


Little is known about psoriasis in geriatric patients, whereas treating this growing population can be challenging due to comorbidities, comedication and physical
impairments. To compare disease and treatment characteristics of psoriasis patients ≥ 65 years old with patients < 65 years old, a self-assessment survey was sent to all members of the Dutch Psoriasis Association (n = 3,310). In total, 985 (29.7%) patients returned the survey, 414 (43.6%) respondents were ≥ 65 years old. Patients ≥ 65 years old had experienced erythrodermic psoriasis significantly more frequently than patients < 65 years old, other disease characteristics were highly comparable. Despite a significantly higher prevalence of comorbidities and comedication use in patients ≥ 65 years old, no difference was seen between the age groups regarding systemic antipsoriatic treatment (38.3% in ≥ 65 years old vs 42.3% in < 65 years old; p = 0.219). Remarkably, treatment-related side-effects were reported more frequently by patients < 65 years old. In conclusion, age alone should not be a limiting factor in psoriasis management, and proper attention must be paid to additional patient-related factors.
Key words: psoriasis; dermatological agents; frail elderly; aged; geriatric population; surveys; questionnaires.
Accepted Jun 15, 2020; Epub ahead of print Jun 16, 2020
Acta Derm Venereol 2020; 100: adv00215.
Corr: Marieke van Winden, Department of Dermatology, Radboudumc, PO Box 9101, 6500HB Nijmegen, The Netherlands. E-mail: Marieke.vanWinden@radboudumc.nl
Little is known about geriatric psoriasis, although health problems and medication can complicate the management of psoriasis. To compare characteristics of patients ≥ 65 years old with those < 65 years old, a survey was sent to all members (3,310) of the Dutch Psoriasis Association. In total, 985 (29.7%) patients returned the survey, 414 (43.6%) respondents were ≥ 65 years old. Despite more comorbidities and medication use in ≥ 65 years old, no difference was seen between age groups regarding systemic antipsoriatic treatment (38.3% vs 42.3%). Side-effects were reported more frequently by patients < 65 years old. Thus, age alone should not limit psoriasis treatment, and proper attention must be paid to patient-related factors.
Psoriasis is an immune-mediated inflammatory disease which is frequently seen in older adults. As the ageing world population continues to expand, dermatologists will increasingly be confronted with patients aged 65 years and older. Although the exact prevalence of psoriasis in older adults is unknown, it is estimated to range from 1% to 19% (1–3). Balancing the possible risks of antipsoriatic therapies in older adults and optimal psoriasis treatment can be challenging, due to factors such as comorbidities, concomitant medication, physical impairments and changing pharmacokinetics and pharmacodynamics (4, 5).
Little research has been conducted concerning disease and treatment characteristics in older psoriasis patients, or “geriatric psoriasis” (Fig. S1). The few available studies show similar disease severity compared with younger patients, although prescribed therapies appear to differ (6, 7). Moreover, data concerning the use of systemic treatment in geriatric psoriasis are scarce, since older adults are frequently excluded from clinical trials (8, 9). Therefore, it is currently unclear what risks are associated with antipsoriatic treatment in this growing population and whether geriatric patients with psoriasis are treated optimally.
To improve patient-centred clinical care in geriatric psoriasis, more knowledge needs to be acquired in this particular patient group. The objective of this study was therefore to provide more insight into the disease and treatment characteristics in older adults with psoriasis compared with younger patients.
Study design and participants
A nationwide cross-sectional study was conducted to assess the clinical characteristics of older adult patients with psoriasis, as well as current and previous treatments. A self-assessing multimodality survey was sent to all members of the Dutch Psoriasis Association (n = 3,310), along with study information and a prepaid envelope. In addition to this paper-based version, a hyperlink to the online web-based survey (Qualtrics, Provo, UT, USA) was provided and printed repeatedly in the Dutch Psoriasis Association Magazine. Returning the survey was construed as informed consent. Approval from the Research Ethics Committee of Radboud University Medical Centre was obtained before starting the study. This study was reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) criteria (10).
Survey
A survey was developed based on an extensive review of the literature, patient interviews, and multiple meetings with a multidisciplinary focus group consisting of physicians in dermatology and rheumatology, (specialized) nurses, clinical researchers, and a dermato-psychologist. The survey included multiple sections enquiring about sociodemographic aspects, psoriasis characteristics and associated therapy using multiple choice questions, Likert scales, and visual analogue scales. Furthermore, open-ended questions were added to each section to further evaluate relevant items not captured by the questions included in the survey, answers were categorized for further analyses. Disease severity was measured using the Self-Administered Psoriasis Area Severity Index (SAPASI), a validated patient-assessed instrument based on the frequently used Psoriasis Area Severity Index (11). The SAPASI ranges from 0 to 72 and can be classified into 4 categories: in remission (SAPASI = 0), mild (> 0 ≤ 3), moderate (> 3 ≤ 15) and severe (> 15) (12). Prescribed therapies were categorized into 4 different groups: topical therapy, phototherapy, conventional systemic therapy, and modern systemic therapy (biologics and small-molecule inhibitors). Body mass index (BMI) was calculated based on reported weight and height. Polypharmacy was defined as the simultaneous use of 5 or more medications (13). A pilot study was performed in 10 geriatric patients with psoriasis prior to distribution of the survey to improve its quality, and assess the relevance and comprehensibility of the questions, instructions and response options.
Data processing and analysis
Data were processed anonymously using the automatic form identification software Remark Office Optical Mark Recognition, version 9.5 (Gravic, Inc. Malvern, PA, USA) and Castor Electronic Data Capture, a web-based data management system in compliance with Good Clinical Practice (GCP) standards (Castor Research Inc., Hoboken, NJ, USA). To ensure correct data entry, 10% of the data entry was checked manually by an independent researcher who was not involved in data entry. Statistical analyses were performed using Statistical Package for Social Sciences (SPPS) Statistics for Windows, version 25.0 (IBM, Armonk, NY, USA). Descriptive statistics were used to summarize categorical data as frequencies and percentages and continuous variables as mean ± standard deviation (SD) or median (range), as appropriate according to the distribution of the data. Missing values were excluded from analyses. Patients were categorized into 2 age groups; patients ≥ 65 years old and patients < 65 years old. Comparisons were made using Student’s t-test or Mann–Whitney U test for continuous variables, and the χ2 or Fisher’s exact test for categorical variables. Subgroup analyses were performed comparing outcome measures of patients ≥ 80 years old with patients < 80 years old, and comparing patients with early disease onset (onset of symptoms before the age of 40 years) and patients with late disease onset (onset of symptoms after the age of 40 years) (14). Logistic regression was used to correct for confounding variables and to determine odds ratios (ORs). Age and sex distribution of the respondent population were compared with the target population to test for non-response bias, using available current data on the members of the Dutch Psoriasis Association and previous research in this population (15).
Study participants
Between 11 December 2018 and 4 September 2019, 3,310 patients with psoriasis were approached for participation. In total, 985 (29.7%) surveys were returned. Due to missing age values, 27 respondents were excluded from analyses. Eight more respondents were excluded from analyses due an insufficient number of answered items (e.g. responses to age and sex only). The remaining 950 respondents were suitable for analysis. The mean ± SD age was 61.1 ± 13.7 years, range 7–95, and 414 (43.6%) of the respondents were ≥ 65 years old. Of these, 58 (14.0%) respondents were ≥ 80 years old. A full overview of responder characteristics is given in Table I. Although a significant difference in sex was seen between patients ≥ 65 years old vs those < 65 years old, results after stratification for sex did not differ from the main analysis (data not shown).
Non-response bias was assessed by comparing age and sex distribution of the study respondents with the target population; no significant differences were found (Table SI). Since 95.5% (n = 879) of the surveys were returned in the winter, an additional analysis on seasonal difference was performed; no significant impact on outcome measures was seen. There were no significant differences in outcome measures between paper-based and web-based responses (data not shown).
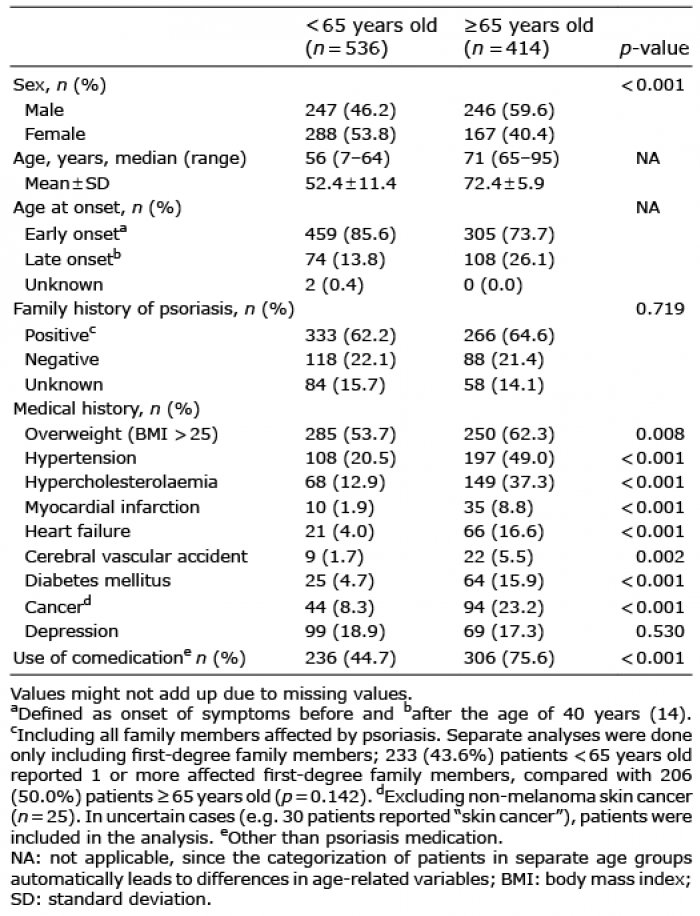
Table I. Responder characteristics of geriatric psoriasis patients (≥65 years old) compared with patients < 65 years old
Comorbidities and medical history
Except for depression, all reported comorbidities were significantly more common in patients ≥ 65 years old, as is illustrated in Table I. A cardiovascular risk profile (e.g. obesity, hypertension, hypercholesterolaemia, diabetes mellitus, myocardial infarction, heart failure and cerebral vascular accident) was more prevalent in patients ≥ 65 years old compared with patients < 65 years old. Moreover, patients ≥ 65 years old had a significantly higher BMI (median 26.2 (range 17.7–65.9 kg/m2) in ≥ 65 years old vs 25.4 (14.3–56.1 kg/m2) in < 65 years old; p = 0.006). A (history of) malignancy was significantly more often reported by patients ≥ 65 years old compared with patients < 65 years old (n = 94 (23.2%) vs 44 (8.3%) respectively; p < 0.001). Of all patients reporting a (history of) malignancy, 71 (43.3%) reported skin cancers (35.2% non-melanoma skin cancer, 22.5% melanoma, 42.3% unknown type of skin cancer).
The use of concomitant medication was reported by 306 (75.6%) patients ≥ 65 years old, vs 236 (44.7%) patients < 65 years old (p < 0.001). The most frequently used types of concomitant medication were cardiovascular drugs (n = 211 (69.0%) ≥ 65 years old vs n = 104 (44.1%) < 65 years old; p < 0.001) and antidiabetic drugs (n = 42 (13.7%) ≥ 65 years old vs n = 21 (8.9%) < 65 years old; p = 0.004). Moreover, polypharmacy was significantly more prevalent in patients ≥ 65 years old (n = 103 (30.7%) ≥ 65 years old vs n = 47 (13.9%) < 65 years old; p < 0.001).
Disease characteristics
As shown in Table II, plaque psoriasis and psoriasis capitis were the most frequently reported clinical psoriasis types currently present in both patient groups (cumulative prevalence: 67.2% and 70.6%, respectively). Patients ≥ 65 years old had experienced erythrodermic psoriasis significantly more frequently than patients < 65 years old (n = 70 (17.1%) ≥ 65 years old vs n = 31 (5.8%) < 65 years old; p < 0.001). Comparable rates of psoriatic arthritis were reported in both age groups (n = 158 (38.5%) ≥ 65 years old vs n = 193 (36.2%) < 65 years old; p = 0.464). Guttate and genital psoriasis were significantly more frequently reported by patients < 65 years old. In both groups, patients experienced their first symptoms of psoriasis most frequently before the age of 18 years (n = 136 (32.9%) ≥ 65 years old vs n = 219 (40.9%) < 65 years old). Of all patients ≥ 65 years old, 65 (15.7%) reported disease onset after the age of 50 years, 14 (3.4%) respondents reported disease onset after the age of 65 years, as is illustrated in Fig. S2.
Table II. Disease and treatment characteristics of geriatric patients with psoriasis (≥65 years old) compared with patients < 65 years old
A subgroup analysis was performed to compare disease characteristics in patients ≥ 65 years old with early disease onset with those with late disease onset. Erythrodermic psoriasis was significantly more frequently reported by patients with early disease onset (n = 63 (20.8%) vs n = 7 (6.5%); p = 0.001), as well as psoriasis unguium (n = 160 (52.8%) vs n = 42 (39.3%); p = 0.016). Other disease characteristics did not differ between the onset groups.
The majority of all patients had never experienced a period of total skin clearance (n = 228 (55.6%) ≥ 65 years old vs n = 302 (56.7%) < 65 years old; n = 0.774). Only 82 (8.7%) patients in the total study population experienced a period of total skin clearance longer than 3 years in a row. Although patients ≥ 65 years old reported a slightly lower current SAPASI score compared with patients < 65 years old (median 5.24 (0–20.2) in ≥ 65 years old vs 5.72 (0–35.5) in < 65 years old; p = 0.016), disease severity was considerably high in both groups, as most patients currently received antipsoriatic treatment. When comparing the age groups according to categorized SAPASI scores, no significant difference was seen in disease severity; a current moderate disease activity was reported by 266 (68.9%) patients ≥ 65 years old, severe psoriasis was reported by 17 (4.4%) patients ≥ 65 years old, whereas 371 (71.1%) patients < 65 years old reported a moderate disease activity and 33 (6.3%) a severe disease activity (p = 0.260).
Antipsoriatic treatment
As shown in Table II, there were no significant differences in currently used therapies by patients ≥ 65 years old compared with patients < 65 years old. No significant difference was seen between the age groups regarding the use of conventional systemic therapies (n = 107 (26.1%) ≥ 65 years old vs n = 140 (26.4%) < 65 years old; p = 0.913), nor in the use of modern systemic therapies (n = 63 (15.4%) ≥ 65 years old vs n = 100 (18.9%) < 65 years old; p = 0.160). A combination of systemic agents was used by 17 (4.1%) patients ≥ 65 years old and 22 (4.2%) patients < 65 years old (p = 0.997). When comparing the specific systemic agents between the age groups, no significant differences were seen. As is shown in Fig. S3, most frequently used systemic agents were fumaric acid, methotrexate and adalimumab in both age groups (cumulative respectively 34.1%, 30.2% and 16.0%). No significant differences between the age groups were seen in previously used therapies.
A separate analysis comparing patients ≥80 years old (n = 58) with patients p = 0.759). Modern systemic therapies were used in 6 (10.5%) patients ≥ 80 years old, compared with 157 (17.8%) patients p = 0.161). A significant higher number of patients ≥ 80 years old were currently treated with phototherapy, although the sample size was quite small (n = 8 (14.0%) vs n = 38 (4.3%); p = 0.001), as is summarized in Table SII.
Adverse events were reported significantly more frequently by patients < 65 years old compared with patients ≥ 65 years old, even after correction for type of treatment (only topical therapy, UV therapy with or without topical therapy, conventional systemic therapy with or without topical or UV therapy, modern systemic with or without topical or UV therapy and combined systemic therapies with or without topical therapy, OR: 1.57; 95% CI: 1.09–2.25; n = 0.015).
Patients ≥ 65 years old were significantly more often dependent on assistance with treatment or skin care compared with patients < 65 years old (n = 56 (14.9%) ≥ 65 years old vs n = 46 (9.0%) < 65 years old; p = 0.007); 47 (83.9%) were helped by a partner or family member, and 9 (16.1%) relied on medical caretakers or others. Of all patients ≥80 years old, 11 (20.8%) were dependent on others, 6 (54.5%) were assisted by a partner or family member, and 5 (45.5%) by medical caretakers. No difference was seen among the age groups in the daily amount of time patients spent on their treatment or skin care. Most patients spent less than 30 min per day on psoriasis management (n = 352 (92.9%) ≥ 65 years old vs n = 481 (94.3%) < 65 years old; p = 0.635).
Managing psoriasis in older adults can be a clinical challenge, due to factors such as comorbidity, concomitant medication, ageing-related organ impairment and functional deterioration. Limited data are available to guide clinicians in treating this growing patient group. The aim of this study was to evaluate disease and treatment characteristics in geriatric psoriasis patients and to identify differences compared with a younger population.
In this large cross-sectional study, plaque psoriasis and psoriasis capitis were the most frequently reported types of psoriasis in both groups. Erythrodermic psoriasis was significantly more often reported by patients ≥ 65 years old, in line with previous research (6, 7, 21). A possible explanation for this difference could be that patients ≥ 65 years old have been treated with less potent therapies in the past during prolonged periods of time, increasing the potential of developing more severe and extensive psoriasis. Furthermore, since the question was posed whether patients had ever experienced an episode of erythrodermic psoriasis in the past, the a priori chance is higher in older patients due to the higher number of cumulative disease years. This too explains the fact that erythrodermic psoriasis was reported more frequently by patients with early disease onset, as has also been stated previously (14). Other types of psoriasis have been studied to a lesser extent; Phan et al. reported a higher prevalence of guttate psoriasis in patients ≥70 years old compared with patients < 70 years old (21). In other studies, including the current study, this difference was not seen (6, 7).
In this study, the majority of patients ≥ 65 years old reported a moderate current disease activity, although median SAPASI scores were slightly higher in patients < 65 years old. Previous studies are in line with these results, showing comparable disease severity in both age groups (6, 7). Strikingly, the majority of the respondents in both groups reported never having achieved total skin clearance, while total clearance of psoriasis is frequently mentioned as one of the most important treatment goals to improve quality of life in patients with psoriasis (22, 23). It seems that psoriasis treatment in both age groups could be further improved, tailored to individualized treatment goals. Currently, little research is available assessing treatment goals and quality of life in geriatric psoriasis patients specifically, to evaluate whether patients consider themselves optimally treated.
Patients ≥ 65 years old reported significantly more comorbidities and concomitant medication in comparison with patients < 65 years old, in line with previous research (7, 21). Comorbidities and concomitant medication should be acknowledged when considering management options, especially with regard to contra-indications of antipsoriatic therapies. Despite a significant higher prevalence of (relative) contra-indications for several antipsoriatic systemic therapies reported by patients ≥ 65 years old, no significant differences were found between the age groups when comparing the individual systemic agents. Even in a subgroup analysis of patients ≥80 years old, systemic therapies did not differ significantly from in younger patients, although the number of patients ≥80 years old using modern systemic therapies was small. This is in contrast with previous studies stating that (modern) systemic therapies are less often prescribed in older patients (7, 21, 24, 25). Some studies suggest that prescription of systemic therapies increases over time, due to the fact that physicians have gained more experience with these therapies and are therefore more comfortable with prescribing systemic therapies, explaining the difference between the present study results and those found in previous studies (7, 24). Another explanation could be that the treatment goals and preferences of patients ≥ 65 years old have changed over time, although available literature in this field is scarce (23). Significantly more patients ≥ 65 years old required assistance with treatment or skin care, it is therefore important to consider this aspect in choosing antipsoriatic treatment.
In order to minimize the risks of potential drug interactions, as well as treatment-related adverse events, managing psoriasis in patients with comorbidities and concomitant medication requires extra attention. In this study, significantly fewer adverse events were reported by patients ≥ 65 years old, even when corrected for the type of treatment. It should be noted that this involves only self-reported side-effects and probably does not include asymptomatic treatment-related laboratory changes. Moreover, the reasons for ceasing previous therapies were not evaluated, which could be related to adverse events experienced in the past. Available research varies widely concerning the rates of adverse events and tolerability profiles in older adults, frequently stating adverse event rates do not differ between age groups (6, 7, 25–27). More real-life data is needed to provide clarity and guidance in this field.
Limitations
This study has certain limitations due to the study design. Firstly, any survey is associated with a risk of recall bias and misinterpretation of the questions, although this risk was minimized by pre-testing the survey in a pilot study. Since all participants were members of a patient association, a risk of selection bias exists. A higher level of education was seen in the study population compared with the Dutch overall population (17), which might be associated with membership of a patient association altogether (Table SIII). Moreover, members of a patient association might be older (16, 18–20) and have more severe psoriasis than the overall psoriasis population (20). Since this study aimed to study a population representative of daily dermatological care, it was assumed that the Dutch Psoriasis Association closely resembles the target population. A relatively large cohort of patients ≥ 65 years old responded compared with the composition of the Dutch population. The survey was introduced explaining the nature of the study; to study differences in psoriasis management and characteristics among different patient age groups. Therefore, patients ≥ 65 years old may have been stimulated to respond, whereas patients in middle-age felt less urge to respond (sampling bias). However, age and sex distribution of the respondent population were shown to be representative for the target population. In addition, response rates were similar to previous studies with comparable study designs (15, 28). Moreover, the current study comprised one of the largest geriatric psoriasis populations described so far.
Conclusion
Treating geriatric patients with psoriasis requires extra attention to comorbidities and the use of concomitant medication, since these were significantly more frequently seen in patients ≥ 65 years old than in patients < 65 years old. Despite these obvious differences in patient-related characteristics, a better tolerability profile was reported by patients ≥ 65 years old. Based on the results of this study, chronological age alone should not be a limiting factor in choosing antipsoriatic therapy, although patient-related characteristics must be considered; physical impairments, availability and necessity of help, and possible drug-interactions can complicate treatment decisions. In order to provide personalized medicine, more research on treatment goals and patient preferences in geriatric psoriasis patients is needed to further guide clinicians in optimally treating this growing patient group.
The authors would like to thank all respondents who completed the survey, and the Dutch Psoriasis Association for their efforts regarding this study. Moreover, the authors would like to thank the focus group members for their input, especially J. van den Reek, M. Kooijmans-Otero, S. Spillekom van Koulil, M. Eilander, M. Teunissen, A. van der Wielen-Willems.
Funding source: This investigator-initiated study was conducted with financial support from Almirall. The funding source had no influence on study design, data collection and analysis, or the content of the manuscript.
Conflicts of interest: MECvW has carried out investigator-initiated research with financial support from Almirall and has carried out clinical trials for AbbVie, Celgene, Janssen, Leo Pharma, Lilly, and Novartis. PCMvdK served as the chief medical officer of the International Psoriasis Council and received fees for lectures and consultancies from Bristol-Myers Squibb, UCB, Leo Pharma, Eli Lilly and Company, Dermavant, Almirall, Celgene, Novartis, Janssen, and AbbVie. EMGJdJ has received research grants for the independent research fund of the Department of Dermatology of Radboud University Medical Centre Nijmegen, the Netherlands from AbbVie, Pfizer, Novartis, Janssen Pharmaceutica and Leo Pharma, has acted as consultant and/or paid speaker for and/or participated in research sponsored by companies that manufacture drugs used for the treatment of psoriasis including AbbVie, Janssen Pharmaceutica, Novartis, Lilly, Celgene, Leo Pharma, UCB and Almirall. All funding is not personal, but goes to the independent research fund of the Department of Dermatology of Radboud University Medical Centre Nijmegen, the Netherlands. SFKL has received research grants for investigator-initiated research by Almirall. No other potential conflicts of interest were reported.


 Click to show fullsize
Click to show fullsize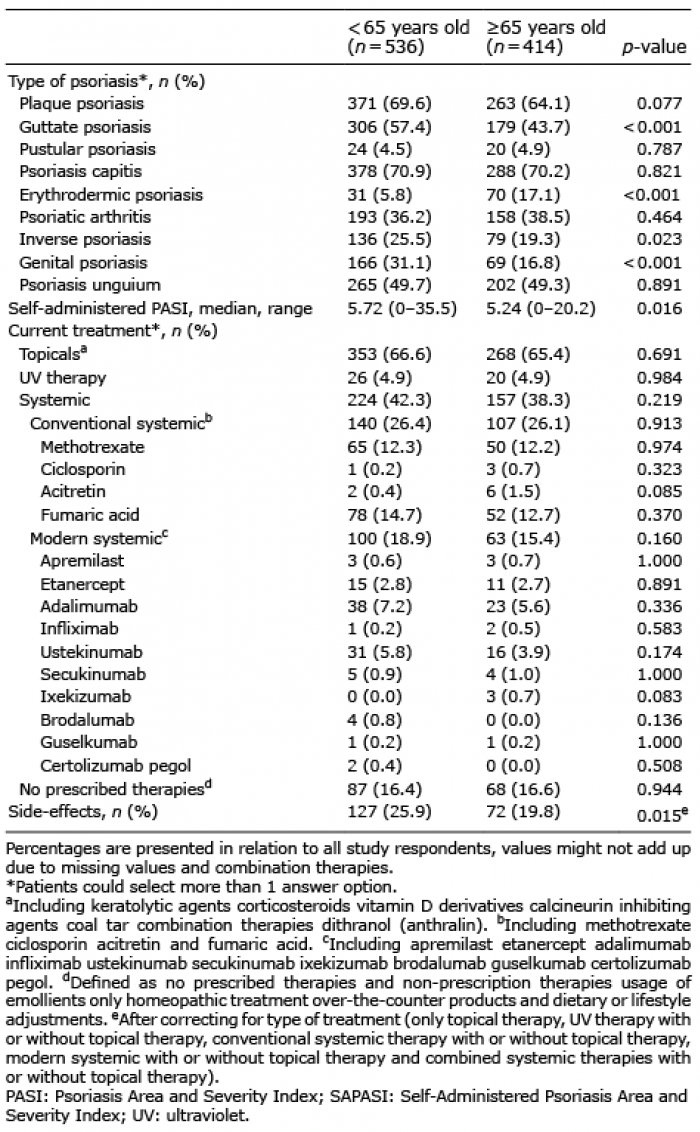 Click to show fullsize
Click to show fullsize