


1Dermatology Department, West Hertfordshire NHS Trust, Hemel Hempstead, UK, 2Dermatology, Department of Experimental, Diagnostic and Specialty Medicine, University of Bologna, via Massarenti 1, IT-40138, Bologna, Italy, and 3Twin Research and Genetic Epidemiology Unit, Kings College London, UK. E-mail: federica.scarfi2@unibo.it.
Accepted Jun 15, 2020; Epub ahead of print Jun 17, 2020
Acta Derm Venereol 2020; 100: adv00211
Hereditary leiomyomatosis and associated renal cell cancer (HLRCC; OMIM 605839) is a rare genetic disorder causing cutaneous and uterine benign smooth muscle tumours with an associated risk of renal malignant tumours. HLRCC is caused by mutations in the fumarate hydratase (FH) gene with an autosomal dominant inheritance. Cutaneous leiomyomas (CLs) are found in most cases with FH germline mutations and present as light brown or purplish papules or nodules. It has been reported that patients with fewer skin lesions are at higher risk of kidney cancer. In 48% of families, CLs number can exceed 100 in at least one member (1).
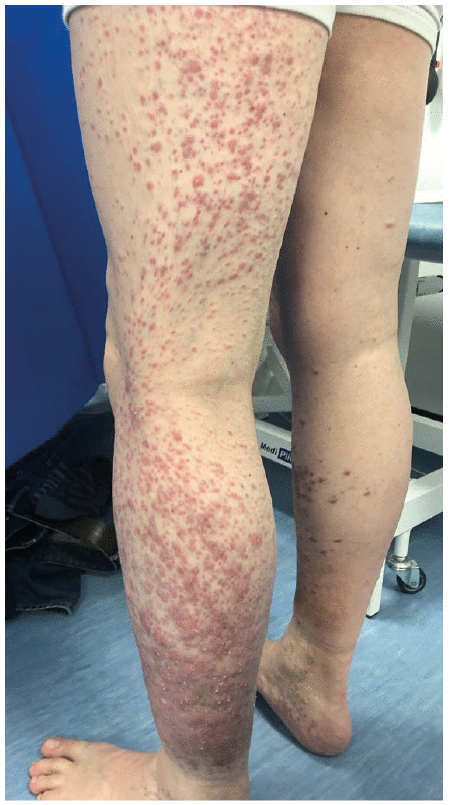
A 46-year-old man presented since the age of 10 with violaceous papules on the lower legs which were proven to be CLs on histology. During his adolescence, the leiomyomas rapidly spread all over the legs reaching up to the thighs. He underwent genetic testing which confirmed the presence of a germline variant of uncertain clinical significance in the FH gene: a heterozygous missense variant c.829A>C, p. (Thr277Pro). His father was found to be carrying the same mutation but presented with a milder phenotype. Due to the associated risk of kidney cancer, both father and son have yearly MRI scans of the abdomen which have been normal.
The patient was re-referred to the dermatology clinic because of increasing pain in both legs. His symptoms were exacerbated when standing or when exposed to cold, making it impossible for him to continue working as a chef. In the past, he was treated with warming the limbs, compression stockings, acetaminophen, codeine, pregabalin amitriptyline and local imiquimod without improvement. Nifedipine has somehow helped the pain. Due to the extent of his condition (Fig. 1), surgery, laser or radiotherapy were deemed unsuitable. Our patient has agreed to be treated with botulinum toxin injections.
Fig. 1. Sheets of leiomyomas on lower legs, reaching up to the thighs.
The FH gene is important for the Krebs cycle and converts fumarate to malate. FH mutations result in a build-up of fumarate. The excess fumarate leads to aberrant regulation of hypoxia-inducible factor (HIF) levels in the cell, causing pseudo-hypoxia and a consequent increased transcription of genes involved in nutrient catabolism, angiogenesis, cell growth and differentiation. FH is believed to act as a tumour suppressor gene. Although allelic loss is the most common alteration, insertion and missense mutations have been described in kidney tumours from patients with germline mutations of FH. Germline bi-allelic FH mutations with loss of FH activity lead to a severe syndrome with brain abnormalities, learning difficulties, seizures and facial deformities (2).
CLs are the most common clinical manifestation which usually develop in early adulthood. They can be divided in subgroups by their clinical and histological aspects: piloleiomyomas, genital leiomyomas and angioleiomyomas. Mosaic presentation may be found as well as a different degree of gene penetrance as found in the family reported here (3).
Leiomyosarcoma transformation is very rare. How-ever, it warrants close follow-up of lesions with biopsies when lesions rapidly increase in size, become ulcerated or are suddenly more painful (4). In 2016, Sommer et al. (5) reported the case of a melanoma and basal cell carcinoma in a patient with HLRCC and they emphasise the need for close skin surveillance and follow-up (5).
The hallmark clinical feature for CLs is pain. The pain can be explained, in part, by the increased presence of nerves and their consequent compression as well as smooth muscle fibres contractions. The pain is usually paroxystic and can be triggered by emotional stress, cold temperatures and pressure. It can be very troublesome, sometimes accompanied by vagal symptoms. It severely affects patient’s quality of life, even leading to attempted suicides (6).
Kidney cancer risk can reach over 20% over a lifetime. However, risk may change depending upon the site of the mutation. The mean age at diagnosis is 44 years and the most common form is the type II papillary renal cell carcinoma (6). The current recommendation for renal cancer screening is a yearly MRI scan. In the 2014 consensus guidelines, genetic testing for FH mutations and renal MRI surveillance are advised. Family members should be screened for renal cancer from the age of 8–10 years onwards (7). Even though over 70 variants have been reported in the FH gene, some families are without known variants. Moreover, there is no clear genotype–phenotype correlations (6). The absence of a germline mutation can be explained by a somatic mutation or mosaicism and can be detected in subsequent screening tests (8). If a mutation is not found, the fumarate enzyme activity can also be measured in different tissues. The loss of FH by immunohistochemistry may have a role in screening, although it has a low sensitivity (9).
Even though our patient has a genetic variant of un-known clinical significance, considering the severity of his cutaneous phenotype, it is very likely to be a pathogenic variant. To our knowledge, this is the first report of heterozygous missense variant c.829A>C, p. (Thr277Pro) in a familial leiomyomatosis family.
Treatment is mostly based on case reports with the principal aim at reducing pain. Triggering of pain with local anaesthesia needs to be taken into consideration as well as a high recurrence rate of up to 50% after surgery (6). Other destructive therapeutic modalities are electrodessication, carbon dioxide laser (10) and liquid nitrogen cryotherapy in single small lesions (11).
Interestingly, the use of botulinum toxin injection has been reported showing an improvement in pain scores and quality of life (12). Intralesional triamcinolone also eased pain and reduces the size of the lesions (13). Topical therapy with capsaicin and topical analgesics has been tried with variable results. Lidocaine patches have shown adequate pain control in one case report (14).
Oral pain killers, including NSAIDs, narcotics and neuroactive medications such as gabapentin, pregabalin and duoxetine have been tried with varied responses. Since the smooth muscle has alpha adrenergic innervation, selective antagonists such as doxazosin have also been used, with dramatic improvement of pain in two cases (15).
Due to the enhanced vascular growth, nitroglycerine has also been used. Lastly, calcium channel blockers such as amlodipine and nifedipine, the latter up to 4 times a day, have also shown good pain control (6).
We maintain the importance of prompt diagnosis in order to initiate renal cancer screening in patients with CLs. Also, we highlight the importance of skin follow-up to rule out malignant tumours but more importantly to control pain and enhancing quality of life.


 Click to show fullsize
Click to show fullsize