


1Maruho Co., Ltd., Osaka, Japan, 2SHIELD center, Galderma S.A., New York, USA, 3Chitofuna Dermatology Clinic, Tokyo, Japan, 4Benesse Style Care Co., Ltd., Tokyo, Japan, 5Takase Clinic, Tokyo, Japan, 6Saint-Care Holding Corporation, Tokyo, Japan, 7Research and Development, Galderma S.A., Sophia Antipolis, France
#These authors contributed equally.
A total of 185 elderly Japanese patients with mild to severe dementia were surveyed on itch, using multiple methods of evaluation including self-evaluation of itch conducted by patients as well as evaluation of scratching behavior and scratching marks on the body surface conducted by others. As a result, 36.8% self-evaluated that they were suffering from itch, whereas 53.5% were found to scratch. Of those who by themselves denied the presence of itch, 31.4% were found to scratch. Dry skin was found in 74.1%, the severity of which was positively correlated to the rating of scratching behavior and marks. These results indicate a high prevalence of pruritus in patients with dementia, and suggest that one should not solely rely on self-evaluation but should refer to additional clinical information such as scratching for evaluation of pruritus in patients with dementia. Skin care with moisturizer may be important to control itch in patients with dementia.
Key words: itch; elderly; dementia; dry skin.
Accepted Jun 15, 2020; Epub ahead of print Jun 17, 2020
Acta Derm Venereol 2020; 100: adv00210.
Corr: Akihiko Ikoma, Maruho Co., Ltd., 1-5-22, Nakatsu, Kita-ku, Osaka, 531-0071, Japan. E-mail: ikoma_eom@mii.maruho.co.jp
This manuscript is about an epidemiological study on the prevalence of itch in patients with dementia. This study is unique since patients with dementia are usually excluded from the target in studies of this kind. The study results show a high prevalence of itch and suggest that dry skin is an important factor closely linked to itch. The study also reveals the limitation of self-evaluation that is usually used for the assessment of itch and indicates the necessity of evaluations by others or objective methods in patients with dementia.
Itch is common in the elderly and significantly impairs their quality of life. The underlying causes of itch in the elderly are multifactorial and seem linked to skin ageing, immunosenescense, and neurological/psychological changes with ageing (1–3). On the other hand, the number of people with dementia is currently around 50 million globally and is estimated to rapidly increase to 82 million by 2030 and 152 million by 2050 following fast growth in the elderly population (4). According to previous epidemiological studies on itch, the prevalence of itch in the elderly varies in a range from 7.3 to 44%, over 20% in most cases (5–10). None of those studies, however, focused on patients with dementia and rather excluded them since those studies were based on self-evaluation of itch. In the present study, we surveyed the prevalence of itch in elderly Japanese patients with dementia, using multiple methods of evaluation including self-evaluation as well as evaluation done by others such as nurses, family members, and care givers. This is a unique study focusing on the prevalence of itch in patients with dementia.
Study subjects
A total of 185 patients (155 females and 30 males, mean ± standard deviation age 87.6 ± 6.5 years) diagnosed with dementia by physicians were surveyed in the study. Of these patients, 141 of them were living in nursing homes under Benesse Style Care or Saint-Care Holding, and 44 in their own homes receiving home-visit medical care by Takase Clinic. In accordance with the ethics committee approval (OPHAC Hospital No. 977), informed consent was obtained from both of the study subjects and their legally-authorized family members before participation in the study. Only if the study subject was not capable of giving informed consent due to dementia, the informed consent of a legally-authorized family member was considered to represent the study subject. The study was conducted in accordance with the 1964 Helsinki Declaration and its later amendments and registered in Japan under UMIN Clinical Trials Registry UMIN-CTR (Registry No. UMIN000025583). The survey was performed during a 5-month period from January to May.
Questionnaire
In the study, local nurses who regularly saw the study subjects and were well informed of their medical conditions were trained on the study procedure and acted as the investigator’s representatives. The nurses interviewed patients and performed their physical assessment, as well as interviewed families and care givers, using a designated questionnaire (Fig. S1). The questionnaire consisted of 3 major parts; demography, staging of dementia, and itch assessments. The demography part contained sections about age, sex, type of dementia, medical history, and skin care. In regard to the type of dementia, the most suitable type was chosen on the basis of the diagnosis in the health records out of the following list; Alzheimer’s disease (AD), vascular dementia (VaD), dementia with Lewy bodies (DLB), frontotemporal dementia (FTD), mixed, others, and unknown. The medical history section included a check list focusing on multiple specific cutaneous (xerosis, atopic dermatitis, psoriasis, and chronic urticaria) and non-cutaneous diseases (liver dysfunction, and renal failure with dialysis) that often cause chronic itch. Other comorbidities were also recorded. In the skin-care section, the nurses obtained information from health records or interviewed families and care givers about how often skin care with moisturizer was applied and the most appropriate answer was chosen from the following list of 5 choices; daily or almost daily, less than daily but 3 or more times a week, occasionally or less than 3 times a week, no skin care, and unknown. In the dementia-staging part, the nurses evaluated the clinical staging of dementia based on the three-grade classification (mild, moderate, and severe) suggested by the Alzheimer’s Association for staging Alzheimer’s disease (11). The itch-evaluation part consisted of 4 sections on itch severity, scratching behavior, scratching marks and dry skin. In the itch-severity section, patients were asked by two steps; first asked whether or not they were at present suffering from itch, and, only if the answer was ‘Yes’, second asked to rate its severity using a 0–10 numerical rating scale (NRS) (0: no itch, 10: worst imaginable itch). The second step was not done if patients answered ‘No’ or were not capable of answering the question in the first step. In the scratching-behavior section, family members or care givers who most often see the patient during day and night were asked to rate the scratching behavior in mean during the latest 3 days using a 0–10 NRS (0; no scratching observed, 10; vigorously scratching almost all time). In the scratching-mark section, the nurses looked at the whole body surface of patients and rated the body surface area (BSA) associated with scratching marks using a NRS (0; no scratching marks, 1: 1–9% BSA with scratching marks, 2; 10–29% BSA with scratching marks, 3; 30–49% BSA with scratching marks, 4: 50% or more BSA with scratching marks). Finally, in the dry skin section, the nurses assessed the severity of dry skin on the driest part of the body using a 0–4 NRS according to the guidance of European Group on Efficacy Measurement of Cosmetics and other Topical Products (EEMCO) (0; absent, 1; faint scaling, faint roughness, and dull appearance, 2; small scales in combination with a few larger scales, slight roughness, and whitish appearance, 3; small and larger scales uniformly distributed, definite roughness, possibly slight redness, and possibly a few superficial cracks, 4; dominated by large scales, advanced roughness, redness present, eczematous changes, and cracks) (12).
Statistical analysis
The prevalence of itch was calculated as the percentage of subjects who answered ‘Yes’ to the question of whether or not she/he was suffering from itch. For evaluation of scratching behavior by family members or care givers and scratching marks by the nurses, scratching was considered to be negative only if both of scratching behavior and scratching marks were rated 0, whereas positive if otherwise, i.e. if either scratching behavior or marks or both were rated 1 or higher. The severity distribution of self-evaluated itch, scratching behavior, scratching marks and dry skin was descriptively summarized by the frequency and percentage. The correlations of the above severities with dementia staging and skin care frequency as well as the inter-severity correlations were estimated using the Spearman correlation. Correlations of comorbidities with scratching behavior/marks and dry skin were estimated using the Wilcoxon rank-sum test. A statistical significance level of 0.05 was used.
Demography and background
The severity of dementia based on a 3-stage scale for Alzheimer’s disease was mild in 42 patients, moderate in 92 patients, severe in 51 patients and unknown in one patient. The major type of dementia was Alzheimer’s disease (122 patients) followed by vascular type (25 patients), unknown (17 patients), dementia with Lewy bodies (DLB) (10 patients), mixed type (7 patients), frontotemporal dementia (FTD) (2 patients) and others (2 patients). Frequent cutaneous and non-cutaneous comorbidities reported by 4 or more patients were xerosis (65 patients), tinea pedis (8 patients), eczema/dermatitis (non-atopic) (8 patients), pressure sores (4 patients), hypertension (25 patients), hyperlipidemia (12 patients), bone fractures (10 patients), renal failure (8 patients including 1 dialysis patient), cardiac failure (8 patients), diabetes mellitus (7 patients), osteoporosis (6 patients), constipation (6 patients), cerebral infarction (6 patients), pneumonia (5 patients), insomnia (4 patients) and liver dysfunction (4 patients). The major frequency of skin moisturizing care was ‘daily or almost daily’ (63 patients) followed by ‘less than daily but at least 3 times per week’ (51 patients) and ‘occasionally or less than 3 times per week’ (37 patients). There were 33 patients without skin moisturizing care and 1 patient with unknown frequency. The purpose of skin moisturizing care was ‘cure only’ or ‘cure and prevention’ of dry skin in 50 patients (79.4%) and ‘prevention only’ of dry skin in 12 patients (19.0%) out of the 63 patients receiving care ‘daily or almost daily care’. On the other hand, it was ‘cure only’ or ‘cure and prevention’ in 33.3% and 29.7% and ‘prevention only’ in 66.7% and 67.6%, respectively, out of the 51 patients receiving care ‘less than daily but at least 3 times per week’ and the 37 patients receiving care ‘occasionally or less than 3 times per week’.
Self-evaluation of itch
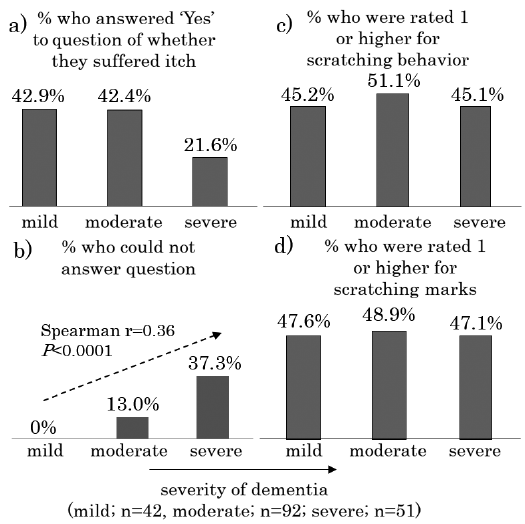
To the question of whether they were suffering from itch, 68 patients (36.8%) (18 with mild dementia, 39 with moderate dementia, 11 with severe dementia) answered ‘Yes’, whereas 86 patients (46.5%) (24 with mild dementia, 41 with moderate dementia, 21 with severe dementia) answered ‘No’. 31 patients (16.8%) (0 with mild dementia, 12 with moderate dementia, 19 with severe dementia) were not able to answer the question. There was no significant statistical correlation between dementia staging and the percentage of patients who answered ‘Yes’ (42.9% with mild dementia, 42.4% with moderate dementia, 21.6% with severe dementia). On the other hand, there was a significant correlation between dementia staging and the percentage of patients who were not able to answer the question (0.0% with mild dementia, 13.0% with moderate dementia, 37.3% with severe dementia, Spearman r = 0.36, p < 0.0001) (Fig. 1). Out of the 68 patients who answered ‘Yes’, 54 patients rated their itch severity, the mean of which was 3.5 ± 2.4 on a 0–10 NRS, whereas 14 patients (2 with mild dementia, 7 with moderate dementia, 5 with severe dementia) were not able to rate it.
Fig. 1. Percentage out of all subjects in each severity of dementia (42 patients with mild dementia, 92 patients with moderate dementia, 51 patients with severe dementia) a) who answered ‘Yes’ to the question whether they were suffering from itch, b) who could not answer the question, c) who were rated 1 or higher for scratching behavior, and d) who were rated 1 or higher for scratching marks. Correlation analysis with the Spearman’s rank correlation coefficient.
Evaluation of scratching behavior and scratching marks
Family members or care givers rated 0 (i.e., no scratching observed) for scratching behavior of 96 patients (23 with mild dementia, 45 with moderate dementia, 28 with severe dementia), whereas they rated 1 or higher for the rest of the patients, i.e., 89 patients (19 with mild dementia, 47 with moderate dementia, 23 with severe dementia). There was no significant statistical correlation between dementia staging and the percentage of patients who were rated 1 or higher for their scratching behavior (45.2% with mild dementia, 51.1% with moderate dementia, 45.1% with severe dementia) (Fig. 1).
The nurses rated 0 (i.e., no scratching marks) for scratching marks on the whole body surface of 96 patients (22 with mild dementia, 47 with moderate dementia, 27 with severe dementia), whereas they rated 1 or higher for the rest of the patients, i.e., 89 patients (20 with mild dementia, 45 with moderate dementia, 24 with severe dementia). There was no significant correlation between dementia staging and the percentage of patients who were rated 1 or higher for their scratching marks (47.6% with mild dementia, 48.9% with moderate dementia, 47.1% with severe dementia) (Fig. 1).
Eighty-six patients (46.5%) were rated 0 for both of scratching behavior and scratching marks (negative scratching), whereas the rest, i.e., 99 patients (53.5%), were rated 1 or higher for either scratching behavior or scratching marks or for both of them (positive scratching). Out of the 68 patients who answered ‘Yes’ to the question of whether or not they were suffering from itch, scratching was positive in 55 patients and negative in 13 patients. Likewise, out of the 86 patients who answered ‘No’, scratching was positive in 27 patients (31.4%) and negative in 59 patients. Out of the 31 patients who were not able to answer the question, scratching was positive in 17 patients and negative in 14 patients (Fig. 2).
Fig. 2. Itch evaluation: self-evaluation versus evaluation done by others.
In the 54 patients who answered ‘Yes’ to the question of whether they were suffering from itch and were able to thereafter rate the severity of itch, there was a statistically-significant positive correlation between self-evaluated ratings of itch and ratings of scratching behavior evaluated by family members or care givers (Spearman r = 0.76, p < 0.0001), and also between self-evaluated ratings of itch and ratings of scratching marks evaluated by nurses (Spearman r = 0.66, p < 0.0001). Additionally, there was a statistically-significant positive correlation between ratings of scratching behavior and ratings of scratching marks (n = 185, Spearman r = 0.83, p < 0.0001) (Fig. 3).
Fig. 3. Correlation of self-evaluated ratings of itch to a) scratching behavior and b) scratching marks, c) correlation of scratching behavior to scratching marks, and correlation of dry skin to d) scratching behavior and e) scratching marks. Correlation analysis with the Spearman’s rank correlation coefficient.
Evaluation of dry skin
The nurses rated 0 (i.e., absent dry skin) for the dry skin of 48 patients (25.9%) but rated 1 or higher for the rest, i.e., 137 patients (74.1%) (1; 84 patients, 2; 30 patients, 3; 21 patients, 4; 2 patients). There was a statistically-significant positive correlation between the severity of dry skin and the rating of scratching behavior (Spearman r = 0.53, p < 0.0001) and also between the severity of dry skin and the rating of scratching marks (Spearman r = 0.54, p < 0.0001) (Fig. 3). Additionally, there was a statistically-significant but mild positive correlation between the frequency of skin care and the severity of dry skin (Spearman r = 0.37, p < 0.0001) (Fig. 4).
Correlations of comorbidities with scratching behavior/marks and dry skin
The 65 patients who had xerosis as a comorbidity in their medical records had significantly higher ratings of scratching behavior/marks and dry skin as compared to the remaining patients (Wilcoxon rank-sum test, p < 0.0001). There was no other significant correlation of comorbidities with ratings of scratching behavior/marks or dry skin.
Fig. 4. Correlation of the frequency of skin care to the severity of dry skin. Correlation analysis with the Spearman’s rank correlation coefficient.
The present study has shown that 36.8% of the surveyed patients with dementia self-reported the presence of itch, equivalent to the previously-reported prevalence of itch in the elderly (5–10), whereas 53.5% were positive with scratching behavior or/and marks according to evaluation done by others such as nurses, families and care givers. The gap between 36.8% and 53.5% indicates that the prevalence of itch in patients with dementia might be underestimated when only based on self-evaluation. The limitation of self-evaluation in patients with dementia is also supported by the result that, the higher the dementia severity was, the larger percentage of patients could not give answers when asked about their itch. Moreover, out of the patients who denied the presence of itch, 31.4% (27/86) were positive with scratching behavior or/and marks (Fig. 2). This suggests that those patients could not recognize their itch or could not properly understand the question and that the patients’ self-evaluation is not suit-able for the assessment of itch in patients with dementia.
Several limitations must be considered in our study. One significant limitation is the use of non-validated instruments for the evaluation of scratching behavior and scratch marks because no such instruments are avail-able, as far as we know. The questionnaire we used was also not validated. Another limitation when evaluating scratching behavior on the skin in dementia is that skin picking behavior may occur more frequently and may influence evaluating itch and the clinical picture of the skin. Patients with dementia may develop abnormal repetitive behaviors such as skin picking (13, 14). Repetitive behaviors in patients with dementia are more frequently related to frontotemporal dementia as compared to other types of dementia including Alzheimer’s disease and have been reported to be rather repetitive impulsions mediated by brain dysfunction than compulsions as in obsessive-compulsive disorders (15). It is hard to differentiate skin picking from itch-induced scratching when only observing behaviors or the surface of the skin. Also, skin picking and the itch-scratch cycle are potentially mixed, since skin picking may lead to local skin inflammation. Thus, the evaluation of scratching behavior and marks by nurses, family members and care givers in the present study has limitations in the precise differentiation of scratching from skin-picking, although the type of dementia in the present study was Alzheimer’s disease in most cases and rarely frontotemporal dementia.
The prevalence of itch based on scratching behavior and marks was not affected by the dementia severity (Fig. 1c, d), whereas the percentage of patients who self-reported the presence of itch was almost half in patients with severe dementia as compared to those with mild or moderate dementia (Fig. 1a). This discrepancy is perhaps linked to the result that the percentage of patients who could not answer the question was the highest in patients with severe dementia (Fig. 1b).
The prevalence of dry skin, equivalent to the total percentage of patients who were rated 1 or higher for the severity of dry skin by the investigators, was 74.1%, which might have been influenced by the period when the survey was performed, i.e., a time period of the year with a relatively dry climate, but is consistent with the previously-reported prevalence of dry skin or xerosis in the elderly (16–18). The significant correlation of the nurse-evaluated severity of dry skin to scratching behavior and marks indicates that dry skin is an important factor for itch in patients with dementia, as is the case with itch in the general elderly population (1, 3, 6, 19). On the other hand, the positive correlation of skin care frequency to dry skin severity might be linked to the result that ‘cure only’ and ‘cure and prevention’ were the major purpose of skin care in the patients receiving daily skin care, whereas ‘prevention only’ was the major purpose in patients who received skin care less frequently, indicating that skin care was more frequently applied to the patients with more severe dry skin but might have been insufficient to manage dry skin in those patients. Interestingly, ‘xerosis’ is much less frequently recorded as a comorbidity in health records (65 patients, i.e. 35.1%), indicating that dry skin might be overlooked or might not be considered as a disease that needs to be treated unless it is a severe case. Clinical studies with appropriate skin care regimens are needed to prove the true efficacy of moisturizer for improvement of chronic itch in patients with dementia.
In conclusion, the present study was a unique study focusing on the prevalence of itch in patients with dementia, who usually are excluded from the targeted population, and has indicated a high prevalence of itch in those patients. For accurate judgement of the presence of itch and assessment of itch severities in patients with dementia whose capabilities of communication are impaired, one cannot rely on self-evaluation by patients but needs to refer to additional clinical information such as scratching. It would be ideal to add objective information such as nocturnal scratching counts (20).
This study was conducted with the support of nurses at Benesse Style Care, Saint-Care Holding and Takase Clinic who acted as the investigator’s representatives. This study was sponsored by Galderma S.A. and Akihiko Ikoma, Kimitoshi Takemura, Joelle Vaglio, Michel Poncet and Didier LeClercq were employed by Galderma S.A. or its affiliate at the time of the study.


 Click to show fullsize
Click to show fullsize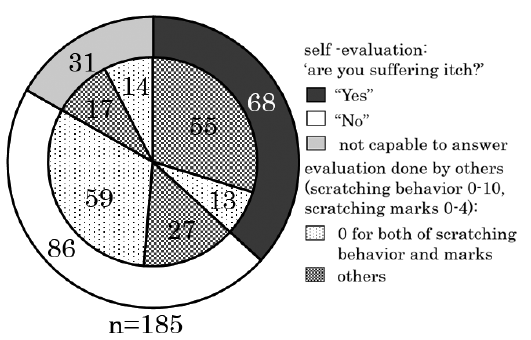 Click to show fullsize
Click to show fullsize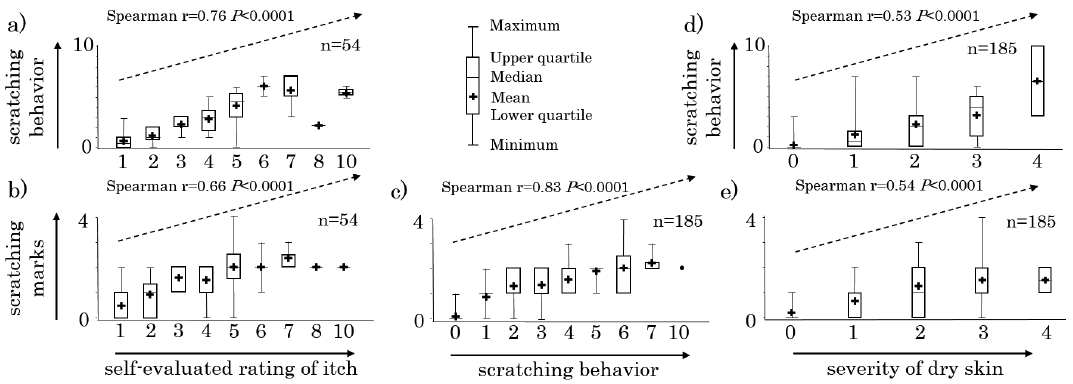 Click to show fullsize
Click to show fullsize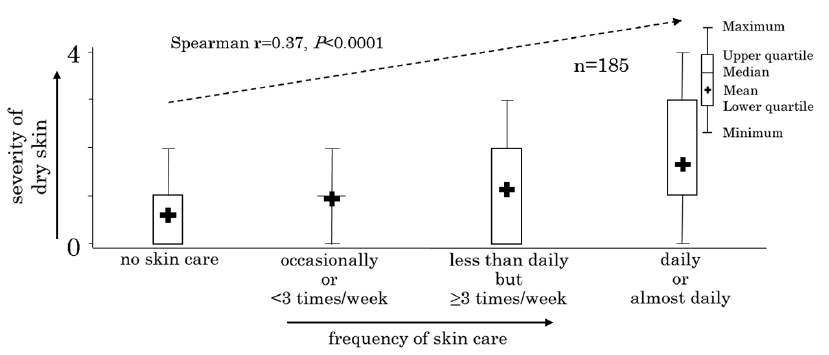 Click to show fullsize
Click to show fullsize