic arthritis, nail involvement is more frequent than in patients with plaque psoriasis, as high as 63% (3), and may correlate with more severe disease (4).
The clinical symptoms of nail psoriasis correspond to the involvement of different structures of the nail and can be divided into those in whom the nail matrix is affected and those in whom the nail bed is affected. Pits, transversal or longitudinal ridges, crumbling, leukonychia, as well as red spots in the lunula, are typical symptoms when the nail matrix is involved, and may result in onychorrhexis or complete onychodystrophy. Nail bed involvement is reflected by oil drop spots, subungual hyperkeratosis, onycholysis, and/or splinter haemorrhages (5).
Nail involvement causes psychological distress and feelings of embarrassment; therefore, patients have significant impairment in quality of life. Patients often try to hide their hands or feet (6). Furthermore, approximately half of the affected patients report pain and/or functional disability, resulting in frustration with daily activities in housekeeping or at work (7).
The treatment of nail psoriasis can be challenging, as therapies are often less effective for nail symptoms compared with skin lesions. Topical treatment is limited, since local antipsoriatic agents can only slowly, or sometimes not at all, penetrate the nail plate. Highly concentrated urea, emollients, corticosteroids (either topical or intralesional), calcipotriol, 5-fluorouracil, anthralin, and tazarotene, as well as psoralen plus ultraviolet A (PUVA) phototherapy or dye-pulsed laser, have been proposed as possibly effective local treatments for nail psoriasis, with variable outcomes (8, 9). Regarding systemic treatments, only sparse data are available regarding the efficacy of fumaric acid esters for the treatment of nail psoriasis (10). However, promising results in the treatment of psoriatic nail disease have been reported for methotrexate, acitretin, cyclosporine A, TNF-α blockers, ustekinumab, and, more recently, apremilast, ixekizumab, and secukinumab (11). This cohort study was planned to evaluate nail involvement in patients with plaque psoriasis and the influence of treatment with adalimumab based on real-world data.
Study population, procedures, and treatment regimen
A non-interventional prospective multicentre open-label cohort study was conducted to evaluate the efficacy of adalimumab, etanercept, or infliximab, either as monotherapy or combination therapy on nail psoriasis during 24 months of therapy in patients with moderate to severe plaque psoriasis with or without psoriatic arthritis. Since data with patients under infliximab, etanercept and combination therapies were very limited, only the cohort of patients receiving adalimumab monotherapy was evaluated.
The study population comprised adult patients with moderate to severe psoriasis, as defined by the “rule of ten” (Psoriasis Area and Severity Index (PASI) >10, Dermatological Life Quality Index (DLQI) > 10), who were candidates for systemic treatment with adalimumab according to licensure and had psoriasis of the fingernails. Exclusion criteria were: any other skin diseases that could interfere with the evaluation of psoriatic severity or forms of psoriasis other than plaque-type and the presence of latent or active tuberculosis, hepatitis B and C infection, and HIV infection. Patients who were unable to understand the questionnaires and adhere to the trial procedures were also excluded.
At baseline, adalimumab 80 mg was administered subcutaneously, followed by a dose of 40 mg at week 1 and then 40 mg in regular 2-week intervals over a period of 2 years. All participating patients provided written informed consent. The study was approved by the ethics committee of Charité-Universitätsmedizin Berlin (EA1/236/08) and was conducted according to the principles of the Declaration of Helsinki.
Efficacy assessments
The severity of psoriatic skin alterations was evaluated using PASI score (12) and body surface area (BSA). Nail involvement was estimated using the total Nail Psoriasis Severity Index (NAPSI) score for all fingernails, resulting in scores ranging from 0 to 80 (13). Efficacy assessments were performed at baseline, every 3 months for the first year and then twice annually for the second year of treatment. To minimize the deviation between the examiners, participating study centres were advised to keep the same investigator for each subject throughout the trial. To evaluate the impact of the disease in everyday life, the DLQI questionnaire was used at every scheduled visit (14).
The primary endpoint of the study was the percentage of patients with improvement in nail symptoms as defined by NAPSI75 response (75% improvement compared with baseline) after 12 months. The mean improvement in NAPSI and DLQI after 1-year of continuous treatment with adalimumab was determined as a secondary endpoint of the trial. Nail matrix and nail bed were assessed separately. Furthermore, the efficacy of treatment was also stratified by sex, age, and body mass index (BMI).
Safety
Adverse events, serious adverse events, and pregnancies, as well as abnormal values of routine laboratory parameters and vital signs, were documented throughout the trial. All adverse events, serious adverse events, and pregnancies that occurred during the trial should be reported to the authorities, as appropriate (Bundesinstitut für Arzneimittel und Medizinprodukte).
Statistical analysis
Statistical calculations were made using the Statistical Program for Social Sciences version 22 (IBM, Armonk, NY, USA) and Microsoft Excel 2013 (Microsoft Corporation, Redmond, WA, USA). The values available at each time-point were analysed as observed in a full analysis set without applying “last observation carried forward” method. The Kolmogorov–Smirnov test indicated the absence of normality in the distribution of the parameters. Differences between the non-paired samples of NAPSI improvement stratified according to age, BMI and sex were tested using the Mann–Whitney U test. Differences between the paired samples of NAPSI or DLQI improvement over the treatment period were analysed using the Wilcoxon matched-pairs signed-rank test. Differences between frequencies of men and women in NAPSI improvement groups, and NAPSI50 or NAPSI70 responders over the treatment period were tested using a χ2 test. The correlations between PASI, NAPSI, and DLQI were analysed using a two-tailed Spearman’s rank correlation test.
Study population
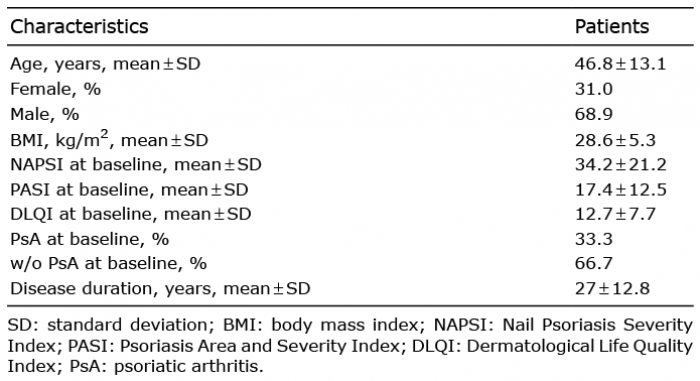
A total population of 267 patients (184 men; 83 women) with nail psoriasis with or without psoriatic arthritis (plaque psoriasis only, 178; psoriatic arthritis, 89) were included in this multicentre non-interventional prospective cohort trial. Patients had a mean ± standard deviation (SD) age of 47 ± 13.1 years, a BMI of 28.6 ± 5 kg/m2, PASI score of 17.4 ± 12.5 and a mean ± SD disease duration of 27 ± 12.8 years (Table I). Approximately 40% of the included patients reported a family history of psoriasis. All patients were recruited from outpatient departments in Germany.
No significant differences in the severity of nail psoriasis were observed between the groups with lower or higher age or BMI than the mean at baseline. However, male patients had more severe nail psoriasis than female patients (mean NAPSI score, 36.6 vs 29.0; p = 0.01).
Table I. Demographic and clinical characteristics of the study cohort (n = 267)
Efficacy of adalimumab on nail involvement
Overall improvement in NAPSI scores during treatment. The impact of adalimumab on nail psoriasis was estimated using the NAPSI, with total scores calculated in addition to nail matrix and nail bed scores. Within 3 months of initiating treatment with adalimumab, patients achieved a statistically significant NAPSI reduction ((32.8 ± 6.2% (mean% ± 95%confidence interval (CI)); p < 0.001), corresponding to a NAPSI score of 22.9 ± 2.3 (mean ± 95% CI), compared with baseline score 34.2 ± 2.5 (mean ± 95% CI) (Fig. 1). Approximately 34% and 17% of the patients achieved NAPSI50 or NAPSI75, respectively, after 3 months of treatment. Parallel improvements in both nail matrix and nail bed scores were observed (Fig. 2).
Fig. 1. Overall improvement in Nail Psoriasis Severity Index (NAPSI), NAPSI50 and NAPSI75 during adalimumab therapy. (a) Percentage reduction in NAPSI compared with baseline (mean ± 95% confidence interval (CI)); (b) p-values for NAPSI between time-points; and percentage of patients achieving (c) NAPSI50 and (d) NAPSI75 under therapy with adalimumab. nV0=267, nV3=240, nV6=225, nV9=190, nV12=187, nV18=157, nV24=143.
Fig. 2. Nail matrix and nail bed improvement trends during adalimumab therapy. Percentage reduction in (a) nail matrix and (b) nail bed Nail Psoriasis Severity Index scores (mean ± 95% CI). **p < 0.01; *** p < 0.001.
After 6 months, NAPSI was reduced by almost half, 16.2 ± 2.1 (mean ± 95% CI) compared with baseline. A statistically significant improvement between the time-points could be observed until one year after the initiation of the treatment. After a stabilization of nail disease until month 18 of continuous treatment, NAPSI further improved at month 24. At month 6 of treatment, 60% of the treated patients achieved NAPSI50, and 36.4% achieved NAPSI75. Nail bed involvement was dramatically reduced, to 42.2% of the initial score, whereas involvement of the nail matrix was reduced to approximately 55% of baseline values (Fig. 2). Nail bed involvement was further significantly reduced until 18 months after the initiation of treatment. After 1 year, approximately 79% of the patients achieved NAPSI50 and approximately 60% NAPSI75. A total NAPSI improvement of 68.6% was observed (11 ± 2.3 (mean ± 95% CI). NAPSI improvement significantly correlated with improvement in PASI (3.7 ± 1.0 (mean ± 95% CI; correlation coefficient, 0.495; p < 0.001). Interestingly, approximately 22%, 42%, and 60% of the patients achieved NAPSI90 after 6, 12, and 24 months of treatment, respectively. In general, nail symptoms continually improved in the first 12 months of treatment and improvement was maintained thorough the 24-month observation period (Fig. 3).
Fig. 3. Clinical outcomes of nail psoriasis in patients under treatment with adalimumab over 24 months. Baseline left (a, b) and right (c, d) hand with severe nail psoriasis. After 3 months of therapy, improvement is noted (e and f, left hand; g and h, right hand). Outcomes further improved after 12 months of treatment (I and j, left hand; k and l, right hand). After 24 months of treatment, no symptoms of nail psoriasis were visible (m and n, left hand; o and p, right hand).
Stratification of treatment response by sex, age, and BMI after 12 months
To determine the influence of demographic factors on the efficacy of adalimumab in nail psoriasis, patients were divided into 4 distinct groups according to improvement in nail psoriasis after 1 year of treatment compared with baseline: < 50%, 50% to 75%, 75–90%, and 90–100%. Sex, age and BMI were separately examined. In order to identify potential predictors for treatment response, the overall improvement in NAPSI stratified by sex, age, and BMI, and was further analysed in a post-hoc manner. Response to treatment did not differ significantly between the 2 sexes, although men had more severe nail disease at baseline. Interestingly, younger patients seemed to respond better to therapy. Overall, at month 12, patients younger than the mean age of the study population had a significantly higher reduction in NAPSI scores than patients > 47 years. The mean age of patients with a NAPSI response of 90–100% (mean age, 43.3 ± 1.5 standard error of the mean (SEM) years) was significantly lower compared with those with a < 50% NAPSI response (mean age 52.8 ± 2.2 SEM years) or a 50–75% NAPSI response (mean age 50.5 ± 2 SEM years; p < 0.05 for both). Surprisingly, patients with NAPSI improvement of 90–100% had significantly higher BMI compared with those with NAPSI response of 50–75% (29.1 ± 0.65 vs 26.8 ± 0.58; p < 0.05). However, the overall NAPSI score reduction did not differ significantly between patients with BMIs lower and higher than the mean values (Fig. 4).
Fig. 4. Stratification of Nail Psoriasis Severity Index (NAPSI) improvement at month 12. Stratification by: (a) sex, (b) age, and (c) body mass index (BMI) of patients achieving an improvement in NAPSI score < 50%; 50–75%, 75–90%, and 90–100% (mean ± SEM). *p < 0.05.
Impact of adalimumab on patient quality of life
A rapid reduction in DLQI scores was achieved, with a significant improvement (47.5%) compared with baseline (p < 0.001), which was apparent within the first 3 months of therapy. After 6 months of treatment, DLQI further improved, to approximately 40% of the initial visit and was maintained over the observation period. At visit 12, the percentage reduction in DLQI compared with baseline correlated significantly with the improvement in NAPSI (correlation coefficient, 0.343; p < 0.001; Fig. 5).
Fig. 5. Dermatology Life Quality Index (DLQI) reduction during adalimumab treatment and correlation with Nail Psoriasis Severity Index (NAPSI) improvement at month 12. (a) Percentage improvement in DLQI scores compared with baseline (mean ± 95% confidence interval (CI)) and (b) correlation of NAPSI improvement with DLQI improvement after one year of treatment.
A variety of local and systemic options to treat plaque-type psoriasis is currently available, with well-established strategies, including a wide range of therapeutics (15, 16). However, for the treatment of special subtypes of psoriasis, such as nail psoriasis, the lack of data, as well as restricted therapeutic options, can make treatment quite challenging. In this study, the efficacy of adalimumab was evaluated in a population of 267 patients with psoriatic nail disease. All fingernails, not just isolated target nails, were assessed for the duration of the trial.
Conventional systemic therapies have been shown to be efficacious in the treatment of nail psoriasis. In a recently published single-blind randomized trial, methotrexate, at a starting dose of 15 mg/week, was significantly superior to treatment with cyclosporine A, and patients achieved a 43.3% reduction in NAPSI scores after 6 months of treatment compared with 37.2% in the cyclosporine treatment arm (17). However, Reich et al. reported a 36.8% reduction in NAPSI scores after 6 months of treatment with methotrexate 5–25 mg/week (18). Acitretin administered at a dose of 0.2–0.3 mg/kg body weight for 6 months led to a NAPSI reduction of approximately 41% (19). In the case of fumaric acid esters, verified data from trials are unavailable, and the evidence of their efficacy in the treatment of nail psoriasis is based solely on case reports (10). Patients treated with apremilast, the first oral phosphodiesterase 4 inhibitor approved for the treatment of plaque psoriasis, had an improvement of 22.5% in NAPSI response after 16 weeks of treatment (20). NAPSI50 was achieved in 44.6% of patients with apremilast 30 mg twice a day vs 18.7% in the placebo group at week 16 (21).
The introduction of biologics expanded the possibilities for treatment of nail psoriasis. Published data already indicate that adalimumab is effective for the treatment of nail psoriasis. In a subanalysis of the BELIEVE study, the median decrease in NAPSI score was 15.1% and 39.5% at week 8 and 16 compared with baseline scores, respectively (22). A phase 3 randomized placebo-controlled trial especially designed to evaluate the efficacy of adalimumab in nail psoriasis was published during the preparation of this manuscript. At week 16, 20.6% of patients achieved a NAPSI75 response; 26 weeks after the initiation of adalimumab, a NAPSI75 response was achieved in 46.6% of patients (23).
As expected from already published data and clinical experience, in this study, treatment with adalimumab resulted in a rapid improvement in nail psoriasis within 3 months of the initiation of therapy, reaching a reduction of about 55% after 24 weeks. Nail psoriasis continuously improved over 9 and 12 months of treatment. The improvement in symptoms was sustained over 2 years of continuous treatment, during the observation period of the trial. The study population represents real-world patients and was larger than in the phase 3 trial. No differences in terms of age, sex or BMI and severity of nail psoriasis were observed at baseline. Both sexes responded equally after one year of therapy. However, younger patients achieved a more pronounced improvement in nail psoriasis. That could be explained either by the faster growth of nails in younger patients or by the fact that they might have experienced less previous therapies before adalimumab. This finding emphasizes the importance of an earlier initiation of therapy with adalimumab in patients with nail psoriasis. Interestingly, patients with a higher BMI responded better to treatment; even though younger patients were neither obese nor overweight.
In parallel with nail symptoms, the quality of life of patients rapidly improved within the first 3 months of treatment and persisted for the entire duration of the trial. After one year of continuous treatment, improvement in DLQI scores correlated significantly with NAPSI improvement, indicating the impact of nail psoriasis on the quality of life of patients. Interestingly, improvement in PASI also correlated with NAPSI improvement, showing a parallel remission of skin and nail disease after treatment with adalimumab.
Taking into consideration the observed efficacy, as well as the safety profile and the uncomplicated application of the drug, adalimumab appears to be a promising long-term therapeutic option for nail psoriasis. Younger and overweight patients, both high-need groups because of family planning, professional circumstances or metabolic comorbidity, respond better to adalimumab.
The authors would like to thank Susanne Weste for her support in organizing and conducting this trial. The design, study conduct, and financial support for the study were provided by AbbVie. AbbVie participated in the interpretation of data, review, and approval of the publication.
Conflicts of interest: GK has received travel grants or honoraria, or has been a consultant member of advisory boards and speakers bureaus for one or more of the following: AbbVie Deutschland GmbH & Co. KG, Actelion Pharmaceuticals Ltd, Basilea Pharmaceutica Ltd, Biogen Idec GmbH, Celgene GmbH, Janssen-Cilag GmbH, Leo Pharma GmbH, Lilly Deutschland GmbH, MSD Sharp & Dohme GmbH, Novartis Pharma GmbH, Pfizer Deutschland GmbH, and UCB Pharma GmbH. FB has received travel grants or honoraria from 1 or more of the following: AbbVie Deutschland GmbH & Co. KG, Biogen Idec GmbH, Celgene GmbH, Galderma GmbH, Janssen-Cilag GmbH, Leo Pharma GmbH, MSD Sharp & Dohme GmbH, Novartis Pharma GmbH, Pfizer Deutschland GmbH. KW has received research grants, travel grants, consulting honoraria or lecturer’s honoraria from AbbVie Deutschland GmbH & Co. KG, Bayer Schering Pharma AG, Biogen IDEC GmbH, Celgene GmbH, Dr Willmar Schwabe GmbH & Co. KG, Flexopharm GmbH & Co. KG, Generon Corporation Ltd, JanssenCilag GmbH, Johnson & Johnson Pharmaceutical Services, Novartis Pharma GmbH, Pfizer Deutschland GmbH, Sanofi-Aventis Deutschland GmbH, FS Trial Form Support GmbH, and UCB Pharma GmbH. RS has received research grants or honoraria for participation in advisory boards, clinical trials, or as speaker for 1 or more of the following: AbbVie Inc., AbbVie Deutschland GmbH & Co. KG, Bayer Schering Pharma AG, Biogen Idec GmbH, Boehringer Ingelheim Pharma GmbH & Co. KG, Celgene GmbH, Celgene International II Sàrl, Charité Research Organisation GmbH, Dr Willmar Schwabe GmbH & Co. KG, Flexopharm GmbH & Co. KG, Generon Corporation Ltd, JanssenCilag GmbH, Novartis Pharma GmbH, Parexel International GmbH, Pfizer Deutschland GmbH, Sanofi–Aventis Deutschland GmbH, TFS GmbH, and UCB Biopharma SPRL. SP has received travel grants or honoraria, or has been a consultant member of advisory boards and speakers bureaus for one or more of the following: AbbVie Deutschland GmbH & Co. KG, Almirall Hermal GmbH, Amgen GmbH, Biogen Idec GmbH, BMS GmbH, Boehringer Ingelheim Pharma GmbH & Co. KG, Celgene GmbH, Charité Research Organisation GmbH, Dermira, Inc, Forward Pharma, GlaxoSmithKline GmbH & Co. KG., Janssen-Cilag GmbH, Leo Pharma GmbH, Lilly Deutschland GmbH, Maruho Europe Ltd, MSD Sharp & Dohme GmbH, Mundipharma, Novartis Pharma GmbH, Pfizer Deutschland GmbH, Sandoz Pharmaceuticals GmbH, VBL Therapeutics, and UCB Pharma.


 Click to show fullsize
Click to show fullsize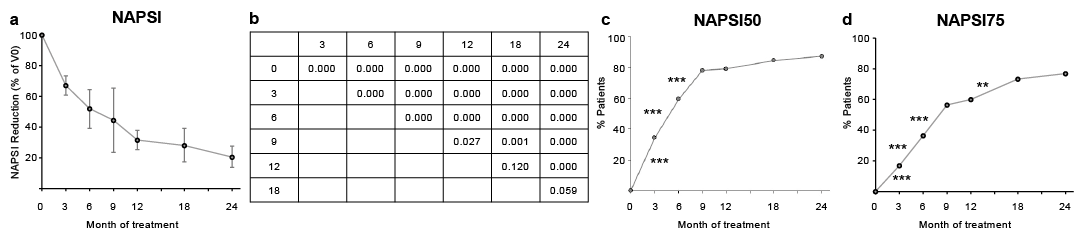 Click to show fullsize
Click to show fullsize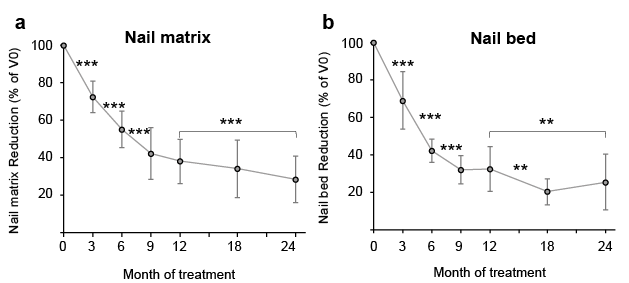 Click to show fullsize
Click to show fullsize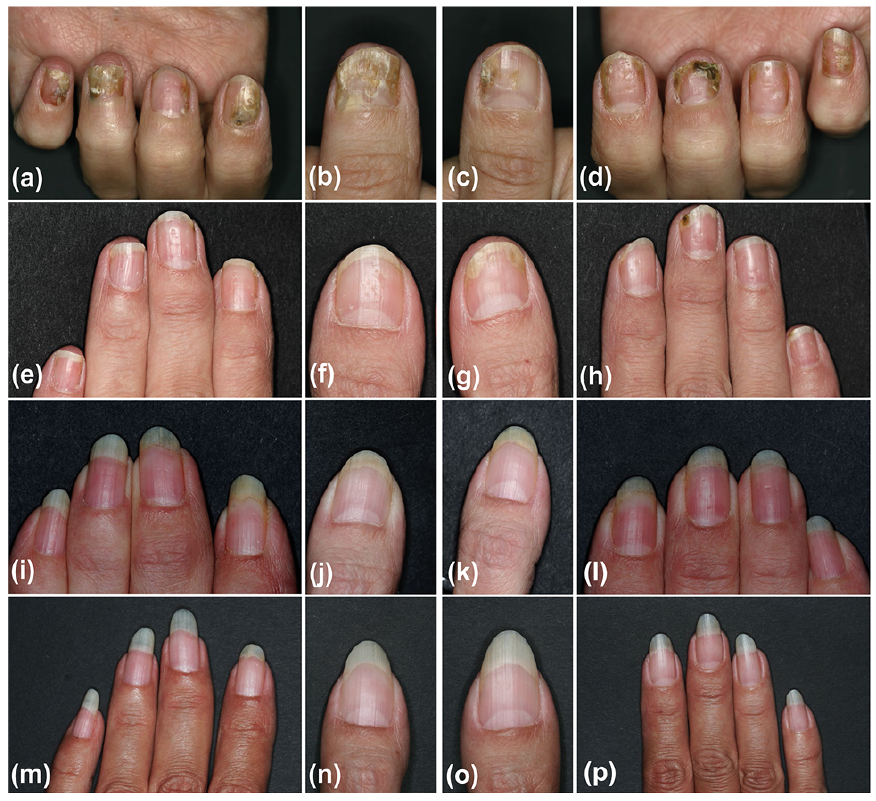 Click to show fullsize
Click to show fullsize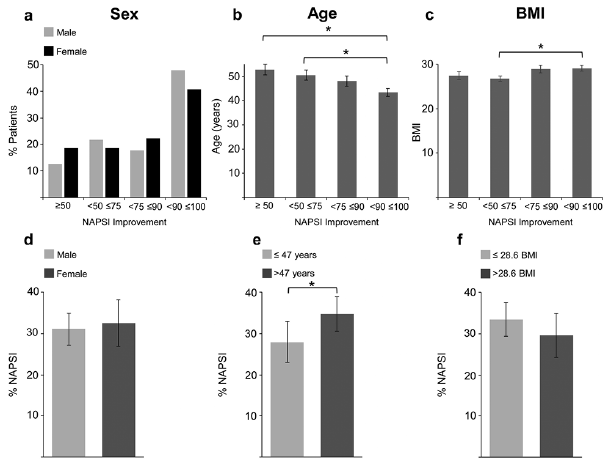 Click to show fullsize
Click to show fullsize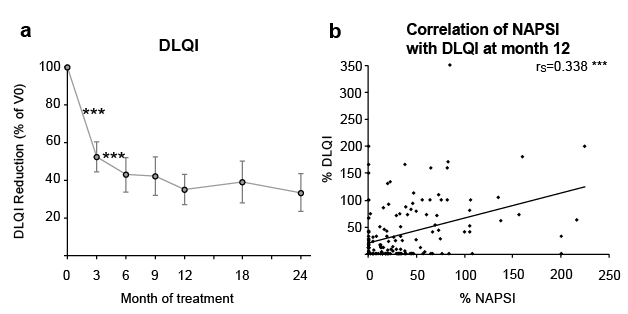 Click to show fullsize
Click to show fullsize