


1Department of Dermatology, Venerology and Allergology, University Medical Center, Ruprecht-Karls-University Heidelberg, Heidelberg, Germany, 2Department of Dermatology, University Hospital of the Paracelsus Medical University Salzburg, Salzburg, Austria, 3MH-Statistical Consulting, Marburg, and 4Dermatopathology, Bodensee, Friedrichshafen, Germany
This study analysed the expression of vascular endothelial growth factor-A (VEGF), VEGFR-2, and VEGFR-3 in primary cutaneous melanomas with positive and negative sentinel node status (SLN) (a total of 58 specimens divided into 2 groups of 29 for each status). The specimens were collected from the pathological archive of the department of Dermatology, Venereology and Allergology of the University Medical Center Heidelberg. A quantification score was developed for protein expression, by considering the percentage of positive melanoma cells (0: 0%, 1: up to 1%, 2: 2–10%, 3: 11–50%, and 4: > 50%) in relation to the intensity of staining (0: negative, 1: low, 2: medium, 3: strong). Tumoural VEGFR-3 expression (mean ± standard deviation) in SLN+ tumours (9.62 ± 3.09) was significantly stronger than in SLN– tumours (6.13 ± 3.87; p < 0.001). A binary logistic regression model proved VEGFR-3 expression and tumour thickness to be significant independent predictors of SLN. These data provide evidence that VEGFR-3 expression may play a critical role in the pathogenesis of malignant melanoma and that its investigation may help to improve the selection of patients with primary cutaneous melanoma for sentinel node biopsy.
Key words: melanoma; sentinel node biopsy; angiogenesis; VEGF; VEGFR-2; VEGFR-3.
Accepted Jun 25, 2020; Epub ahead of print Jul 3, 2020
Acta Derm Venereol 2020; 100: adv00235.
Corr: Ferdinand Toberer, Department of Dermatology, Venerology and Allergology, University Medical Center, Ruprecht-Karls-University, Im Neuenheimer Feld 440, DE-69120 Heidelberg, Germany. E-mail: ferdinand.toberer@med.uni-heidelberg.de
The aim of this study was to analyse the expression of proteins that contribute to angiogenesis in primary cutaneous melanoma. Expression of vascular endothelial growth factor-A (VEGF), VEGFR-2, and VEGFR-3 were investigated by immunohistochemistry in a matched cohort of primary cutaneous melanomas with positive and negative sentinel lymph node status (SLN). The results reveal differences in the expression of VEGF and VEGFR-3 in tumours with positive and negative SLN, and that expression of VEGFR-3 is an independent predictor of SLN. Further studies are needed to confirm these results and show whether they may have therapeutic implications.
Cutaneous melanoma (CM) represents the most aggressive and potentially lethal form of skin cancer. Although its incidence accounts for only 5% of all malignant cutaneous tumours, it is responsible for more than 71% of skin cancer-related deaths annually (1).
Sentinel lymph node biopsy (SLNB) is routinely used to determine the status of the regional lymph nodes in patients with clinically node-negative CM. Current guidelines typically recommend SLNB for patients with T2 (>1?2 mm) and T3 (>2?4 mm) melanoma with no clinically apparent lymph node metastases. However, some guidelines recommend that SLNB is also discussed with T1b patients (tumour thickness ≤0.8 mm with ulceration or 0.8?1.0 mm irrespective of ulceration) with most institutions also performing SLNB in T4 (>4 mm) melanomas (2, 3).
The role of SLNB is expanding from that of a prognostic marker to that of a staging tool, and influences access to adjuvant therapy. The increasing avail-ability of effective adjuvant therapies (targeted therapy and immunotherapy) for patients with positive sentinel lymph node status (SLN) supports the argument for extending the use of SLNB, so that more patients can benefit from adjuvant therapies (4).
However, only 20% of all SLNBs in patients with CM worldwide reveal metastases, with wide variations between melanomas with low and high tumour thickness (5, 6). This means that up to 5 surgical SLNBs are needed to detect one case with nodal involvement (7). As SLNB is an invasive procedure that may trigger complications, such as seroma, wound infections, pain, lymphedema, or sensory defects, the decision to perform SLNB should be based on weighing the likelihood of detecting metastases against the potential complications and costs of the procedure (8–12).
A recent study involving 12,918 patients with melanoma who were undergoing SLNB revealed that tumour thickness, younger age, lymphovascular invasion, mitotic rate, axial location and Clark level were independent risk indicators for sentinel node metastases (2).
Despite these findings, the current practice of selecting melanoma patients for SLNB is far from optimal, as 75?80% of the biopsied individuals do not show lymph node involvement (13). Therefore, the aim of the current study was to analyse whether markers of angiogenesis could serve as a surrogate marker and aid in the prediction of SLN, which may ultimately improve preoperative selection of patients for SLNB.
To the best of our knowledge, this is the first immunohistochemical study to analyse vascular endothelial growth factor-A (referred to as VEGF throughout this paper) and the receptors VEGFR-2 (KDR) and VEGFR-3 (FLT4) in a matched study population of sentinel node positive and negative primary CM.
Specimens
A total of 58 paraffin-embedded primary CM specimens (29 SLN+ ; 29 SLN– ) were collected from the the pathological archive of the department of Dermatology,Venerology and Allergology of the University Medical Center Heidelberg and were analysed using immunohistochemistry. The 2 groups were matched with regard to clinical (age, sex) and histological features (histological type, ulceration).
Immunohistochemistry
The following primary antibodies were used for immunohistochemistry (antibody: clone, source, company, dilution, and antigen retrieval): VEGF: EP1176Y, rabbit, Zytomed Systems, Berlin, Germany, 1:200, pH 9.0; VEGFR-2: 55B11, rabbit, Cell Signaling, Frankfurt, Germany, 1:500, pH 9.0; VEGFR-3: KLT9, mouse, Leica, Nußloch, Germany, 1:10, pH 9.0. To evaluate the expression of VEGF, VEGFR-2, and VEGFR-3 in the CM specimens, a quantification score (QS) was calculated by multiplying the relative proportion of positive melanoma cells (levels of positivity: 0: 0%, 1: up to 1%, 2: 2–10%, 3: 11–50%, and 4: >50%) with the value of the staining intensity (level of intensity: 0: negative, 1: low, 2: medium, and 3: strong). Single products were added to obtain a summed score if multiple intensity ranks were observed in a single specimen. “Blinded” analysis was performed on the specimens by 2 independent dermatopathologists (FT and WH) without knowledge of SLN, tumour thickness, section number or any other clinical data. All cases in which different scores were calculated were discussed in a consensus panel to obtain a single final score. In addition, epidermal VEGF expression was evaluated by measuring the staining intensity (level of intensity: 0: negative, 1: low, 2: medium, and 3: strong) of VEGF in epidermal keratinocytes.
Statistical methods
Statistical analysis was performed using SPSS statistical package (v24.0, SPSS Inc., Chicago, IL, USA). Group differences in expression of the different proteins were tested using the Mann–Whitney U test. In order to illustrate the distribution of expression of the different proteins in SLN+ and SLN– cases, the data are presented as box plots with medians, interquartile ranges, and ranges. Spearman’s rank correlation coefficients were calculated to explore the correlation between the different protein expression scores and the clinical (age, sex) and histological (tumour thickness, ulceration, histotype, regression, and lymphovascular invasion) data. In addition, SLN was modelled in a stepwise binary logistic regression with potential predictors, such as age, sex, ulceration, tumour thickness, tumoural VEGF expression, epidermal VEGF expression, VEGFR-2, and VEGFR-3 expression. p-values < 0.05 were considered statistically significant.
Clinical data
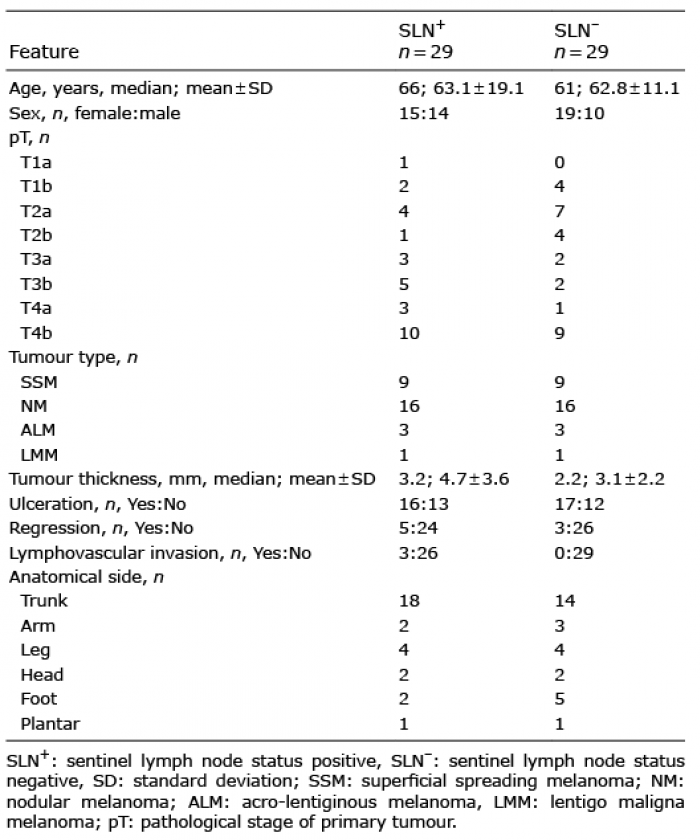
The mean ± standard deviation (SD) age of SLN+ patients (female/male: 15/14) was 63.1 ± 15.9 years (range 33–88 years) and that of SLN– patients (female/male: 19/10) was 62.8 ± 11.1 years (range 47–82 years). Additional clinical and histological data are summarized in Table I.
Table I. Clinical and histological data
VEGF expression
Epidermal VEGF expression was found in all analysed tumours and was rated strong (score 3) in 95% of the CM cases investigated. The epidermis directly above the tumour tended to show higher expression of VEGF than the epidermis at the periphery of the tumour (Fig. 1a–c, e). There was no significant difference in epidermal expression of VEGF between SLN+ and SLN– tumours (p = 0.237) (Fig. 2).
Tumoural VEGF expression was observed in 55/58 (95%) cases of CM. Expression of tumoural VEGF (Mann?Whitney U test) was significantly stronger in SLN+ (9.03 ± 3.06; mean ± SD) than SLN– cases (5.75 ± 4.02; p < 0.001) (Fig. 2).
Fig. 1. Vascular endothelial growth factor-A (VEGF), VEGFR-2, and VEGFR-3 expression in different primary cutaneous melanomas. (a–c) Nodular melanoma showing strong VEGF expression by a subset of tumour cells and in the epidermis overlying the melanoma (a) Haematoxylin-eosin staining (H&E), original magnification ×25, (b, c) VEGF staining, original magnification ×25 and ×50. (d–f) Superficial spreading melanoma showing strong VEGF expression in the epithelium and by approximately 50% of the tumour cells, but no VEGFR-2 expression; (d) H&E, original magnification ×50, (e) VEGF staining, original magnification ×50, (f) VEGFR-2 staining, original magnification ×50. (g, h) Nodular melanoma showing strong VEGFR-3 expression; (g) H&E, original magnification ×25, (h) VEGFR-3 staining, original magnification ×50.
Fig. 2. Expression scores of vascular endothelial growth factor-A (VEGF), VEGF epidermal, VEGFR-2, VEGFR-3 in sentinel node status positive (SLN+) and negative (SLN–) primary cutaneous melanoma. ***p < 0.001.
VEGFR-2 expression
VEGFR-2 expression was observed in 19/58 CM cases (33%) (superficial spreading melanoma 3/19 (16%), nodular melanoma 15/19 (79%), acro-lentiginous melanoma 1/19 (5%), lentigo maligna melanoma 0/19 (0%)). Fig. 1f shows a melanoma lacking VEGFR-2 expression. VEGFR-2 expression in SLN+ tumours (1.62 ± 3.23; mean ± SD) was not significantly different from that in SLN– tumours (1.44 ± 2.21; p = 0.199; Mann?Whitney U test) (Fig. 2).
VEGFR-3 expression
VEGFR-3 expression was observed in 54/58 CM samples (93%). Fig. 1h shows a melanoma with strong VEGFR-3 expression. VEGFR-3 expression in SLN+ tumours (9.62 ± 3.09; mean ± SD) was significantly higher than in SLN– tumours (6.13 ± 3.87; p < 0.001; Mann?Whitney U test) (Fig. 2).
VEGFR-2 and VEGFR-3 expression without subgroup stratification
VEGFR-2 expression (1.53 ± 2.74; mean ± SD) was significantly lower than VEGFR-3 expression (7.87 ± 3.89, p < 0.0005; Wilcoxon test), when comparing tumours, irrespective of SLN.
Clinical and histological data
There was no statistically significant difference in age between SLN+ (63.1 ± 15.9; mean ± SD) and SLN– tumours (62.8 ± 11.1; p = 0.924; 2-sided t-test). Furthermore, sex was not significantly correlated with SLN (p = 0.289). Ulceration was also not significantly correlated with SLN (p = 1) in the cohort analysed, probably due to the matched distribution of this variable in both subgroups.
Tumour thickness was significantly higher in SLN+ (4.73 ± 3.55; mean ± SD) than in SLN– tumours (3.05 ± 2.23, p < 0.031; Mann?Whitney U test).
Correlational analyses
Protein expression levels. Comparing all CM tumours without SLN subgroup stratification (Spearman’s rank correlation; correlation coefficient 0.331, p < 0.011) with the SLN– subgroup (correlation coefficient 0.49, p < 0.007), revealed that tumoural VEGF and VEGFR-2 expression were positively correlated. Furthermore, comparing all CM tumours without SLN subgroup stratification (Spearman’s rank correlation; correlation coefficient 0.579, p < 0.000) with the SLN– subgroup (correlation coefficient 0.665, p < 0.001) revealed that tumoural VEGF and VEGFR-3 expression were positively correlated.
Protein expression levels and clinical data. Analysis of the tumours without subgroup stratification found that the expression levels of the proteins were not significantly associated with patient age, sex, histotype, regression, lymphovascular invasion, or tumour thickness. However, VEGFR-3 expression was negatively correlated with tumour thickness in the SLN+ tumours (correlation coefficient –0.383, p < 0.040).
Furthermore, expression levels of VEGF and VEGFR-3 in the SLN+ subgroup were significantly different between tumours with and without ulceration (Mann?Whitney U test). VEGF expression in tumours without ulceration was 10.23 ± 3.11 (mean ± SD) and in tumours with ulceration 8.06 ± 2.74 (p = 0.033).
VEGFR-3 expression in tumours without ulceration was 10.76 ± 2.31 (mean ± SD) and in tumours with ulceration 8.69 ± 3.4 (p = 0.042).
Binary logistic regression. Backward stepwise binary logistic regression modelling (covariates: age, sex, ulceration, tumour thickness, tumoural VEGF expression, epidermal VEGF expression, VEGFR-2 expression and VEGFR-3 expression) resulted in 2 independent predictors of SLN; tumour thickness (p = 0.038) and VEGFR-3 expression (p = 0.001) (Table II). The final model achieves Nagelkerke r2=0.559.
Table II. Binary logistic regression model showing the odds ratio (OR) of significant predictors for positive sentinel lymph node status (SLN+)
SLNB in CM allows identification of node-positive tumours, enabling discussion of the risks and benefits of completion lymph node dissection, and offering an approach to identifying patients who may benefit from adjuvant immunotherapy or targeted therapy (2). How-ever, the current practice of selecting melanoma tumours for SLNB is far from optimal, as only 20% of the biopsied tumours show a positive SLN (13).
The current study analysed whether biomarkers related to angiogenesis, such as VEGF and the receptors VEGFR-2 and VEGFR-3, can predict SLN in CM, thereby improving the preoperative selection of individuals for SLNB.
VEGF signalling plays a central role in physiological and pathological (lymph) angiogenesis and may be a potential target for anticancer therapy (14).
VEGF expression has been described in normal epidermis, epidermal appendages and skin tumours (15–17). VEGF not only reveals paracrine actions on endothelial cells, but may also promote skin carcinogenesis by altering the survival, proliferation or stemness of tumour cells via an autocrine loop (18).
Only a few studies have analysed the expression of VEGF and its receptors in CM and melanocytic naevi, most of which have revealed higher expression of VEGF in CM than in the naevi. Furthermore, invasive phenotypes in a vertical growth phase are characterized by higher VEGF production than CM in the radial growth phase (19–23). Primary CM with simultaneous metastases has shown stronger VEGF expression than CM without metastases (23), and it has been suggested that high VEGF levels may increase the risk of nodal metastases and could be considered an unfavourable prognostic factor (24, 25). Nevertheless, the results of studies regarding the impact of angiogenesis on the progression and metastasis of CM are ambiguous and no clear relationship between VEGF expression and prognosis has been verified (19, 23). In the current study VEGF was expressed in 55/58 CM tumours (95%). Tumoural VEGF expression in CM was significantly higher in SLN+ tumours than in SLN– tumours. These results are in agreement with the findings of other studies (23–25). VEGF expression in the current study was not correlated with sex, regression, lymphovascular invasion or tumour thickness. Interestingly, Bayer-Garner et al. also found no tendency of VEGF expression to be related to lymphovascular invasion, whereas they found VEGF immunoreactivity to be related to lack of regression (26). These authors speculated that a diminished VEGF immunoreactivity in areas of regression might be a result of fewer VEGF receptors in these areas (26).
Upon comparing all tumours irrespective of SLN and in the SLN– subgroup, the current study found that tumoural VEGF, VEGFR-2, and VEGFR-3 expression were positively correlated, indicating that tumoural VEGF production may stimulate expression of VEGFR-2 and VEGFR-3 in the context of an autocrine loop. These findings are in agreement with the observations of Mehnert et al., which showed a positive correlation between expression of VEGF and VEGFR-2/VEGFR-3 (19). Furthermore, Mehnert et al. showed that, in primary CM, expression of VEGFR-3 was significantly higher than that of VEGFR-2, concurrent with our results (19). We also found no significant correlation between tumoural VEGF expression and tumour thickness, consistent with the findings of Demirkesen et al. (23). Nevertheless, Straume & Akslen (21) found an inverse relation between VEGF expression and tumour thickness (21). The authors speculated that, in thicker melanomas, a lower baseline level of VEGF might be sufficient to maintain an established vascular system.
Interestingly, in most cases the highest epidermal VEGF levels were present in the epithelium directly above the CM. We interpret this high level of VEGF expression in peritumoural epidermis as an interaction of the CM with the overlying epithelium. Cytokines, such as transforming growth factor-alpha released by tumour cells, may stimulate VEGF production by epidermal keratinocytes (18). Paracrine effects of the increased epidermal VEGF production on endothelial cells may consecutively lead to angiogenesis, and may additionally stimulate proliferation, maintain stemness, and promote survival of tumours through direct effects on tumour cells (18). However, epidermal VEGF expression was not associated with SLN.
Only a few studies have analysed VEGFR-2 and VEGFR-3 expression in melanocytic naevi and CM (19, 27–29). VEGFR-2 is preferentially expressed in endothelial cells and regulates endothelial migration and proliferation (30). Given the availability of VEGFR-2-specific tyrosine kinase inhibitors, tumoural VEGFR-2 expression may have translational relevance. Few studies have shown the presence of VEGFR-2 in CM and a possible relationship of VEGFR-2 expression with tumour thickness (19, 21, 27). We found VEGFR-2 expression in only 19/58 melanomas (33%), and that it was significantly lower than that of VEGFR-3 in all tumours, irrespective of SLN. These findings indicate a minor role of VEGFR-2 compared with that of VEGFR-3 in melanoma pathogenesis. Interestingly, in our study the majority of VEGFR-2 expressing melanomas (79%) were nodular. Other studies revealed a higher percentage of VEGFR-2-positive CM (21, 27). These discrepancies might be explained by differences in the study populations investigated and by variations in antibody specificity.
In accordance with the findings of Mehnert et al. (19), VEGFR-2 expression in the current study was not correlated with sex, ulceration, regression, lymphovascular invasion, tumour thickness, or SLN.
Adult tissue expression of VEGFR-3, a key player in lymphangiogenesis and lymphatic metastasis, is largely confined to lymphatic endothelium (14, 31). VEGFR-3 expression in tumour cells and tumour vasculature has rarely been analysed, and there are conflicting reports regarding the location of VEGFR-3 (endothelial cells and/or tumour cells) (14).
We found that VEGFR-3 was expressed in 54/58 CM samples (93%) (tumour cell expression). VEGFR-3 expression was positively correlated with tumoural VEGF expression and was associated with positive SLN. In agreement with the findings of Mehnert et al. (19), VEGFR-3 expression was not associated with age, sex, ulceration, or histotype in our cohort. Furthermore, we found no association of VEGFR-3 expression with regression or lymphovascular invasion. As lymphovascular invasion was found in only a small number of cases, our results regarding this histological feature must be interpreted with caution. Nevertheless, it would be of interest to analyse the association of VEGF/VEGFR expression and lymphovascular invasion more in detail in future studies. Since intravascular melanoma cells are often difficult to detect on haematoxylin and eosin (H&E) stained sections it would be desirable to use double immunohistochemistry with markers for lymphatic endothelial cells and melanoma cells in order to detect lymphovascular invasion.
In summary, despite some limitations (i.e. retrospective analysis, relatively small cohort, no clinical follow-up data), the current study provides evidence that VEGF and VEGFR-3 expression may play a critical role in the formation of lymphatic metastases of CM, and that the investigation of these biomarkers may assist in risk-stratification and selection of tumours for SLNB. Nevertheless, to confirm the current findings, prospective multicentre studies that risk-stratify tumours for SLNB based on the expression of VEGF and VEGFR-3 are necessary to validate the predictive value of positive SLN in CM.


 Click to show fullsize
Click to show fullsize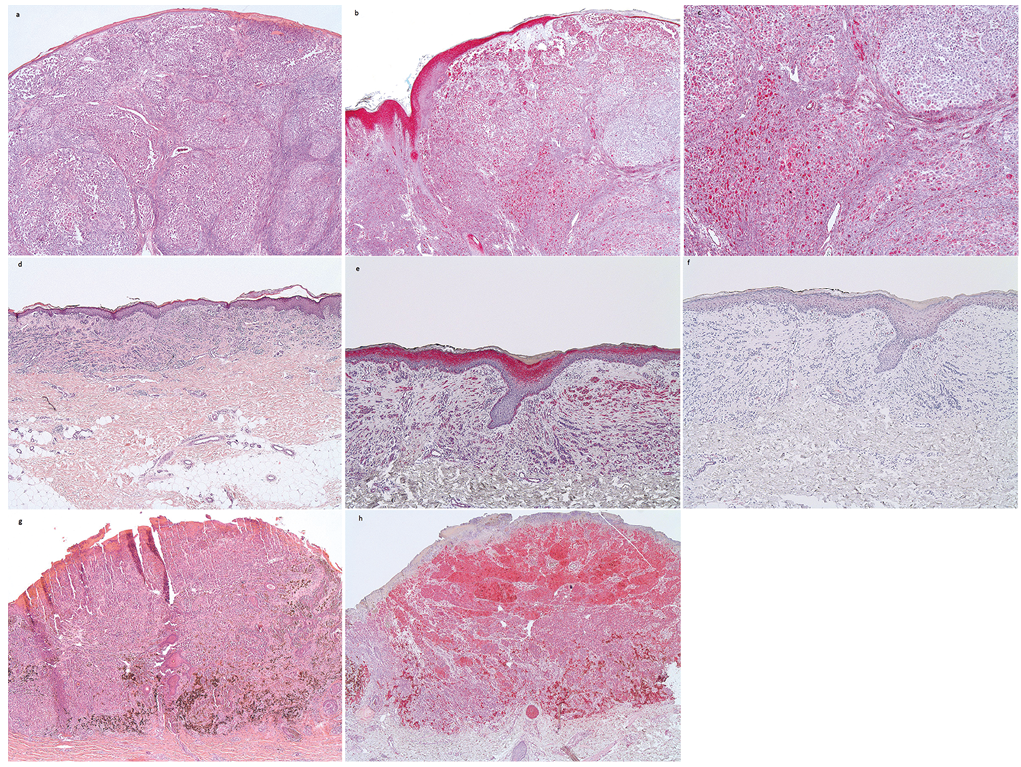 Click to show fullsize
Click to show fullsize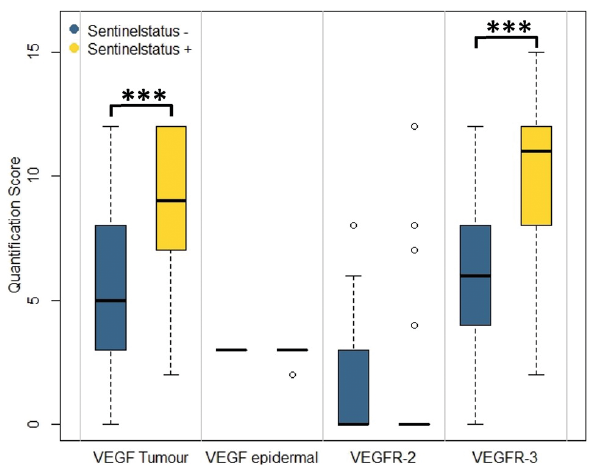 Click to show fullsize
Click to show fullsize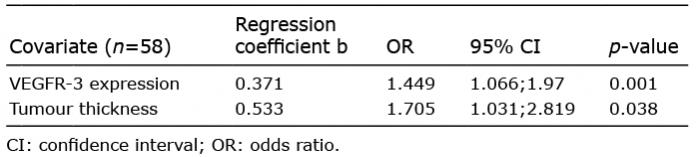 Click to show fullsize
Click to show fullsize