


1Department of Dermatology und Venereology, 2Department of Psychiatry and Psychotherapeutic Medicine, Medical University Graz, Graz, 3Center for Integrative Addiction Research (CIAR), Grüner Kreis Society, 4Department of Religious Studies, University of Vienna, Vienna, Austria
Shame has been registered as a part of psychosocial distress in patients with psoriasis. This study investigated 44 patients with psoriasis and 88 age- and sex-matched individuals without skin disease. Skin shame, multifarious expressions of shame, psychological symptoms, overall health, dermatological quality of life, disease burden and disease severity were measured. Higher levels of skin shame correlated with a greater disease burden (r=0.63; p < 0.01), higher Dermatology Life Quality Index (r=0.33; p < 0.05), and lower mental quality of life (r=–0.30; p < 0.05). Patients had a higher level of skin shame (F=74.03; eta2= 0.36; p < 0.01) and less physical quality of life on the SF-36 (F=5.14; eta2= 0.04; p < 0.05) than non-dermatological controls. General shame was not related to disease burden or quality of life. While self-rated skin shame appears to be related to quality of life in patients with psoriasis, no association was registered between expert-rated Psoriasis Area and Severity Index and quality of life.
Key words: psoriasis; skin shame; SHAME; quality of life; disease burden; Psoriasis Area and Severity Index.
Accepted Jun 10, 2020; Epub ahead of print Jun 12, 2020
Acta Derm Venereol 2020; 100: adv00205.
Corr: Elisabeth Aberer, Department of Dermatology und Venereology, Medical University Graz, Auenbrugger Platz 8, AT-8036 Graz, Austria. E-mail: eaberer@gmx.at
Shame is a negative emotion that has been shown to cause psychosocial distress in patients with psoriasis. This study used questionnaires to measure skin and general shame. The results show that higher levels of skin shame were associated with greater disease burden and impaired quality of life. Interestingly, skin shame was correlated with severity of psychiatric disease burden in a similar way to in controls without skin disease. Similarly, general shame and psychiatric disease burden did not differ between patients and controls. It was notable that skin shame did not correlate with Psoriasis Area and Severity Index, the measured disease severity index.
Recently, the Global Burden of Diseases Study showed that skin diseases were the fourth leading cause of non-fatal disease burden (1). At least one-third of dermatological patients are impaired by their disease and experience psychological distress, which influences their personal lives as well as their environment, relationships, and professional lives (2–4).
One of the major triggers of psychological distress is the feeling of shame. Shame is associated with a wide range of psychological symptoms, such as anxiety, loss of self-confidence, lowered self-esteem, anger, and frustration (5–7). In the past, the disease-induced level of shame, the extent of embarrassment felt, and the appraisal due to skin disease have been investigated in patients with psoriasis (6–11). In a study conducted by Rzepa et al. (6), half of patients with psoriasis assigned shame to their disease. In comparison, shame played a role in 75% of patients with syphilis and 30% of those with acne.
Psoriasis is a chronic inflammatory skin disease that affects 1–3% of the general world-wide population (9). Psoriasis occurs on different parts of the body, including visible areas of the skin, such as the face, scalp, hands, and nails. The lesions shed scales onto the patients’ clothes, which may give rise to avoidance strategies with regard to social contact (8, 12, 13). The condition is frequently feared in the social environment and mistaken for a contagious disease (7).
A number of previous studies addressing the connection between clinical variables, disease severity and quality of life (QoL) in psoriasis have revealed a poor correlation between Psoriasis Area and Severity Index (PASI) score and overall QoL, such as Dermatology Life Quality Index (DLQI) and psychological distress indexes (14–17). In a multicentre study, psoriasis was described as the disease with the highest psychological burden compared with atopic dermatitis, hand eczema, and leg ulcers. Ten percent of patients with psoriasis are depressed (18); higher depression levels are significantly associated with a higher rate of suicidal ideation (19). Based on the Touch-Shame-Disgust-Questionnaire, Lahousen et al. (9) reported that skin-related disgust and shame were significantly higher in patients with psoriasis than in healthy controls. The patients scored significantly lower than healthy controls with regard to their appraisal of self-touching and parental touching (9, 20).
Feelings of shame have not been given sufficient attention in the past, and controlled studies concerning shame in dermatology do not exist. Recently, we tested adult patients with common skin diseases and a control group without skin disease using the Skin Shame Scale (SSS-24), whose German version has been validated using the SHAME questionnaire (5) and the Brief Symptom Inventory-18 (BSI-18) (21, 22). In further studies, patients with a variety of dermatological diseases were investigated with regard to several variables of shame using the 2 above-mentioned shame questionnaires. In a recently published article by Aberer et al., patients with psoriasis, besides those with inflammatory diseases and eczema, had the highest scores for skin shame, as revealed by the SSS-24 questionnaire (23).
The aim of the present study was to investigate patients with psoriasis, determine the association between skin shame, general shame, and disease activity measured by the PASI, disease burden, and the self-rated DLQI. The second aim was to correlate psychological distress (BSI_GSI) and QoL with levels of skin and general shame in patients with psoriasis. A further aim was to determine differences between dermatological patients and non-dermatological controls with regard to the measured scores.
Study design and participants
This prospective, single-centre, observational study investigated 44 patients with psoriasis from the outpatient clinic at the department of dermatology and venerology, Medical University of Graz, between March and June 2018. The study was approved by the ethics committee of the Medical University of Graz, Austria (30-241 ex 17/18). Patients were asked to complete the questionnaires in the waiting area in order to ensure that their participation did not take additional time.
Written informed consent was obtained and the patients had to be at least 18 years of age. Those who had difficulty understanding German were excluded. Socio-demographic data with regard to age, sex, education, family status, and the subjective burden of disease (measured on a 10-point scale) were obtained by asking all study participants to complete a demographic questionnaire. Disease-related data, including the type of psoriasis (plaque, guttate, inverse, or pustular), psoriatic arthritis, nail psoriasis, DLQI and the PASI (range 0–72; mild (< 10), moderate (10–50), and severe (> 50)) were obtained from the medical records in the MEDOCS database at the University Clinic of Graz.
As controls (CO) (n = 88), we used the data of 488 individuals (of 597 participants eligible for analysis) without skin disease, who were recruited via an online survey at the Medical University Graz, or were hospital residents or related persons (22), who had undergone a recent investigation. The non-dermatological controls were age- and sex-matched with psoriatic patients. The only difference between controls and dermatological patients (DP) was the higher education level of the former.
Psychometric measures
Skin Shame Scale (SSS-24). Based on models of shame in the context of dermatological disease and body awareness, this questionnaire reflects individual skin-related shame. This psychodermatological assessment scale comprises 24 items (such as “I’ve learnt to live with my skin condition”), which have to be answered on a 5-point scale ranging from 1 to 5. The questionnaire has been translated into German and validated, among other means, through correlations with measures of shame and psychological distress. Cronbach’s alpha was 0.95 for dermatological patients (22, 24).
SHAME (SHame Assessment scale for Multifarious Expressions of shame). This questionnaire measures 21 items on 3 subscales, including bodily shame (such as “I buy underwear. When I have just made up my mind, I discover two of my acquaintances who have watched me select.”) and cognitive shame (such as “I am praised for something that I have not achieved myself.”) as adaptive, and existential shame (such as “A friend comes to visit me and brings me the latest CD from my favourite band.”) as pathological-dysfunctional shame. The respondents rated their answers on a scale from 0 to 5 points for each of the 3 subscales, and the scores were summarized. The questionnaire was validated through correlations with measures of psychological distress. Cronbach’s alpha was between 0.76 and 0.86 (5).
Medical Outcomes Study 36-Item Short Form Health Survey (SF-36). QoL was measured by the Medical Outcomes Study 36-Item Short Form Health Survey (SF-36). As an example, 1 item is “In general, would you say your health is…”, with answers ranging from “excellent” to “poor”. The following 8 areas are covered by the SF-36 questionnaire: physical function, physical role, bodily pain, general health, vitality, social function, emotional role, and mental health. For each scale, the score ranges from 0 (poor) to 100 (excellent). The 8 sub-dimensions may be summarized into 2 standardized global scores, i.e. the Physical Component Score (PCS) and the Mental Component Score (MCS) of QoL. SF-36 has been validated in several studies, Cronbach’s alpha was > 0.90 (25, 26).
Dermatology Life Quality Index. The DLQI is a simple validated questionnaire consisting of 10 questions, which measure how much the respondent’s skin problems have affected his/her life over the last week on 4-point Likert scales. The DLQI (range 0–30) comprises items, such as symptoms and feelings, daily activity, leisure, work/school, personal relationships, and side-effects of treatment. One of the items is “Over the last week, how embarrassed or self-conscious have you been because of your skin?”, with answers ranging from “not at all” to “very much”. The reliability of the questionnaire was determined by Spearman’s rank correlation coefficient. The correlation between the overall DLQI scores was very high (γs = 0.99; p < 0.0001). The test-retest reliability of the individual question scores was also high (γs = 0.95–0.98; p < 0.001) (27).
Brief Symptom Inventory-18 (BSI-18). The BSI-18 is a short version of the well-established Symptom Checklist SCL-90-R. The degree of psychiatric burden during the preceding 7 days for 3 dimensions of psychiatric symptoms – somatization (e.g. Difficulty breathing), depression (e.g. Feelings of loneliness), and anxiety (e.g. Nervousness or inner tremor) – is assessed by 18 items (6 items for each sub-scale). The BSI-18 employs a 5-point rating scale ranging from 1 to 5. The 18 items can also be summarized into the Global Severity Index (GSI) of psychiatric symptoms. Correlations with measures of similar dimensions indicate a good convergent validity; criterion-related validity was also established. Cronbach’s alpha was between 0.63 and 0.93 (21).
Statistical methods
Case-control matching was used to generate a suitable control sample. Given the small number of cases, a 1:2 case-control ratio was used to maximize the statistical power of the study. Controls were matched according to sex and age (3-year age bands). Analysis of variance (ANOVA) and χ2 tests were performed for group comparison. Pearson’s correlation was used to investigate the relationship between the study variables. In consideration of the sample size and the exploratory nature of the study, the α-value was set to p < 0.05. A description and interpretation of effect sizes were included for a better evaluation of the results.
Demographics
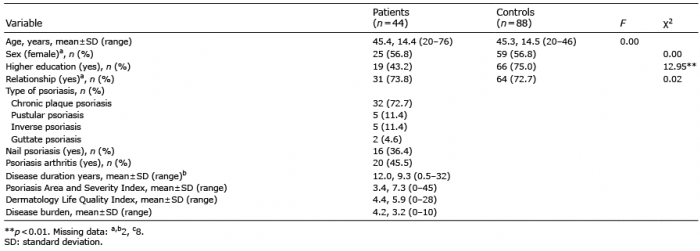
The data of 44 patients with psoriasis (mean ± standard deviation (SD) age 45.41 ± 14.42 years, 25 women (56.8%)) were analysed as seen in Table I. The mean ± SD duration of disease was 12.01 ± 9.33 years (range 0.5–32 years). Nineteen patients (43.2%) had a higher education (high school or university), and 31 (73.8%) were living with a partner. The majority of patients (n = 32) had chronic plaque psoriasis, followed by pustular psoriasis (n = 5), inverse psoriasis (n = 5) and guttate psoriasis (n = 2). Nail psoriasis was observed in 16 patients and psoriatic arthritis in 20. The mean ± SD score on the PASI was 3.39 ± 7.27, the mean ± SD score on the DLQI 4.41 ± 5.92, and the mean ± SD score for disease burden 4.19 ± 3.24.
Table I. Demographics in patients and controls
Controls consisted of 88 age- and sex-matched individuals without skin disease. The mean ± SD age of controls was 45.28 ± 14.49 years, 50 of them were women (56.8%), 72.7% lived in a relationship, and 75% had a high level of education. The education level of controls was significantly higher than that of patients (p < 0.01) (Table I).
Correlations between psychometric variables
Skin shame was correlated with disease burden (r = 0.63; p < 0.01), DLQI (r = 0.33; p < 0.05), and the mental component score of the SF-36 (r = –0.30; p < 0.05) in dermatological patients. No correlations were registered between PASI and other psychometric variables. The DLQI revealed a significant association with the Global Severity Index of the BSI (r = 0.34; p < 0.05), as well with a lower mental component score on the SF-36 (r = –0.33; p < 0.05) (Table II). The SHAME subscales of body and cognitive shame correlated with the depression score of the BSI (r = 0.35; r = 0.31; p < 0.05; data not shown in the tables).
Correlations between psychometric variables were quite different in controls. In contrast to patients with psoriasis, the mean summary score of skin shame in controls correlated with the GSI of BSI (r = 0.28; p < 0.01) as well as with an impaired physical component score on the SF-36 (r = –0.21; p < 0.05). SHAME correlated with an impaired mental health (r = –0.39, p < 0.01) in controls (data not shown in tables).
Table II. Correlations between psychometric variables in patients shown by r-values
Mean differences in psychometric variables between patients and controls
No significant differences were noted in the skin shame scores of patients with additional nail psoriasis (66.63 ± 13.96 vs 63.89 ± 19.81) or psoriatic arthritis (66.90 ± 17.12 vs 63.21 ± 18.51); data not shown in the tables). Patients with psoriasis had a higher SSS-24 score (64.89 ± 17.78 vs 43.39 ± 10.83; p < 0.01), but a lower SF-36 physical component score (47.69 ± 8.70) than non-dermatological controls (51.28 ± 7.58; p < 0.05). The SHAME subscales and BSI-subscales did not differ between patients with psoriasis and controls (Table III).
Table III. Psychometric variables in patients and controls
The present study found that skin shame is a major concern for patients with psoriasis because of its strong association with disease burden and QoL. Notably, skin shame and the investigated subscales of general shame, bodily and cognitive and existential shame did not correlate with disease activity on the PASI.
Patients with skin diseases that alter their appearance are liable to experience social anxiety, stigma, shame, impaired self-esteem and QoL (24). Dalgard et al. (19) highlighted the clinical implications of disease burden, especially with regard to psoriasis. Their observational cross-sectional study assessing depression and anxiety by the HADS showed that, of all dermatological conditions, only psoriasis was significantly associated with suicidal ideation; psoriasis was also associated with the highest burden of depression and anxiety. Disease burden summarizes all factors contributing to morbidity in patients, such as physical conditions, mental health, anxiety, depressive disorders, or psychological impairment (4, 12). In the present study, disease burden was measured on a self-rated score that did not correlate with any subscale of the BSI. Therefore, we assumed that skin shame is an aspect of QoL, and especially of mental health.
In contrast to QoL variables, skin shame did not correlate with the mean global severity index of the BSI, although feelings of stigma, embarrassment, and shame are known to be precursors of depression. Gupta et al. (28) examined the experience of stigma among 137 patients with moderate to severe psoriasis. The authors reported that the clinical severity of disease had no impact on whether the patients felt stigmatized. However, higher depression scores were seen in the stigmatized group (28). In our study, patients with general shame may have been stigmatized, as shown by the fact that cognitive and bodily shame, 2 subscales of SHAME, were correlated with the depression score of the BSI. A number of previous studies investigating the association between clinical variables, disease severity, and QoL in psoriasis have revealed a poor correlation between the PASI score and overall QoL, such as DLQI and psychological distress indexes (14, 15). In a systematic review of the published literature, Kimball et al. (29) suggest that the impact of psoriasis on QoL and psychosocial comorbidities is not always proportional to, or predicted by, measurements of disease severity, such as scores on the body surface area index or the PASI. In accordance with previous reports, we observed that the DLQI, including physical and mental health, is most likely independent of the PASI administered by the physician, and that skin disease may have a notable impact on the patients’ QoL even when limited skin areas are involved (29, 30). In view of the fact that the majority of our patients were already undergoing specific systemic treatment, the mean PASI of 3.39, which was an expression of the clinical severity of disease, was rather low. This might be one reason for the absence of a correlation between skin shame scores and the PASI.
In contrast to controls, the SHAME summary score of patients did not correlate with skin shame. The SHAME questionnaire includes bodily, cognitive, and existential shame (5). Bodily shame was not higher in psoriasis patients than in controls, which may suggest that bodily shame affecting the ideal body image, intimacy and sexuality is not impaired by skin lesions.
As expected, skin shame was more pronounced in patients than in controls without skin disease, but the general experience of shame was not higher in patients with psoriasis than in controls. However, the physical health of patients with psoriasis was significantly impaired compared with that of controls.
The fact that all investigated parameters correlated with skin shame in age- and sex-matched controls without dermatological disease raised certain questions. We used twice as many controls, whose demographics differed only in terms of their educational status. Socioeconomic studies showed that shame and anger are associated with a low level of education (7). In fact, patients with psoriasis were less educated, which might be a limitation of the study, and their skin shame was higher than that of controls. We do not attribute this higher level of skin shame to the patients’ educational level, but to the disease itself. In a previous study by Aberer et al. (23), dermatological patients generally had a higher level of skin shame; the level was highest in patients with psoriasis. The physical appearance of psoriasis also causes a substantial social burden for patients (31). One significant aspect of this burden is the experience of stigmatization, which was reported by 73% of patients and correlated, among other predictor variables, with a lower level of education, greater visibility of disease, as well as the severity and duration of disease (31).
A limitation of the current study is the self-reported questionnaire measurement of disease burden. In the absence of a disease burden questionnaire for skin disease in the German language, we used the SF-36 and DLQI. These are 2 standardized instruments that objectively measure different aspects of limitations in Qol, which may be summarized as disease burden.
The prime limitation of this pilot study is the relatively small number of patients with psoriasis. Therefore, group differences in the manifestations of psoriasis (such as arthritis or nail psoriasis) related to the SSS-24 could not be analysed separately. In fact, approximately 15–25% psoriatic patients have concomitant skin and joint symptoms and 8.5% of patients with psoriasis have psoriatic arthritis, which is associated with a higher psychosocial burden and reduced QoL (32, 33). We were unable to evaluate the specific influence of psoriasis with manifest arthritis on QoL or depression, because our sample size was too small for a reliable statistical analysis. Furthermore, we did not address other comorbidities, such as cardiovascular disease or alcohol abuse (34). Alcohol is known to have an impact on the disease and affect levels of depression as well as QoL (34). Furthermore, alcohol is an additional triggering factor for shame (35). Given the absence of information about alcohol consumption in the medical records of our patients, we were unable to assess this factor in the present study. Further investigations on the subject of alcohol will be necessary to prevent disease exacerbation caused by alcohol abuse and sensitize physicians to this issue during their consultations with patients.
In conlusion, skin shame plays an essential role in psoriasis because it aggravates the burden of disease and QoL. In view of the importance of a patient’s psychosocial environment, a physician-patient relationship based on trust should be given greatest priority. This holistic view must include shame as a significant psychological disease burden because shame is liable to affect the course of the disease, its attendant psychological disabilities, and economic concerns. The feeling of shame combined with a lack of self-esteem leads to higher levels of stress and mental illness. This vicious circle may aggravate flares of the disease, its recurrence, as well as the severity and duration of symptoms. Future studies should address the impact of shame in a more representative sample size.
This project was funded by a prize for “Dermatologist from the Heart” awarded by the Austrian Dermatologic Society in 2017.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize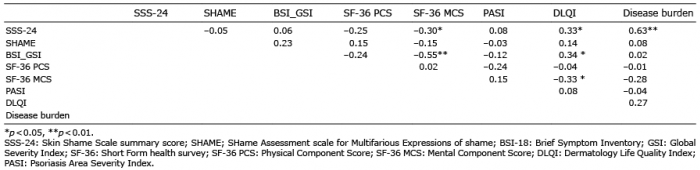 Click to show fullsize
Click to show fullsize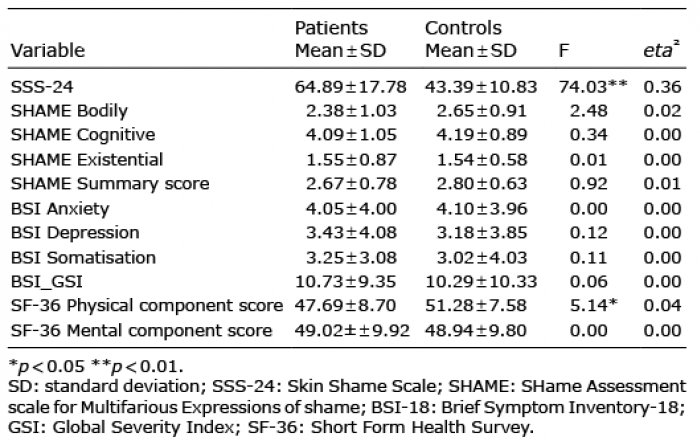 Click to show fullsize
Click to show fullsize