


1Departments of Dermatology and 5Pediatrics, Nagoya University Graduate School of Medicine, 65 Tsurumai-cho, Showa-ku, Nagoya 466-8550, Departments of Dermatology, 2Juntendo University Urayasu Hospital, Urayasu, 3Odawara Municipal Hospital, Odawara, 4Center for Advanced Medicine and Clinical Research, Nagoya University Hospital, Nagoya, Japan, and 6St John’s Institute of Dermatology, King’s College London, Guy’s Hospital, London, UK. *E-mail: takeichi@med.nagoya-u.ac.jp; makiyama@med.nagoya-u.ac.jp
Accepted Jun 15, 2020; Epub ahead of print Jun 16, 2020
Acta Derm Venereol 2020; 100: adv00209
“Keratinopathic ichthyoses” has been proposed as an umbrella term for epidermolytic ichthyosis (EI), superficial epidermolytic ichthyosis, annular epidermolytic ichthyosis, ichthyosis Curth–Macklin, autosomal recessive epidermolytic ichthyosis and ichthyosis with confetti (IWC) (1, 2). All types of keratinopathic ichthyoses are caused by variants in the keratin family genes KRT1, KRT2 or KRT10 (2). IWC is usually caused by frameshift variants in the C-terminal region that result in a delayed termination codon with downstream arginine-rich tail of the keratin protein, leading to nuclear localization of mutant keratin and/or (for arginine-rich tails) intermediate filament dysfunction (3–6). We describe here 3 patients with IWC who have a recurrent splice-site variant in KRT10 (Fig. 1a).
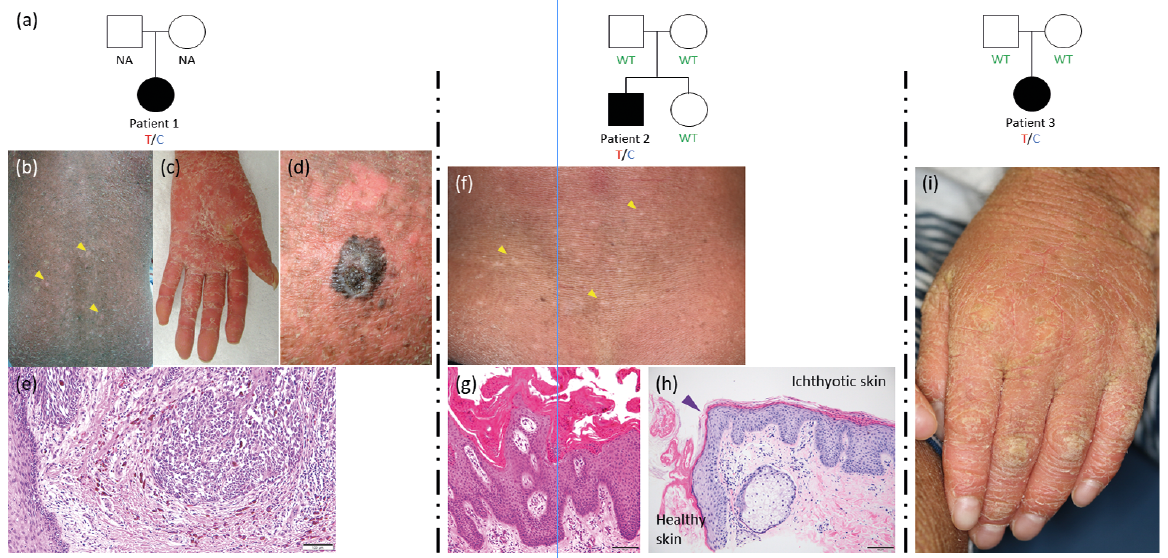
Fig. 1. Family trees and clinicopathological features of the 3 cases. (a) Pedigrees of 3 families and segregations of the variant c.1373+2T>C in KRT10. De novo variants in cases 2 and 3. “T/C” means heterozygous variants of c.1373+2T>C. WT: wild-type sequence; NA: not analysed. (b) Case 1. Normal-appearing white spots (yellow arrowheads) scattered on the back. (c) Case 1. Marked palmoplantar keratoderma on the left palm. (d) Case 1. A large black nodule on the right thigh. (e) Case 1. A haematoxylin-eosin-stained section of the skin tumour shows the proliferation of atypical melanocytes in various sizes with large nuclei, and mild lymphocytic infiltration in the upper dermis. (f, h) Case 2. Revertant spots (yellow arrowhead). Light microscopic observations of a pale revertant spot on the back demonstrate correction of the pathologic findings seen in (h). Purple arrowhead: a border between the affected, ichthyotic skin and the healthy skin. (g) Hyperkeratosis and parakeratosis with hypogranulosis are seen in the affected epidermis. Granular degeneration was not observed. (i) Case 3. Scaly hyperkeratosis with erythema and fissures is present on the dorsum of the left hand.
Case 1. A 47-year-old woman presented with a history of ichthyosis from birth. With ageing, several pale macules had developed on her trunk and limbs, suggesting IWC (Fig. 1b). She had severe palmoplantar keratoderma (PPK) (Fig. 1c). At age 24 years, she had a malignant melanoma (MM) in situ on the dorsal side of the right little finger. She underwent amputation of the right little finger following local recurrence 3 years after the initial resection surgery. At age 40 years, she noticed an irregular black nodule on the right thigh (Fig. 1d). Histologically, atypical melanocytes of various sizes were found in the rete ridges of the epidermis (Fig. 1e). Immunohistochemical analyses showed these melanocytes to be positive for anti-HMB45 and weakly positive for anti-S100 antibodies. The nodule was diagnosed as an in situ MM and was surgically excised.
Case 2. A 16-year-old boy exhibited redness and generalized skin scaling over the entire body since soon after birth. Examination revealed mild diffuse scaly erythema on the trunk and extremities. A skin biopsy specimen from his right lower leg showed marked hyperkeratosis with parakeratosis (Fig. 1g). With increasing age, several pale macules developed on his trunk and thighs (Fig. 1f). Histologically, orthokeratosis was seen in the pale macule (Fig. 1h).
Case 3. An 8-year-old girl presented with diffuse redness and scaling, which had appeared all over her skin during infancy. Examination revealed mild diffuse scaly erythema on her extremities (Fig. 1i).
Further clinical details for all 3 patients are presented in Table SI.
Following ethical approval, informed written consent was obtained in compliance with the guidelines of the Declaration of Helsinki. Using DNA from the 3 affected individuals, whole-exome sequencing was performed on the Illumina HiSeq 2500 (San Diego, CA, USA), as described previously (7) and in Appendix S1.
Interestingly, all 3 cases had a previously reported heterozygous splice-site variant in KRT10 (c.1373+2T>C) (8). Its presence in genomic DNA was confirmed by Sanger sequencing (Fig. S1a) and its absence in the parental genomic DNA of cases 2 and 3 was demonstrated (DNA from the parents of case 1 was not available), showing their variants to be de novo (Fig. 1a). Subsequently it was examined whether this splice-site variant is expected to lead to aberrant or normal splicing by RT-PCR, using RNA extracted from pulled hair samples of cases 2 and 3 (9). PCR was performed by using several primer pairs between exon 5 and exon 8 in KRT10 (Table SII). Only one aberrant splicing product was identified in the patient’s RNA (Fig. S1b). Aberrant splicing at the splice donor site of exon 6 causes a frameshift, generating a premature stop codon 6 codons downstream (p.Ser458Argfs*6) (Fig. S1c). In addition, immunohistochemical analyses were conducted with 2 anti-K10 antibodies and 1 anti-K1 antibody in lesional skin samples from cases 1 and 2. Brown dots, indicating aberrant nuclear localization of keratins 1/10, were visible in the nuclei of many epidermal keratinocytes in the patients’ skin (Fig. S2).
Probands in 2 families had de novo variants (Fig. 1a). c.1373+2T>C might therefore be a mutational hotspot for IWC in the Japanese population. With regards to EI, there are several well-known mutational hotspots in the helix initiation and termination motifs of K1 and K10 (2). In contrast, frameshift variants in the hotspot genomic region coding the C-terminal tail of K10 or K1 have been reported in IWC (4, 8, 10–12).
The variant c.1373+2T>C in KRT10 has been reported previously as a pathogenic variant in an individual with IWC (8). The patient was a 6-year-old girl with an initial clinical diagnosis of congenital ichthyosiform erythroderma. The first spots that raised suspicion of IWC developed when this patient was aged 4 years (8). In the literature, most patients with IWC have unique variants, most of which replace the endogenous glycine-rich tail with a polyarginine sequence in K1/K10, although a large intragenic deletion in KRT1 was also reported previously in IWC (3). In the current subjects, only one aberrant splicing product was identified, a truncated form of K10 containing a premature termination codon (p.Ser458Argfs*6) (Fig. S1c), notwithstanding that the methodology may not have been able to detect small quantities of either spliced products (e.g. containing polyarginine tails).
Aberrant nuclear localization of K1 and K10 was detected in the skin samples from cases 1 and 2 (Fig. S2). Renz et al. reported aberrant nuclear localization of K10 featuring an arginine-rich C-terminus, but not if featuring an alanine-rich C-terminus (6). Instead, the protein displayed cytoplasmic localization, consistent with wild-type and truncated forms of K10 (6). The cDNA sequencing showed only a truncated form of K10 and immunohistochemistry showed both cytoplasmic and aberrant nuclear localization of K10.
Case 1 has had 2 episodes of MM and a higher risk of developing non-melanoma skin cancers has been reported in adult patients with IWC (11). Indeed, we reported previously that a case of IWC caused by a KRT1 variant showed an ulcerated basal cell carcinoma (3). Nearly one-fifth of patients with IWC develop skin cancer at a young age (11, 13). From the present case alone, it was not possible to conclude whether IWC might be associated with occurrence of MM. Furthermore, cases 1 and 2 showed PPK. PPK was commonly believed to be a more prominent feature in patients with EI with variants in KRT1 than in those with variants in KRT10 (2). However, some exceptions exist where KRT10 variants have been identified in patients with severe EI and PPK (14). Although PPK is more prominent in EI patients with KRT1 variants than in those with KRT10 variants, PPK is known to be associated with most IWC cases, including cases with KRT10 variants (2, 11).
In conclusion, this study identified a recurrent splice site variant, c.1373+2T>C, in KRT10 in 3 unrelated Japanese subjects with IWC, which causes a premature termination codon variant and nuclear K10 staining in epidermal keratinocytes. Patients with IWC may also be at greater risk of developing skin malignancy.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize