


1Department of Dermatology, CHR Orléans, FR-45000 Orléans, 2Department of Dermatology, University of Tours, CHRU Tours, 3Plateform IBiSA of Electron microscopy, INSERM U1259, University of Tours, Tours, France, and 4Department of Pathology, CHR Orléans, FR-45000 Orléans. E-mail: anne.moineau@gmail.com
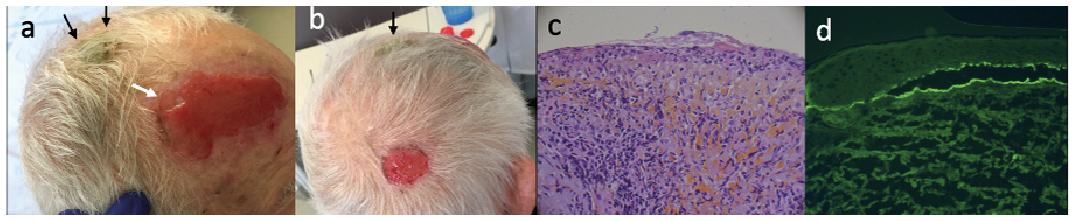
A 75-year-old man, whose main medical history was surgical removal of a basal cell carcinoma on the vertex 5 years ago, presented 3 large dome-shaped plaques that had emerged several weeks earlier. Bowen’s disease was suspected and he was treated with cryotherapy, without success. Physical examination revealed 2 well-defined erosive plaques with excessive granulation tissue localized on the forehead and parietal scalp (Fig. 1a, b). The lesion on his forehead also had peeling epidermis on the posterior part (Fig. 1a, white arrow). The vertex lesion was a well-defined hyperkeratotic plaque (Fig. 1a, black arrows). There was no Nikolsky’s sign. The lesions were neither itchy nor painful. There were no other skin lesions and no mucosal involvement. The patient did not report any other somatic symptoms, and the results of standard laboratory tests were normal.
A punch biopsy in the centre of the forehead erosive plaque revealed non-specific erosion without malignancy (Fig. 1c). Direct immunofluorescence assay of peripheral erosive skin tissue was performed (Fig. 1d).
What is your diagnosis? See next page for answer.
Fig. 1. (a) Erosive plaque with excessive granulation tissue on the forehead in a 75-year-old man. (b) Erosive lesion on the parietal scalp and hyperkeratotic plaque on the vertex (black arrows). (c) Histology: superficial ulceration with absent epidermis and presence within the dermis of an inflammatory infiltrate composed of eosinophils, lymphocytes and plasmocytes (Haematoxylin-Eosin ×40). (d) Direct immunofluorescence: thin, continuous and linear immunoglobulin G (IgG) deposits along the dermal–epidermal junction.
Acta Derm Venereol 2020; 100: adv00208.
Diagnosis: Brunsting-Perry variant of cicatricial pemphigoid
On clinical presentation, multiple skin carcinomas (Bowen’s disease), erosive pustular dermatosis and Brunsting-Perry pemphigoid were suspected. Direct immunofluorescence of the periphery of the erosive skin lesion revealed thin, continuous and linear IgG and C3 deposits bound to both the roof and floor of the sub-epidermal blister. Enzyme-linked immunosorbent assay (ELISA) findings were positive for a BP180 NC16a fragment at 31 UI/ml (n < 20). The search for anti-laminin-332 antibody was negative. Immunoelectron microscopy analysis of the forehead peripheral skin lesion confirmed cicatricial pemphigoid with granular deposits of IgG and C3 along the dermal–epidermal junction (Fig. 2a) in the lamina densa. Lack of deposits under the lamina densa excluded acquired bullous epidermolysis (Fig. 2b).
The patient first received topical clobetasol, with no improvement. He then received 100 mg dapsone per day, which led to healing of the erosive plaques after 4 months of treatment, but left cicatricial alopecia. Dapsone was maintained for 12 months with no disease relapse.
Brunsting-Perry pemphigoid is a rare sub-epidermal blistering disease, originally described by Brunsting & Perry in 1957 as a rare variant of cicatricial pemphigoid, which is characterized by inflammatory plaques and bullous lesions limited to the head, neck, scalp, and upper trunk, with mild or no mucosal involvement (1). The lesions induce secondary cicatricial alopecia.
The current case of Brunsting-Perry is atypical in its presentation because the patient never reported having blisters. Moreover, excessive granulation of erosive cutaneous plaques is rare in cicatricial pemphigoid. It can be confused with skin carcinoma or an erosive pustular dermatosis (but the lack of efficacy of clobetasol was not consistent with the latter diagnosis). The epidermal peeling bordering excessive granulation tissue was a clue to suspect sub-epidermal blistering disease in our case (white arrow).
Target antigens described include BP180 (2, 3), BP230 (3, 4), laminin-332 (4), desmoplakins I/II (4), LAD-1 (5) and type VII collagen (6, 7).
Brunsting-Perry pemphigoid has also been described as a possible clinical variant of epidermolysis bullosa acquisita (6,7); however, the pathogenic mechanisms and autoantigens in this condition remain debated. In a recent review, type VII collagen was the second most common target antigen detected after BP180 in Brunsting-Perry pemphigoid (4 of 11 cases with identified target antigens) (7). The phenomenon of epitope spreading, which would unmask different antigens, could explain the divergent findings of the immunofluorescence against a single phenotype (8).
Cicatricial pemphigoid is an autoimmune sub-epidermal blistering disease clinically characterized by elective mucosal involvement and healing with synechia in the mucous membrane subtype. The cutaneous involvement is inconsistent. The clinical polymorphism of cicatricial pemphigoid is associated with significant immunopathological heterogeneity. Usually, there are a few skin lesions represented by blisters and chronic erosions. Milium grains and depressed atrophic scars are present. They predominate on the head and neck or even the thorax.
Other immunopathological techniques allow for a differential diagnosis of certainty with acquired epidermolysis bullosa. Immunoblotting revealed reactivity on an epidermal extract, with a 180-kDa protein most often corresponding to the BP180 antigen of bullous pemphigoid. Autoantibodies to laminin-332 must be sought when indirect immunofluorescence reveals autoantibody deposits on both the floor and roof of the sub-epidermal blister, because the presence of autoantibodies to laminin-332 was associated with increased relative risk of cancer in a series of 35 patients (9), but this finding was not confirmed in a case-control study of 154 patients (10). However, anti-laminin-332 autoantibodies are more likely to be present when mucous membrane pemphigoid is severe (10).
Treatment of cicatricial pemphigoid lacks international consensus. In most cases, dapsone is the first-line treatment (11). Sulphasalazine or cyclin can also be used after failure or when dapsone is contraindicated. Second-line treatments include prednisolone, intravenous methylprednisolone, cyclophosphamide, mycophenolate mofetil, intravenous immunoglobulin, etanercept and rituximab. The combination of several drugs may be required (12).
In conclusion, Brunsting-Perry disease could be a clinical expression of different sub-epidermal blistering diseases. Clinicians should be aware that its clinical presentation could simulate other skin conditions, as in the current case, with excessive granulation tissue leading to a differential diagnosis with cutaneous cancer.
Fig. 2. Immunoelectron microscopy of scalp skin biopsy (×30,000); dermis is naked because of the epidermal blister cleavage (asterisk). High magnification (inset). (a) Discontinuous dot-shaped IgG deposits in the lamina densa (LD), indicated by arrowheads (results are similar to anti-C3 antibody findings). (b) Lack of specific immunolabelling with anti-IgA antibody (results similar to anti-IgM antibody findings).


 Click to show fullsize
Click to show fullsize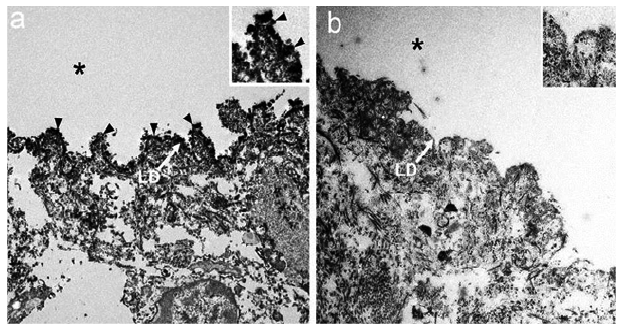 Click to show fullsize
Click to show fullsize