


1UOC Dermatologia, and 2Department of Pathophysiology and Transplantation, Università degli Studi di Milano, Foundation IRCCS, Cà Granda Ospedale Maggiore Policlinico, Via Pace 9, IT-20122 Milan, Italy. *E-mail: valenbenzecry@gmail.com
Accepted Jun 10, 2020; Epub ahead of print Jun 12, 2020
Acta Derm Venereol 2020; 100: adv00207
Dupilumab is a fully human monoclonal immunoglobulin (Ig)G4 antibody that inhibits the T-helper type 2 (Th2) cytokines interleukin (IL)-4 and IL-13 by targeting the IL-4Rα subunit, thereby inhibiting the JAK-STAT path-way. Dupilumab is known for its excellent efficacy and safety in patients with atopic dermatitis (AD) and has not been associated with increased infections (1). We report here a case of disseminated molluscum contagiosum (MC) during dupilumab therapy.
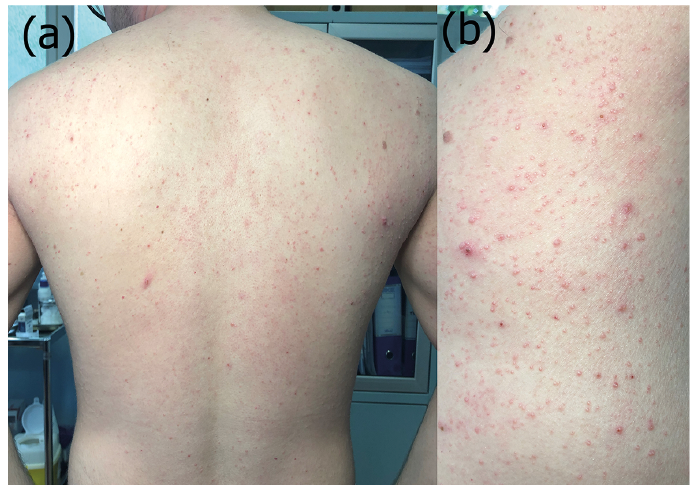
The patient was a 26-year-old man with persistent and severe AD since childhood. He was treated unsuccessfully with topical corticosteroids and calcineurin inhibitors, narrow band-ultraviolet B (UVB) and cyclosporine. The patient also had 3 MC on his right shoulder, which had appeared 2 years previously. He started on dupilumab (starting dose 600 mg, followed by 300 mg every other week). Two weeks later, the patient presented with rapidly spreading MC involving the trunk and upper limbs (Fig. 1), causing significant psychological distress. Curettage of several lesions, including the larger and more acutely inflamed MC, was performed on the 3rd and 6th weeks. The treated lesions healed, while the numerous residual MC that were not treated gradually regressed until complete resolution without scarring at week 9. At the 16th week of follow-up, no additional MC were observed (Fig. 2). The control of AD was excellent: Eczema Area and Severity Index (EASI): 6 (baseline 24), numerical rate scale (NRS) for pruritus: 2 (baseline 9), Dermatology Life Quality Index (DLQI): 3 (baseline 20).
Fig. 1. Clinical photographs. (a) Extension of molluscum contagiosum infection 2 weeks after the beginning of dupilumab therapy (b) Close-up of numerous molluscum contagiosum.
Fig. 2. Complete resolution of molluscum contagiosum without scarring at the 16th week of dupilumab therapy.
MC is a common, often self-limited, viral infection. Patients with severe AD may be at an increased risk of disseminated MC, probably due to factors such as impaired barrier function, skin damage associated with scratching, alterations in the skin microbiome, reduced expression of antimicrobial peptides (AMP) (2), frequent use of topical steroids/immunomodulators and systemic immunosuppressive therapies.
In a recent meta-analysis of randomized controlled trials, dupilumab was associated with a 46% decrease in skin infections compared with placebo (1). To our knowledge, despite the wide use of dupilumab for AD, only 2 reports of disseminated MC during dupilumab therapy have been reported in the literature (3, 4). In 4 patients MC dissemination was observed at the 4th week of therapy and spontaneously disappeared by week 32 (4). In another case, despite cidofovir administration, dupilumab therapy was stopped because of worsening of MC (3).
Although the exact mechanism is unknown, a poss-ible explanation for the extension of a pre-existing MC infection is that, since AMP expression is known to be inhibited by Th2 cytokines (5), dupilumab-induced dual inhibition of IL-4/IL-13 signalling led to an increase in b-defensins and LL-37 (1), aiding resolution of MC. Moreover, curettage probably shortened the time to resolution (6 weeks, compared to 14 to 28 weeks) (4).
Dermatologists should be aware of this possible “side-effect”’ of dupilumab, which probably illustrates the rapid modulation of immune response and progressive improvement in skin barrier function induced by inhibition of the IL-4/IL-13 pathway.
Informed consent was obtained from the patient for publication of this article.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize