


1Department of Dermatology-Venereology and 2Department of Onco-Dermatology, Hôpital Robert-Debré, avenue du Général Koenig, FR-51100 Reims, and 3Department of Pathology, Hôpital Maison-Blanche, Reims, France. E-mail: eml.dz@live.fr
Accepted May 28, 2020; Epub ahead of print Jun 8, 2020
Acta Derm Venereol 2020; 100: adv00202
Diffuse dermal angiomatosis (DDA) is a rare variant of cutaneous reactive angiomatosis characterized by proliferation of endothelial cells in the reticular dermis (1). Most often unifocal or involving both breasts (2), it can also affect the lower limbs, abdomen and buttocks. We describe here a case of multifocal DDA in a woman with multiple cardiovascular risk factors.
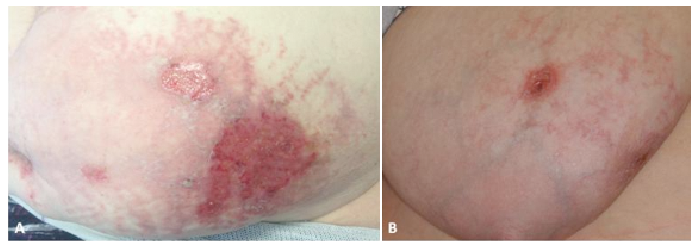
Ten months after surgery for an abdominal hernia, superficial pustular and ulcerous abdominal lesions with telangiectatic borders developed in a 61-year-old obese woman (body mass index 44.1 kg/m2) (Fig. 1A). The patient had a history of dyslipidaemia, high blood pressure, chronic renal failure, chronic arterial occlusive disease of the lower extremities treated by angioplasty of the right femoral artery, and current smoking. She was receiving platelet anti-aggregants and an angiotensin-converting-enzyme inhibitor, but no statins (because of myalgia during treatment). Biopsy of the border of an ulceration showed an epidermis of normal morphology surmounted by a thin layer of orthokeratosis, adjacent ulcerations extending into the superficial dermis, lined with fibrino-leukocyte coatings; the base of the ulcer was fibrous and had many capillary neovessels and a few clumps of lymphocytes. The dermis and hypodermis were normal. Acute or specific inflammation was not observed.
Fig. 1. (A) Erosive, pustular, livedoid lesions of the abdomen and (B) ulcerated lesion with livedoid and telangiectatic lesions of the right breast in a 61-year-old obese woman (body mass index 44.1 kg/m2).
Despite the lack of pathological evidence, at this time, the clinical diagnosis favoured a superficial pyoderma gangrenosum, which was effectively treated with topical propionate clobetasol 0.05%. Two years later, painful telangiectatic and livedoid lesions developed on the right breast, with superficial ulcerations and atrophic scars (Fig. 1B). Three months later, the patient also presented telangiectasia on the left breast. Blood test results were normal, with normal blood count, coagulation, and protein S and C levels, and a negative search for anti-nuclear, anti-DNA, anti-phospholipids, anti-neutrophil cytoplasmic antibodies; cryoglobulinaemia; and HIV and hepatitis B and C virus infection. The patient showed moderate hyperhomocysteinaemia (homocysteine level 22.8 µmol/l (range 5–20 µmol/l)). Histology of the lesion on the right breast revealed a dermal proliferation of endothelial cells between collagen bundles (Fig. 2A), with some telangiectasia. The cells were not atypical and were stained with CD31 (Fig. 2B), but not CD34. Ki 67 level was not increased. The features were consistent with DDA.
Initial management consisted of advice regarding weight reduction, adequate blood pressure control, and smoking cessation and the introduction of rosuvastatin, 5 mg/day, which was well tolerated after a month of treatment. The patient also received isotretinoin, 10 mg/day, for one month, which was inefficient and not well tolerated (mood disorder) and was stopped by the patient. At one-year follow-up, the patient had reduced her smoking consumption, but she had not lost weight, and lesions on the breasts were unchanged.
Fig. 2. (A) Histology showing a proliferation of endothelial cells in the dermis between collagen bundles. (B) CD31 staining on immunohistochemistry. Magnification ×20.
DDA was first described by Krell et al. in 1994 (1). It is a rare, acquired, benign variant of cutaneous reactive angiomatosis, characterized by an extravascular proliferation of endothelial cells, manifested by erythematosus or purpuric or livedoid patchy lesions evolving into dry necrosis or superficial ulcerations (2). The typical localizations are breasts, abdomen, lower extremities, and the arms, buttocks and trunk (3). We describe here an obese woman in whom patchy telangiectatic, livedoid and erosive lesions developed on the abdominal wall secondary to a local surgery and who presented, several months later, painful breast involvement, with features consistent with DDA.
Touloei et al. recently reviewed 73 cases published in the literature (3). DDA seemed to occur mostly in females with large pendulous breasts. Most patients had an underlying severe vascular disease, were overweight, and had high blood pressure and a history of smoking.
Differential clinical diagnoses are pyoderma gangrenosum, Degos disease, cutaneous reactive angiomatosis, Kaposi sarcoma, and pathomimia, as well as calciphylaxis. Of note, cases of associated calciphylaxis (3, 5) occurred in patients with high cardiovascular risk associated with chronic renal failure and dialysis.
Histologically, DDA is characterized by dermal proliferation of endothelial cells between collagen bundles that expresses CD31 and CD34 (1) and sometimes forming small vascular lumina. Unlike cutaneous reactive angiomatosis, DDA does not feature an intravascular proliferation of endothelial cells that can occlude the vascular lumina. The pathological differential diagnoses include acroangiodermatitis, Kaposi sarcoma and well-differentiated angiosarcoma.
After excluding cases with explicit unifocal involvement, involvement of both breasts, or un-reported location, 13 cases were found in the literature of DDA with multifocal involvement (1, 4–14), as in our case (Table SI). Among them, 84.6% involved women, with mean age 58 years; 46.2% involved current smokers; and 46.2% featured atherosclerosis, as expected according to the review of Touloei et al. (3) The thigh was the most common location, observed in 61.5% of cases. A secondary involvement on another place after healing in the first place, as observed in the current case, was not reported, with multifocal involvement occurring during the same time. Revascularization was effective in 5 patients with arterial stenosis or occlusion in the same location as DDA.
The pathophysiology of DDA is still not completely understood. An initial ischaemic event favoured by local trauma could lead to inflammation and endothelial proliferation because of the production of vascular endothelial growth factor (2, 5, 9). This hypothesis is supported by 5 cases of haemodialysis-related arteriovenous fistula with DDA occurring on the same upper extremities (3), a case of prior breast reduction in the same location as DDA (4), and by the current case, after surgery of the abdominal wall. An ischaemic mechanism is also supported by some patients with an underlying arterial occlusion or tight artery stenosis of the leg or thigh and DDA in the same location (1, 4, 7, 8, 10, 13, 14).
The treatment of DDA is not well codified and relies mainly on managing atherosclerosis risk factors. Smoking cessation led to complete resolution of DDA in 2 cases (3). With breast involvement, isotretinoin has been proposed because of its anti-angiogenic role, with good efficiency (3), as well as pentoxifylline and oral corticosteroids (3). Breast reduction surgery may also be considered, with good results (15). In our case, the first episode in the abdomen was effectively treated with topical propionate clobetasol 0.05%, which was reported as partially effective. According to the literature data, topical corticosteroids did not show to be an effective option for the treatment of DDA, explaining why we did not prescribe them despite the fact that the abdominal lesions had previously developed favourably with topical corticosteroids. The efficacy of revascularization of the involved area (1, 3, 4, 7, 10, 14) has been reported and seems to be the most efficient treatment with extremities involvement.
DDA should be better known by dermatologists and discussed in the setting of telangiectatic lesions with superficial ulcerations, occurring on an atheromatous site or on breasts. Cardiovascular diseases must be investigated in these patients. Multifocal lesions are possible. The correction of the favouring factors, including cardiovascular risks, is essential in the treatment of this condition.
The authors thank Laura Smales (BioMedEditing) for providing writing assistance in English.
Conflicts of interest: MV has been an investigator, a board member or has received fees from Amgen, Boehringer, Novartis, Leo Pharma, Lilly, Arrow, Abbvie, Janssen, MSD, Pfizer, and Medac.


 Click to show fullsize
Click to show fullsize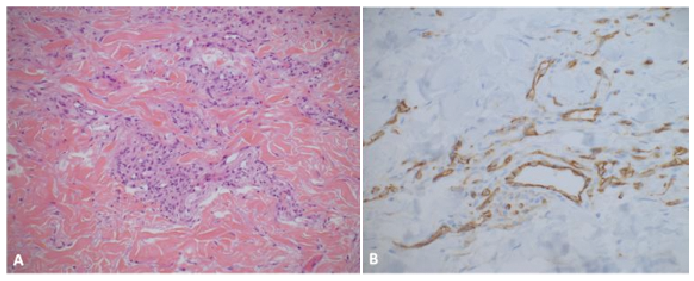 Click to show fullsize
Click to show fullsize