


1Department of Dermatology and Medical Research Center Oulu, PEDEGO Research Unit, University of Oulu, Oulu University Hospital, 2Faculty of Medicine, University of Oulu, and 3Infrastructure for Population Studies, Medical Faculty, University of Oulu, Oulu, Finland. *E-mail: kaisa.tasanen@oulu.fi
#These authors contributed equally.
Accepted Jun 16, 2020; Epub ahead of print Jun 18, 2020
Acta Derm Venereol 2020; 100: adv00216.
Hidradenitis suppurativa (HS) is a chronic inflammatory disease characterized by painful, often discharging, lesions of intertriginous areas of the skin. HS is more common in females than males and it occurs most often after puberty (1). HS is associated with several somatic and psychiatric comorbidities (2–4), depression and anxiety being the most common in both adult and adolescents (4, 5). HS is often unrecognized, and patients with HS may not seek medical help. Diagnosis may be delayed for more than a decade (6). The long diagnostic delay makes it impossible to reliably study the temporal relationship of HS and its comorbidities via registry data. Therefore, we performed a retrospective hospital-based study to analyse the effect of disease duration on psychiatric comorbidity.
The Oulu University Hospital (OUH) database was queried to obtain the records of all patients diagnosed with HS at the hospital between 1996 and 2015. Each diagnosis was identified by the presence in the record of International Classification of Diseases, Tenth Revision (ICD-10) code L73.2. All patients with at least one registered L73.2 code were included. The retrieved patient records were reviewed by the authors for demographics, disease duration, smoking status, and pre-selected comorbidities, as well as the diagnosis date of any psychiatric comorbidity. Statistical analyses were conducted using the SAS software package (version 9.4, SAS Institute Inc., Cary, NC, USA). All results are presented as proportions and means. Because the study was based on a retrospective review of records, the agreement of the ethics committee was not required. However, the study methods were approved by the Medical Director of OUH.
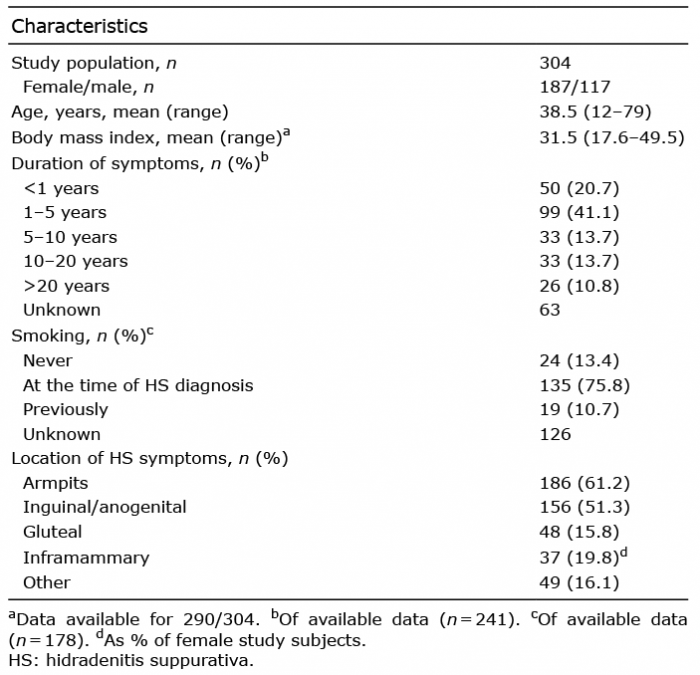
The database search returned the records of 304 patients; 187 females (61.5%) and 117 males (38.5%), mean age 38.5 years (range 12–79 years). At the time of diagnosis over 60% (n = 191) had had symptoms of HS for longer than 1 year. Smoking status was reported for 60.1% (n = 178/304) of cases and of these 75.8% (n = 135/178) were current smokers (Table I).
Table I. Characteristics of the study population
Sixty percent of patients had at least 1 comorbid disease, and over half of these (51.3%) had at least 2 comorbid diseases. All the investigated comorbidities are shown in Fig. 1. The most common comorbidities were cardiovascular diseases (CVD) (35.9%), diabetes (23.0%), obesity (20.4%) and depression (15.5%).
Fig. 1. Comorbid diseases in patients with hidradenitis suppurativa (n = 304) treated in Oulu University Hospital between 1996 and 2015.
Regarding psychiatric comorbidities and their relationship with duration of HS symptoms, those with <1 year of HS symptoms were most likely to have a diagnosis of depression or another psychiatric comorbidity (Table II). Those who had had HS symptoms for longer than 5 years had a lower rate of psychiatric comorbidities. Patients with depression or other psychiatric comorbidities did not differ from those without in terms of age at diagnosis, diagnostic delay or other comorbidities studied.
Table II. Duration of hidradenitis suppurativa (HS) symptoms and psychiatric comorbidity at the time of the HS diagnosis
This study found that 15.5% of patients with HS had a diagnosis of depression. This reflects both our previous findings based on Finnish registry data (4) and similar findings from Israel (3). A diagnosis of at least 1 psychiatric disorder other than depression was also found in 15% of cases. However, the study design prevented us from analysing these diagnoses in detail.
In the current study, depression and other psychiatric comorbidities were most often seen in patients whose HS had been diagnosed recently. The prevalence of depression and other psychiatric comorbidities decreased after onset of HS symptoms. Over the past decade there has been an increase in awareness of HS comorbidities (7). However, this does not entirely explain our findings, because the cut-off date for our study period was 2015. One possible explanation could be that patients who experienced a long diagnostic delay learned to cope with their HS symptoms before diagnosis, and were no longer experiencing any psychiatric consequences by the time of their HS diagnosis.
Most patients in the current study had at least 2 HS comorbidities. Cardiovascular diseases (CVD) and diabetes were the most common comorbidities. CVD were present in approximately 40% of the study population. This is notable because the reported prevalence of CVD in overweight middle-aged Finns is approximately 8%; much lower than that found in our comparatively young population (mean age <40 years) (8). However, more than 1 in 5 of our study subjects was obese. Previously, a large Danish registry-based study found that HS is a remarkable and independent risk factor for cardiovascular diseases (9), and an Israeli study reported that patients with HS have an elevated risk of metabolic syndrome, diabetes, hypertension and hyperlipidaemia (10). In addition, most of the subjects were previous or current smokers; smoking is known to be strongly associated with HS (11).
Although metabolic diseases are the most common comorbidities of HS, psychiatric disorders greatly diminish patients’ quality of life. To further reduce the psychiatric morbidity of HS patients, it is important that dermatologists are aware of the possibility of psychiatric problems when diagnosing HS. This would help to guide patients with HS to seek social support and psychiatric care if needed. These procedures may bolster resilience and coping in patients with HS, which, in turn, may help to prevent mental illness from becoming chronic (12).
A strength of this study is that it includes all patients with HS treated in the OUH over a 19-year period. All medical records of patients included in the study were reviewed carefully and used to verify HS diagnoses. The individual follow-up time varied from less than 1 year to 2 decades, and this can be considered as a limitation of this study. Furthermore, since this study was based on hospital medical records, it was unable to capture diagnoses made in the primary care setting.
Conflicts of interest. HT has received educational grants from Novartis, AbbVie, LEO Pharma, MSD, Galderma Nordic, Pfizer, Meda, Janssen-Cilag and Roche, and honoraria from Abbvie. KT has received educational grants from Novartis and Pfizer and honoraria from Novartis, Abbvie, Janssen-Cilag, SanofiGenzyme and Lilly for consulting and/or speaking. LH has received educational grants from Shire, Janssen-Cilag, Novartis, AbbVie and LeoPharma, honoraria from SanofiGenzyme, Novartis, Abbvie and UCB Pharma for consulting and/or speaking and is an investigator for Abbvie. The other authors have no conflict of interest to declare.


 Click to show fullsize
Click to show fullsize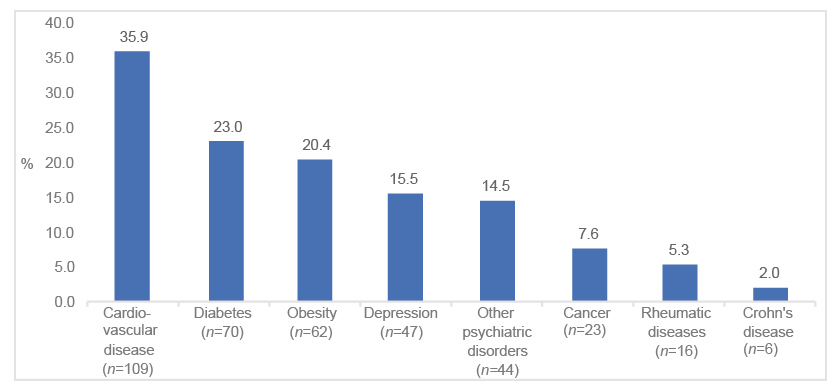 Click to show fullsize
Click to show fullsize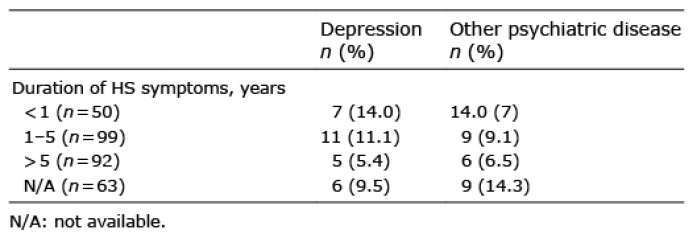 Click to show fullsize
Click to show fullsize