


1Section of Dermatology, Department of Medicine and Surgery, University of Parma, Via Gramsci 14, IT-43126 Parma, 2Department of Pathology,
University of Parma, Parma, and 3Skin Cancer Unit, Istituto Scientifico Romagnolo per lo Studio e la Cura dei Tumori (IRST) IRCCS, Meldola, Italy. E-mail: bea.defelici@gmail.com
#These authors contributed equally to this work.
A 45-year-old North African man referred to us with a bullet-like nodule, which was smooth, firm and pink, that had appeared one year previously on his left little toe (Fig. 1A, B). At first it was asymptomatic, but in the last 3 months the lesion had begun growing, completely involving the nail bed, with total dislocation of the nail plate, causing much discomfort. Dermoscopy revealed that the main feature was an extensive network of monomorphic thin and thick branched vessels on diffuse blushing background with central hyperkeratosis (Fig. 1C, D). X-ray and magnetic resonance imaging ruled out involvement of the distal phalanx. An incisional biopsy revealed a dermal low-grade proliferation of CD34+ spindle cells in a collagenous stroma, with hyperkeratotic epidermis (Fig. 2). Immunohistochemistry was negative for alpha-smooth muscle actin, CD99, S100, epithelial membrane antigen (EMA), desmin, myogenin, and beta-catenin. The nodule and the nail apparatus were thereafter completely excised with a V-Y flap reconstruction.
What is your diagnosis? See next page for answer.
Fig. 1. (A, B) Nodular bullet-like pink lesion with keratotic plug at the end of the left little toe. (C, D) Diffuse monomorphic vascular pattern characterized by arborizing vessels with high variability in length and thickness on diffuse blushing background (non-polarized digital dermoscopy, magnification ×20).
Fig. 2. Fibrous dermal tumour with spindled cells in a loose storiform pattern and numerous capillaries. Haematoxylin and eosin stain; panoramic view (A) ×1 and (B) ×4; immunohistochemistry for CD34, (C) ×4.
Acta Derm Venereol 2020; 100: adv00236.
Diagnosis: Superficial acral fibromyxoma
Superficial acral fibromyxoma (SAF) is a rare benign soft tissue tumour, first described by Fetsch et al. in 2001 (1). It usually appears in middle-aged adults as a painless slow-growing mass, almost exclusively localized in the hands and feet with a predilection for sub- and periungual areas (1). Histologically, it is characterized by a dermal proliferation of spindle and/or stellate cells in a myxocollagenous stroma with an immunohistochemical positivity for CD34 and CD99 and a possible focal positivity for EMA (1). Histologically, bone invasion is a rare event, even though up to one-third of cases can show a radiological involvement (1).
In the literature there are approximately 300 cases described (2), and only 5 of these have a dermoscopic description (3). The high variability of this tumour, together with the lack of specific clinical and dermoscopic clues, makes the diagnosis very difficult. In most cases a soft tissue tumour not otherwise specified is suspected, but SAF is often misdiagnosed as a ganglion or epidermoid cyst, fibroma, pyogenic granuloma, chondroma, wart or, even worse, with keratoacanthoma (KA), squamous cell carcinoma (SCC) or amelanotic melanoma (1), which causes anxiety in both the doctor and the patient. In our case, due to the hyperkeratotic plug and the recent fast growth, primary differential diagnosis was KA/SCC, but a dermoscopic monomorphic pattern of branched vessels as arborizing vessels is uncommon in these tumours (4). In addition, nodular basal cell carcinoma (BCC) can often exhibit arborizing vessels. However, acral BCCs are rare, an arborizing vascular pattern is not present and they are usually associated with genetic diseases, such as Bazex-Dupré-Christol syndrome, xeroderma pigmentosum, or Gorlin syndrome (5). Furthermore, various vascular patterns are identified in the SAF, but our case showed widespread branches of vessels with length and thickness variability, differing from the other cases described in the literature (3).
Once again, this case highlights the importance of dermoscopy and the identification of a vascular pattern for melanocytic and, moreover, non-melanocytic lesions. Nonetheless, dermatologists always have to be cautious when confronted with a nodular pink lesion, due to the possibility of dangerous differential diagnoses.
Total excision of SAF is usually sufficient to prevent relapses, and there is no evidence of malignant progression or metastatization (1, 2). Nevertheless, surgical management must be radical with tumour-free margins in order both to minimize the risk of local recurrences and to preserve the function and maintain the best possible esthetic result (Fig. 3).
Fig. 3. Follow-up at 3 weeks, after V-Y flap reconstruction.


 Click to show fullsize
Click to show fullsize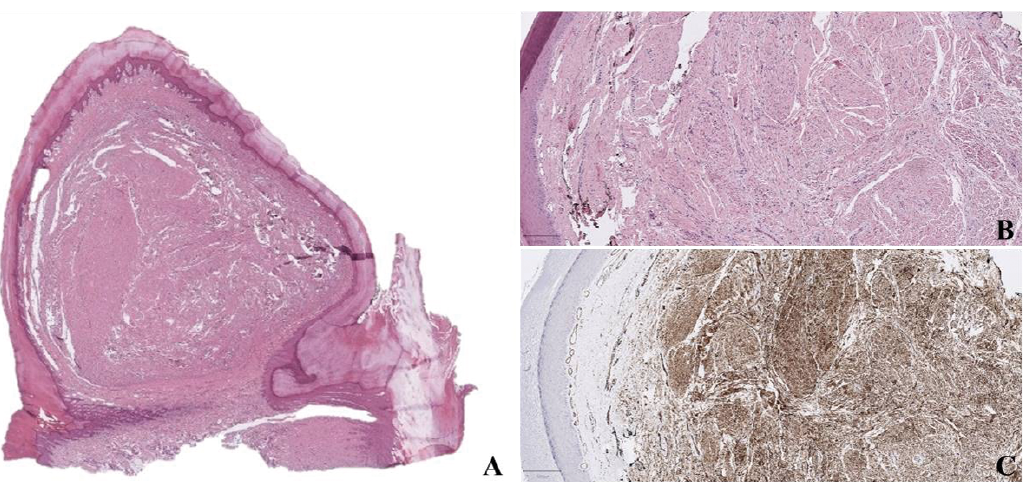 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize