


1Department of Dermatology, University Hospital of Brest, 2 Avenue Foch, FR-29200 Brest, and 2Department of Psychiatry, Hospital of Bohars, Bohars, France. E-mail: charlesdervout@gmail.com
Accepted Jun 16, 2020; Epub ahead of print Jun 18, 2020
Acta Derm Venereol 2020; 100: adv00217.
Delusional infestation is a psychiatric disorder characterized by an aberrant perception of being infested by small organisms (insects, bacteria, worms) or inanimate pathogens (fibres, hairs, particles (1–3)). Hence, it is not restricted to “delusional parasitosis” or Ekbom syndrome, and includes Morgellons disease and other atypical manifestations (4, 5). Delusional infestation is a rare disorder, which is more common in women. The worldwide incidence and prevalence of delusional infestation are unknown. The annual incidence of delusional infestation is estimated at 2.37 per 100,000 person per year, with a prevalence of 17 per million inhabitants per year in Europe (1), whereas Bailey et al. estimated an annual incidence of 1.9 per 100,000 person per year in the USA (6).
All organs can be “infested”, but patients frequently report cutaneous symptoms, such as sensations of crawling, biting or stinging, in the skin or under the skin. Because of the cutaneous complaints, patients with delusional infestation are commonly seen by dermatologists. Physical examination usually shows non-specific signs, such as excoriations, xerosis, lichenification, and sometimes auto-inflected skin damage to “dig out” the suspected pathogens.
Delusional infestation has 2 subtypes: primary delusional infestation, which is a monodelusional disorder with no detectable aetiological condition, and secondary delusional infestation, related to a medical or psychological disorder or drug abuse (1, 7, 8).
Here, we describe 2 patients with a long history of chronic pruritus of undefined aetiology that led to the development of delusional infestation.
Case 1. A 71-year-old woman presented chronic pruritus for 2.5 years that was associated with sensations of stinging and itching of the arms and legs. Three years previously she had undergone chemotherapy with cisplatin for pharynx carcinoma. Physical examination revealed signs of chronic itching, with linear excoriations and cutaneous nodules. The diagnosis of chronic nodular prurigo was proposed. The patient was convinced she was infested with parasites. Thoraco-abdomino-pelvian scan, complete laboratory tests according to the European recommendations (9) and skin biopsy searching for underlying dermatosis or small fibre neuropathy did not show abnormalities. Electromyography confirmed the diagnosis of distal sensitive polyneuropathy secondary to cisplatin. Pregabalin was introduced (100 mg twice daily) and the patient commenced topical corticosteroids. Despite partial resolution of the chronic nodular prurigo symptoms, the delusional infestation was persistent; the patient remaining convinced that she was infested and showing signs of depressive disorder. Pregabalin was discontinued because of insufficient anti-pruritic effect and adverse effects (sleepiness) and switched to duloxetine 30 mg/day. At the same time, the patient started psychotherapy. After a few months of follow-up under duloxetine, the delusional infestation disappeared, with improvement of both the skin condition and depression.
Case 2. A 61-year-old woman presented with chronic pruritus for 10 years; the clinical examination revealed chronic nodular prurigo. The patient also had pernicious anaemia and hypothyroidism: both conditions were being treated and were considered stable. The same medical check-up as for case 1 did not reveal any abnormalities, with the exception of histological examination of skin biopsies (showing low epidermal neurite density, which led to a diagnosis of small-fibre neuropathy) and computed tomography (CT) scan (showing multiple mediastinal adenomegalies, associated with bilateral micronodular peri-lymphatic infiltrates, which suggested a diagnosis of sarcoidosis). Levels of calcium and angiotensin conversion enzyme were normal, and cytological analysis of mediastinal adenomegaly was not able to confirm granuloma. The patient then refused new skin biopsy. The diagnosis of small fibre neuropathy probably secondary to sarcoidosis was proposed. During the different consultations and examinations, the patient started to develop a delusional infestation (Fig. 1). She said she saw filamentous structures under her skin and in faeces and was increasingly invaded by such thoughts. Many samples were taken, but no infection was found, the structures being textile fibres. However, the patient persisted in her delusional infestation.
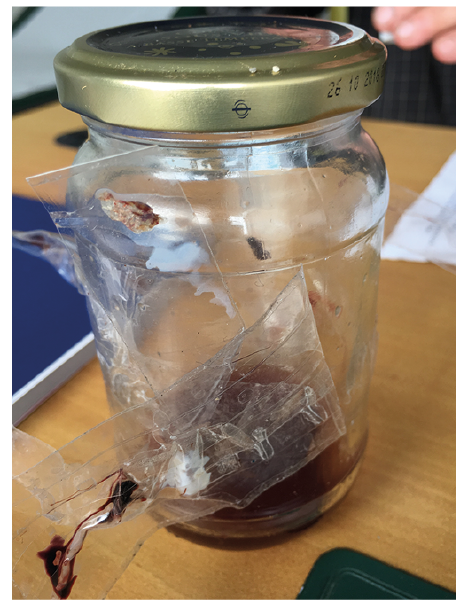
Fig. 1. A sample patient with delusional infestation can present in medical check-up. The jar contains ”evidence” of the infestation, with several pieces of skin scratched off, blood and substances of unknown origin. textile fibres and insects are scotched to the jar.
The pathogenesis of delusional infestation is probably multifactorial (1). Recent progress in brain imaging has provided interesting results for understanding this disorder. Cortical alteration and dopaminergic neurotransmission abnormalities in brain regions involved in body perception (dorsal striatum, thalamus) judgement (frontal cortex) and sensory gating (thalamus) are frequent in patients with delusional infestation (10–12). Explaining the different mechanisms that could induce delusional infestations to the patient might help in prescribing individual psychotherapy and medication.
The treatment of delusional infestation is challenging. Patients generally focus on their skin infestation. Psychiatrist intervention and the prescription of anti-psychotic medications are frequently refused. Management of delusional infestation requires good strategies to develop a therapeutic alliance between the patient and the physician (13). A multidisciplinary approach with dermatological and psychiatric cooperation is essential for treating this condition (14).
In our 2 cases, chronic pruritus was initially the main complaint, and patients were diagnosed with chronic nodular prurigo. Patients frequently have difficulty understanding that repetitive scratching and skin injuries lead to the development of nodules or papules. The long duration of symptoms, especially pruritus, and the lack of diagnosis are possible factors that led to the development of delusional infestation. For both patients, complete check-ups revealed organic causes of their cutaneous symptoms. This knowledge helped alleviate the delusional infestation for the first patient, but it is too early to provide data for the second patient.
Case 1 is a good example of a multidisciplinary approach, treating at the same time the chronic nodular prurigo and depression, thereby leading to complete resolution of the delusional infestation. For case 2, the delusional infestation developed during the diagnostic phase. Despite the diagnosis of sarcoidosis and small-fibre neuropathy, the patient refused the diagnosis and therapeutic proposals.
In conclusion, these 2 cases of delusional infestation secondary to chronic nodular prurigo with an underlying neuropathy show the importance of managing chronic pruritus in terms of diagnosis and therapeutics. Multidisciplinary management is necessary to propose a global approach to this condition. Dermatologists should keep in mind that patients with delusional infestation may have underlying somatic conditions (15) that need to be elucidated.


 Click to show fullsize
Click to show fullsize