


1Department of Dermatology, Venereology and Allergology, Wroclaw Medical University, Wroclaw, Poland, and 2Department of Dermatology, School of Medicine, Cardiff University, Cardiff, UK
Chronic diseases not only have a direct influence on patients’ quality of life, but can also affect the life of family members. The aim of this study was to create the Polish language version of a questionnaire estimating impact of disease on quality of family life: the Family Reported Outcome Measure – 16 (FROM-16). A standard forward and backward translation procedure was used to convert the original English version of FROM-16 into the Polish language. Creation of the Polish version was performed in a group of 30 patients’ family members. The Polish language version of FROM-16 showed very good internal consistency reliability, the Cronbach α coefficient was 0.89. Reproducibility level was established with an intraclass correlation coefficient of 0.98. The Polish language version of FROM-16 can potentially be used as a tool to assess quality of life of patients’ family members.
Key words: Family Reported Outcome Measure; quality of life; validation; questionnaire.
Accepted Jun 23, 2020; Epub ahead of print Jul 3, 2020
Acta Derm Venereol 2020; 100: adv00219.
Corr: Jacek C. Szepietowski, Department of Dermatology, Venereology and Allergology, Wroc?aw Medical University, Cha?ubi?skiego 1, PL-50-368 Wroc?aw, Poland. E-mail: jacek.szepietowski@umed.wroc.pl
There is a high negative impact of a patients’ disease on the quality of life of family members. The Family Reported Outcome Measure – 16 (FROM-16) was originally created in English. The questionnaire enables assessment of relevant quality of life aspects of the family members of patients with various medical conditions. This study aimed to create the Polish version of FROM-16. The results demonstrated high internal consistency and reproducibility of the instrument, therefore warranting its further use in families of Polish patients.
Over the last 20 years, there has been an increasing interest in quality of life (QoL) in clinical practice. Assessment of the impact of QoL has become important in routine clinical decision-taking, influencing the selection of treatment and assessment of its effectiveness. It has been demonstrated that individuals’ QoL can also influence the QoL of those around them, including partners or parents (1, 2). The negative impact of a patient’s disease on their family members has been established in relation to emotional state and physical, social and financial aspects (1, 3).
Several instruments have been developed to assess the influence of chronic illness on the lives of families of patients; however these are mostly disease- or speciality-specific (1, 4). The Family Reported Outcome Measure (FROM-16) is a unique measure created by Golics et al. (5) from Cardiff University, Cardiff, UK, published in 2014. The questionnaire, containing 16 items, is designed to establish the impact on QoL of an adult family member or partner resulting from having a person (of any age) in a family with any disease or condition. Notably, FROM-16 enables direct comparison of the impact of QoL between family members of patients with different medical conditions. The questionnaire is self-explanatory and can be implemented simply in routine practice, taking, on average, only 2 min to complete (5).
As the original instrument was created in English, the aim of the current study was to prepare the Polish language version of FROM-16 in family members of patients with chronic disease. This will enable the use of FROM-16 in future routine clinical practice and research in people speaking Polish.
The Polish language version of the FROM-16 questionnaire was prepared in conformity with international standards (6). Permission to translate FROM-16 into Polish was given by the copyright holders of the instrument.
Translation and creation process
First, the original English version of FROM-16 was translated into Polish by 2 independent translators. The resulting versions were compared in terms of existing discrepancies by a third consultant, a bilingual expert in the field, and a unified version was reached by consensus. In the next stage reverse translation from Polish to English was performed by another independent translator who was not familiar with the original version of the FROM-16 questionnaire. The back translation was sent to a member of the team who created the original version for their comments. Minor corrections were made in translation in accordance with their recommendations. As a result, a final Polish version of FROM-16 was derived.
Subsequently, cognitive debriefing procedure was conducted. To assess the level of comprehensibility of the translation it was tested on a group of 8 parents. All interviewees were women aged 35–48 years who looked after children with various conditions (1 child with urticaria, 1 with psoriasis, and 6 with type I diabetes mellitus). The time required to complete the questionnaire was measured and then questions were asked regarding intelligibility and wording of both questions and answers. All doubts or suggestions from the respondents were noted and a report was prepared based on the information collected. After reading the report, the authors of the original version of the questionnaire expressed official consent to use the Polish language version of FROM-16.
A further step was carried out in a group of 30 family members of endocrinology, oncology and dermatology patients. Among those, there were 9 patients with type I diabetes mellitus, 8 with growth disorders (mainly growth retardation), 4 with malignancies (2 with lung cancer, 1 with thyroid cancer and 1 with prostate cancer), 6 with psoriasis vulgaris, 2 with atopic dermatitis, and 1 with pemphigus vulgaris. All participants were asked to complete the questionnaire twice with an interval of 3 days. The interval was considered sufficient to prevent patients from recalling their previous answers, but not to allow for any significant changes in disease severity or the family situation.
Statistical analysis
Statistical analysis of the results obtained was carried out to assess the reliability of the questionnaires using the Statistica 13 (Dell, Inc., Tulsa, OK, USA) software. Internal consistency of the questionnaire was evaluated with Cronbach’s α coefficient and by determining the correlation coefficients between the responses to individual questions and total score. It is generally assumed that the internal consistency is good if the Cronbach’s α coefficient is a minimum of 0.7 (7). The questionnaire reproducibility (test–retest reliability) was evaluated by comparison of the responses of 2 administrations of the questionnaire by the same person, using the intraclass correlation coefficient (ICC). It is assumed that the ICC should be at least 0.7 (8). The entire statistical analysis was carried out at the confidence level α = 0.05. p < 0.05 was considered statistically significant.
The time needed to complete the Polish language version of the questionnaire varied between 3 and 7 min (mean 4.5 ± 1.5 min). None of the respondents reported any problems concerning understanding the questions or instrument categories. Moreover, they did not submit any suggestions on changing the wording of questions. Based on the above information, the intelligibility and wording of each question was assessed as satisfactory.
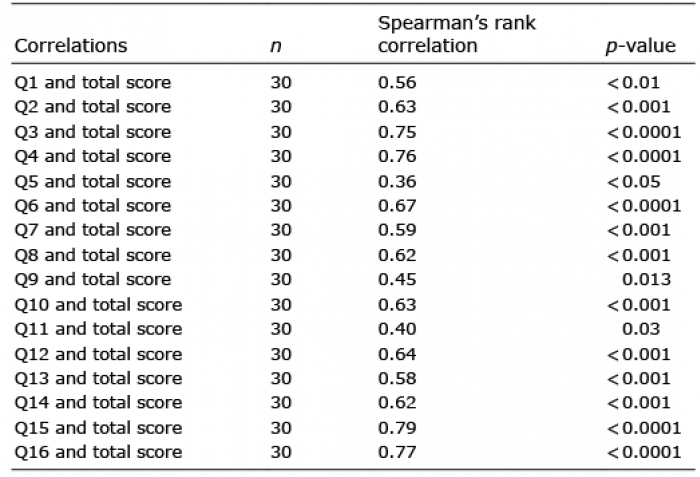
Assessment of internal consistency of the Polish language version of FROM-16 demonstrated that the different items of the questionnaire interrelated with one another. Cronbach’s α coefficient for the whole scale was high and amounted to 0.89 (95% confidence interval (95% CI) 0.82–0.94), which indicates very good internal consistency of the questionnaire. Similarly, Cronbach’s α both domains (i.e. Emotional and Personal & Social Life) was also high (0.82 (95% CI 0.7–0.9) and 0.87 (95% CI 0.79–0.93), respectively). Significant correlations were found between the results obtained for each item and the total score of the questionnaire (Table I).
Table I. Correlation of each item (Q) score with total score of the Family Reported Outcome Measure – 16 (FROM-16)
The reproducibility of FROM-16 was determined using an ICC coefficient and assessed as 0.98 for the whole FROM-16. The ICC between scores obtained during the first and second questionnaire completion were 0.92 for the Emotional domain and 0.97 for the Personal & Social Life part of FROM-16. In addition, no statistically significant differences were found between the total score obtained after completing the questionnaire twice (on day 0 and day 3) (Table II). Correlation coefficients between the answers to individual questions obtained during the first and second survey completion were also determined. Statistically significant, positive correlations were found between the results obtained for each question when completing the questionnaire twice (detailed data not shown).
The Polish language version of FROM-16 is available from Cardiff University website (https://www.cardiff.ac.uk/medicine/resources/quality-of-life-questionnaires/family-reported-outcome-measure).
Table II. Reproducibility of results
The negative impact of many diseases is not limited to the patients, but may extend to those around them. However, this burden is often unrecognized or underestimated. Family members play a crucial role in the care of patients, yet they may not acquire the level of psychosocial support that they truly need (2–4). The FROM-16 questionnaire can be completed by every adult who has a family member or partner with any health condition or disease. The questionnaire has the potential to be used in a variety of clinical situations, clinical research and education programmes for families of patients.
This study describes the development of the Polish language version of FROM-16. The analysis of internal consistency was carried out on the basis of correctly completed questionnaires on the first day of the study. Statistically significant, positive correlation between the results obtained for each question separately and the total number of points was established. The results regarding internal consistency were very good, the value of Cronbach’s α (0.89) was similar to that of the original version (0.91) (5). Based on responses of 2 administrations of the questionnaire with an interval of 3 days, a questionnaire reliability analysis was made. The level of reproducibility was determined using the ICC coefficient, which was 0.98. No statistically significant differences were found between the total score and the score for individual questions obtained after completing the questionnaire twice.
The authors of similar projects, in which various dermatological questionnaires were validated, obtained comparable results. Chantarasap et al. (9) validated the Thai version of the FROM-16 questionnaire. In their study of Thai cancer patients’ family members, determining internal consistency of the scale, they documented a Cronbach’s α coefficient of 0.86. Similarly, Marciniak et al. (10) obtained a Cronbach’s α coefficient of 0.84 in the validation process of the Polish language version of the Family Dermatology Life Quality Index (FDLQI). In another validation process, of the Polish language version of the Dermatology Life Quality Index (DLQI), conducted by Szepietowski et al. (11), very good internal consistency of the scale was obtained, with a Cronbach’s α coefficient of 0.9. In addition, Hrehorów et al. (12) and Dimitrov et al. (13), also developed and validated both Polish and Arabic language versions of questionnaires for assessing stigmatization in patients with psoriasis, using a 6-item stigmatization scale and a 33-item instrument (Feelings of Stigmatization Questionnaire), obtaining similar results. The Cronbach’s coefficient α values for the Polish adaptations were 0.84 and 0.86, respectively, and for the Arabic adaptations 0.89 for both instruments.
Study limitations
This study has some limitations. It aimed to create a Polish language version of FROM-16 instrument; for this purpose, reliability and reproducibility assessments were performed. However, further validation process on a larger population with convergent validity might be requested.
Conclusion
The newly developed Polish version of FROM-16 has shown high internal consistency and good reproducibility. Therefore, it can be used effectively to study the impact of a disease on the QoL of family members. We encourage its further utilization in the future, not only by healthcare professionals, but also by social science researchers, and as an outcome measure in pharmaceutical company research.


 Click to show fullsize
Click to show fullsize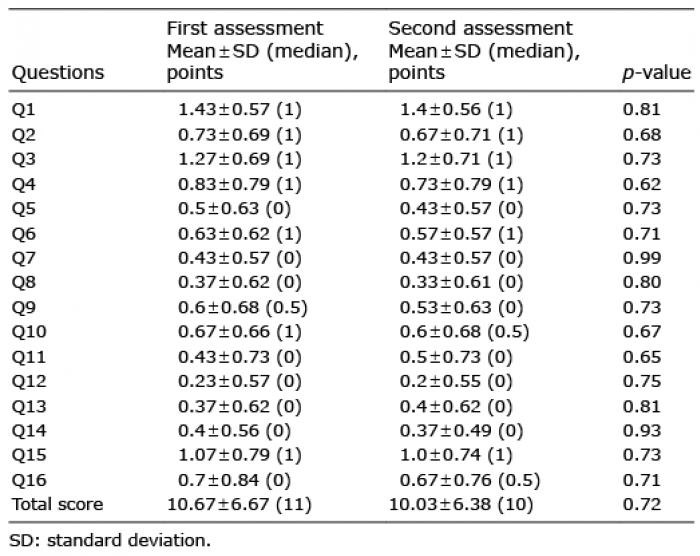 Click to show fullsize
Click to show fullsize