


1Department of Dermatology and Skin Cancer, CHU Timone, APHM, Aix Marseille University, INSERM, CRCM, 2Department of Pathology, Aix Marseille University, INSERM, MMG, APHM, CHU Timone, 3EA 3279, Aix Marseille University, Marseille, and 4Department of Dermatology and Skin Cancer, CHU de Reims, Reims, France
#These authors contributed equally.
Most melanomas are diagnosed by the patients themselves or by their partners or relatives; they alone can describe its history. We designed a prospective cross-sectional study to describe patients’ perception of morphology, growth pattern and kinetics of their primary melanoma over 1 mm in thickness before resection. Patients were interviewed with a questionnaire, a grid representing 9 possible scenarios of melanoma growth, and a set of 87 photographs of potential aspects of melanomas and precursors. Most patients were able to describe the growth of their melanoma and select pictures representative of its successive aspects before resection. Among 453 patients, 60% reported a preexisting lesion present for years. Growth pattern scenarios concurred with tumor kinetics but with no statistical difference between nodular and superficial spreading subtypes. These subjective patient-reported indicators about melanoma growth over time could dynamically complement its objective pathological analysis otherwise static at a single time point.
Key words: patient; perception; melanoma; growth.
Accepted Jun 25, 2020; Epub ahead of print Jul 3, 2020
Acta Derm Venereol 2020; 100: adv00222.
Corr: Prof Jean-Jacques Grob, Department of Dermatology and Skin Cancer, CHU la Timone, 264 rue Saint-Pierre, FR-13885 Marseille Cedex 05, France. E-mail: jean-jacques.grob@ap-hm.fr
Among 464 interviewed patients having undergone primary melanoma resection, most could describe precisely the kinetics and patterns of growth, as well as the features of their melanoma over time. Patient-reported “subjective” information is often neglected by clinicians. However, such information regarding melanoma kinetics of growth over time is probably indicative of biological aggressiveness. Any patient-described features indicative of a fast growing melanoma may constitute an additional argument favoring close follow-up, or even adjuvant treatment in ambiguous AJCC III A situations. Furthermore, better understanding of patients’ perception of early melanoma will help tailor the detection advice offered to the community.
Despite dramatic progress in the treatment of advanced melanoma, early diagnosis of primary melanoma remains crucial. More than half of primary melanomas are detected by the patients themselves or by their partners or relatives (1–5).
Except for the few high-risk patients with multiple nevi followed-up via video surveillance or total body (digital) photography (6), the natural history of melanoma before diagnosis is unknown to clinicians and only patients have access to this information. Studies using artificial intelligence may help to understand early phases of tumor growth in high risk groups (7). However, most melanoma grow in an unselected population, not under surveillance, and interviews of patients are the only source of information about early melanoma growth including its aspects and kinetics. In order to improve early detection, we need to understand how early phases of melanoma growth are perceived by the patient. In order to understand the biological aggressiveness, we need to know how fast a melanoma grows before its resection. Therefore, although patient-reported data are subjective and submitted to memory bias, and for this reason often neglected, they may be a unique source of relevant information.
We conceived an original prospective survey to help patients describe the characteristics and history of their primary melanoma before initial resection. We used 2 instruments specifically designed to help patients recall and translate in a standardized way their perceptions: a visual grid representing the different possible scenarios of melanoma growth, and a set of photographs representing a panel of possible aspects of melanoma. The primary objective was to investigate the pre-resection phase of melanoma growth, from the patient’s point of view.
Study design
From January 2012 to January 2016, we prospectively included patients at the time of their first visit for primary melanoma in two dermatology departments: Marseille and Reims French university hospitals. According to French law in 2012, Institutional Review Board approval was not required in the setting of this non-interventional study. The procedures followed were in accordance with the Helsinki Declaration of 1975, as revised in 1983.
Inclusion and exclusion criteria
We included only patients with a primary melanoma of tumor thickness ≥ 1mm. In the absence of prior studies on patients’ perceptions, we wanted to maximize the probability of obtaining relevant information on melanoma concerning its natural history. We therefore excluded patients with incipient lesions for which the descriptive history may be too short to be informative with regards to growth kinetics and pattern. Eligible patients were consecutively included if they were over 18 years of age, were able to remember approximately when they first noticed a lesion at the site of their primary melanoma, and had signed an informed consent. Interviewers were asked to exclude patients if they or their partner or relative were considered unable to appropriately answer the questionnaire, whatever the reasons: clear statement from the patient or their partner or relative that they have not previously paid any attention to the lesion, major inconsistencies during the medical interview, obvious memory disorder…
Evaluation criteria
At baseline, demographic data, pathological data and initial melanoma resection date were collected. Two pathologists reviewed all histopathological reports. All pathology slides of nodular melanoma (NM) and those for which there was a doubt or ambiguity in the pathological report were reviewed to limit pathological misclassification.
Patient interview
Patients were interviewed according to a pre-established standardized questionnaire by specifically trained senior dermatologists.
Growth pattern scenario according to the patient
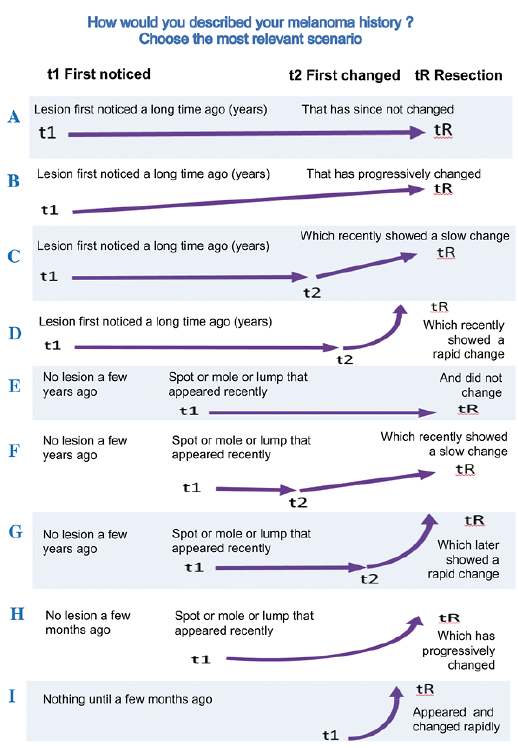
Patients were presented a specifically designed set of 9 figures representing the different possible scenarios of growth patterns from the time they first noticed a lesion to the time it was removed and diagnosed as a melanoma (Fig. 1). They were asked to choose among the 9 figures the one best matching the GPS of their melanoma.
Melanoma characteristics according to the patient
Patients were interviewed with the help of a grid including 87 photographs (Fig. 2) chosen to represent the variability of early melanoma and nevi aspects. Each patient had to choose at least one picture that resembled most the first lesion they noticed on the melanoma site (t1); if relevant, at least one picture of the lesion at the time it changed or became curious or suspicious (t2) and, at least one picture at the time of first resection (tR). Those who were unable to recall, or declared themselves unable to find one representative picture within the grid, were not excluded from the study.
Melanoma kinetics index (MKI) assessment
The growth rate of each primary melanoma was calculated by the MKI (8, 9) according to a previously described method using the formula: MKI = (Breslow) / (t1-tR) for de novo primary melanoma (< 5 years); MKI = (Breslow / (t2-tR) for primary melanoma on a preexisting lesion (> 5 years). The 4th quartile was defined as “Fast growing melanoma”.
Statistical analysis
Categorical variables were expressed as counts and percentages. The distribution of GPSs was analyzed according to histological subtype and to melanoma kinetics with a χ2 test. A p-value < 0.05 was considered to be statistically significant.
Fig. 1. Grid presented to patients in order to help them describe their melanoma’s history in a standardized manner (indicative translation from French). Each figure (from A to I) represents a different melanoma growth pattern scenario (GPS) as described by the patients.
Fig. 2.Grid of 87 photographs used by each patient to assess their melanoma characteristics.
Description of the population and circumstances of diagnosis
A total of 464 patients were included and 453 analyzed (11 were excluded because considered unable to answer by the interviewers). The median age was 61 years (range 18–89); 248 (55%) were male. Patient clinical and histological characteristics are reported in Fig. S1.
In our cohort, 250 patients (55%) detected their melanoma themselves and asked for a consultation, 127 patients (28%) were alerted by their relative/partner, and 60 (13%) by a health professional, mostly either a general practitioner (5%) or a dermatologist (6%) (Fig. S2).
Among cases detected by patients, 206 patients were able to specify the factors raising their attention (Fig. S3):
– a change in a preexisting lesion in 107 cases (43%), that included a combination of size and/or color and/or shape changes
– symptoms in 66 cases (26%) encompassing bleeding, itching, and pain
– appearance of a new/abnormal/ugly lesion in 33 cases (13%)
while 44 patients (18%) were unable to answer this question.
Growth pattern scenario according to the patient
Only 3 patients could not choose any pattern among the 9 scenarios and were excluded from the analysis for simpli-fication. Among the 450 remaining patients, 60% reported that a prior lesion was already present for years before melanoma was diagnosed (patterns A to D, Table I). Conversely 26% of patients certified the absence of any prior lesion a few years ago (patterns E to G), and 14% the absence a few months ago (patterns H to I).
Table I. Histopathological subtypes, growth kinetics, mode of detection and melanoma growth pattern scenario (GPS) according to the patient.
Melanoma characteristics according to the patient
Using the grid of 87 photographs (Fig. 2), 64%, 69% and 68% of patients were able to select a single picture as representative of their melanoma at t1, t2 and tR, respectively. Only 16%, 7% and 8% found no relevant pictures to match their lesion features at t1, t2 and tR, respectively.
At t1, the most frequently selected photographs were in decreasing order numbers 17, 20, 33, 32 and 16 (Fig. 3), and most of the lesions identified by the patients were pigmented and flat. At t2, the most frequently selected photographs in decreasing order were 53, 17, 20, 33, 38 and 41, with a mix of flat lesions and nodules. At tR, the most frequently selected photographs in decreasing order were 53, 22, 17, 20 and 52. Interestingly, many obviously-malignant-for-a-dermatologist lesions, such as depicted in pictures 7, 8, 21, 26 and 37, were never or very rarely cited. Among the 87 photographs, only six: 6, 8, 59, 80, 81 and 84 were never chosen by any patient at t1, t2 nor at tR.
Fig. 3. Distribution of photographs according to the frequency of selection by patients. Each bar represents the selection index calculated as follows: when patients cited only one lesion, the value is 1, when they chose n lesions, the value is 1/n. t1 was the time when the patient first noticed a lesion on the site where the primary melanoma was later diagnosed; t2, if relevant, the time when he/she first noticed that this lesion changed or became curious or suspicious and tR, the time of first resection (tR).
Considering it likely that individuals with no previous experience with melanoma are not as able to recognize characteristic signs from lesion photographs as are dermatologists, we asked 4 such inexperienced individuals (non-health professionals and non-skin cancer patients) to look at the 87 photograph grid, and to cluster the lesions that they considered more or less the same. They simplified the 87 lesions of our “expert grid” into a “naive grid” with 30 clusters. A dermatologist (CG) helped them to express in basic language the common traits of their clusters (e.g. “pink spot”, “blueish lump” etc. (Fig. 4) (Indicative translation from French). Using this “naive grid” for t1, “brown spot or mole” (cluster 13) was by far the most cited (30%) cluster, followed by “irregularly-shaped dark spot or mole” (cluster 15). For t2 and tR, “ugly dark brown lump” (cluster 24) and cluster 13 were the most frequently mentioned (18%/19%, and 16%/12%, respectively).
Fig. 4. Thirty “naïve” clusters defined from the 87 photographs according to the similarity of their clinical features by 4 non-experienced investigators (indicative translation from French).
Growth pattern scenario according to histopathological subtypes
There was no clear difference in the distribution of GPS between superficial spreading melanoma (SSM) and nodular (NM) subtypes (p = 0.105). The other subtypes could not be statistically compared due to the low number of cases. Patients describing a biphasic history (growth pattern scenarios C, D, F, and G of Fig. 1) accounted for 71% of SSM, 74% of NM, 47% of acrolentiginous melanoma (ALM) and 77% of lentigo maligna melanoma (LMM) respectively (Table I). A long and biphasic growth (pattern C and D) was described for 56% of SSM and 53% of NM. Only 26% of patients with NM described a monophasic GPS (patterns A, B, E, H, and I), and only 5% a sudden growth starting from nothing (pattern I).
Melanoma characteristics according to histopathological subtype
At t1, among patients with SSM and NM, the most cited photographs were “brown spot or mole” (cluster 13) (34% and 19% respectively) in Fig. 3. For SSM, 24% of cases at t2, and 22% at tR were described as “ugly dark brown lump” (cluster 24). For NM, case descriptions were equally distributed among clusters 24, 15 “irregularly-shaped dark spot or mole” and 22 “light brown lump” at t2 (each with 10%), but cluster 24 was dominant at tR (19%). Other histopathological subtypes were too rare to permit an analysis.
Melanoma growth pattern scenario as a function of their growth kinetics
“Fast growing melanoma”, defined as the 4th quartile of MKI, had a rate of growth > 0.7 mm/month. Compared to the 1st quartile defining the “very slow-growing melanomas”, the distribution of GPS was significantly different (p < 0.001) between “fast growing melanoma” and “very slow growing melanomas” (Table I). The GPS types H and I, representing a short and monophasic course, were described by 21 patients (19%) with “fast growing melanoma”, and by only 4 patients (3%) with “very slow-growing melanoma”. GPS type A and B, representing a very long course was described by 22 % of the patients with “very slow-growing melanoma “and by 1 % of the patients with “fast growing melanoma”.
Melanoma characteristics as a function of growth kinetics
At t1, for both patients with very slow and those with fast growing melanoma, the most cited photographs belonged to cluster 13 “brown spot or mole” (33% and 32% respectively). At tR, for patients with very slow-growing melanoma, clusters 13 and 24 “ugly dark brown lump” were the most often cited. In patients with fast growing melanoma at tR, cluster 24 was the most often selected.
Using an original but standardized approach, most patients of this large cohort were able to describe the early features of their melanoma and its history before resection, showing that patients know much more about their melanoma than what clinicians tend to expect.
While it is easy to be skeptical about seemingly unclear stories related by patients, they remain the only source of evidence concerning the whole course of their melanoma. Such a “subjective” assessment of the overall growth over time might be more informative about the biological behavior of a melanoma than any retrospective assumption, based on a clinical or pathological “objective” assessment at a single point in time at tumor resection. Most patients in our study were able to describe quite clearly their lesion at t1, t2 and tR. Patients did have more difficulty at describing their lesion at t1 and t2 than at tR, not only because t1 and t2 were further in the past, but also because the medical decision to remove the lesion at tR likely imprinted this final image in their memory. Although the patients were free to choose as many photographs as they wished, most of them selected a single one, suggesting they were confident enough in their choice. Likewise, most were able to choose a single growth scenario among the 9 proposed.
This study gives some clear hints about the natural history of primary melanoma before resection. The only available information about the growth process of early tumors currently comes from monitoring photographs of atypical nevi in a high-risk population (10, 11). However this high-risk group, with a bias in favor of slow-growing melanoma, does not reflect the whole population with melanoma, and especially not those patients who may develop fast-growing “killer” melanomas.
In our cohort, 60% of patients described their melanoma as evolving over many years before resection. However, it remains impossible to ascertain whether this lesion was already a melanoma upfront, or a precursor nevus. Although the proportion of melanoma which develop from nevi is unknown, 1/3 of SSM are considered to develop from pre-existing nevi (12). Our data are in line with an Australian survey in which 65 % of patients reported “having a spot” where the primary melanoma developed (4).
This study gives a very interesting description of the reality of patients’ perception of melanoma from the early disease stages, which may have consequences in terms of early detection. When they first saw their melanoma, patients mainly recalled common flat pigmented lesions. Regardless of whether this perception reflects or not how a dermatologist would describe the lesion, or describes an already existing melanoma or nevus, it does underline the difficulty for very early detection by patients themselves. At the time of resection, many patients still describe flat pigmented lesions (mixture of images of atypical nevi and melanoma). Furthermore, 2 of the 5 most cited photographs chosen for melanoma at tR are images of common nevi. Nevertheless, the dermatologists who proposed resection would probably have chosen other images to represent the situation. This photograph choice illustrates the differences in levels of granularity between the non-experienced and expert population in terms of image analysis. Experts take into account many subtle features to which a non-experienced population is completely blind and probably explains why patients probably always miss some melanomas. Other patients did describe brown or black nodules (using mostly images of typical melanoma) for which the dangerousness is easier to perceive even by the non-experienced individual. This study illustrates the differences between non-experienced individuals and experts in terms of analytical criteria when faced with classifying skin lesions and nevi. With a view to achieving earlier detection of melanoma, any action taken to better educate the community will have to take into account this difference between patients and doctors in their perception of the same reality.
Our study has introduced an original approach to histoclinical subtyping and classifying melanoma growth from early stages. Subjective perception by patients is consistent with the concept of melanoma growth from a flat to a nodular lesion, suggesting that while often misinterpreting this process, patients do clearly see it happening. Histoclinical subtypes are still considered as separate entities although molecular differences remain to be clearly identified (13). Primary melanoma growth is assumed to comprise 2 phases: radial and vertical (14), with a long radial phase in ALM and LMM, intermediate in SSM, and very short in NM. In theory, we should expect NM to be represented mainly by fast and monophasic patterns, and SSM mainly by biphasic patterns. Looking at the photographs and scenarios chosen by patients to describe their SSM and NM, no striking differences are apparent in the distribution of the different patterns. In other words, patients do not perceive any differences between SSM and NM as has been previously reported (15). Such data argue against different natural histories between NM and SSM, suggesting instead that many NM are in fact SSM in which the vertical growth phase secondarily “swallowed” the radial phase.
Kinetics of growth of primary melanoma has been shown to be an independent prognostic factor (8, 9, 16, 17). While most fast growing melanoma are often believed to be nodular (13, 18, 19), our data suggest that some melanoma can grow fast despite not initially looking like nodules. Based on patients’ perceptions therefore, high kinetics does not exclude a biphasic course, a long initial history may end in a fast process, and more generally fast growth does not necessarily indicate nodular melanoma.
This study has some limitations. The patients were prospectively interviewed immediately after resection, when they had the highest probability to recall information. The responses they gave were dependent on their state of memory thus, as with any such memory-based study, a memory bias was introduced. We did our best to limit this bias by never enforcing an opinion or even suggesting towards a response. We included only primary melanoma with a thickness ≥ 1 mm, for the reasons described above. This selection might have accounted for a higher proportion of NMs than expected. The distribution of histoclinical subtypes in this survey nevertheless closely resembles equivalent series in the literature (20). Subjective assessment such as that provided here in the patient-reported data, may be considered a strong limitation or even a bias. Indeed, many clinicians tend to trust only what they see, leading to the neglect and underuse of patient-provided data. However, this study clearly shows that most patients can generally recall quite well the last months or even years history of their melanoma but simply did not associate its appearance with any danger.
This study may contribute towards improving the early detection of melanoma. It has demonstrated potential differences in the perception of nevi and/or growing melanoma between dermatologists and non-experienced individuals. We and others have demonstrated the interest of visual education campaigns (21–26) to stimulate holistic visual pattern recognition, a process shown to outperform education with algorithms like ABCDE (27, 28). In order to choose the right images for use in any such community educational campaign, further work is warranted to specify what granularity non-experienced individuals can really perceive. Considering that most patients in our series were conscious of changes in their lesions likely before the melanoma developed, the right education may help such individuals correctly interpret these changes.
Our findings highlight the need for clinicians to put more trust in the subjective, and thus often considered unreliable, information provided by patients concerning their melanoma history. Indeed, “subjective” cannot be considered as wrong, just as “objective” does not mean informative. This study supports the consistency of patients’ descriptions of their primary melanoma, underlines the potential value of patient-reported kinetics as a criterion for medical decision, and provides some hints towards improving community education campaigns.
Funding sources: Société Française de Dermatologie, Assistance Publique des Hôpitaux de Marseille
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize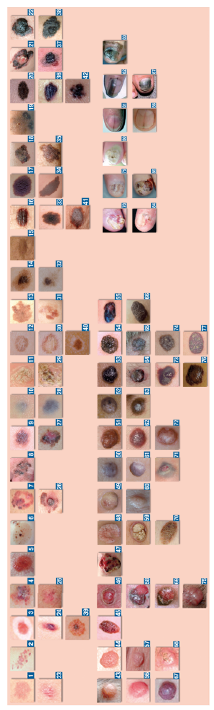 Click to show fullsize
Click to show fullsize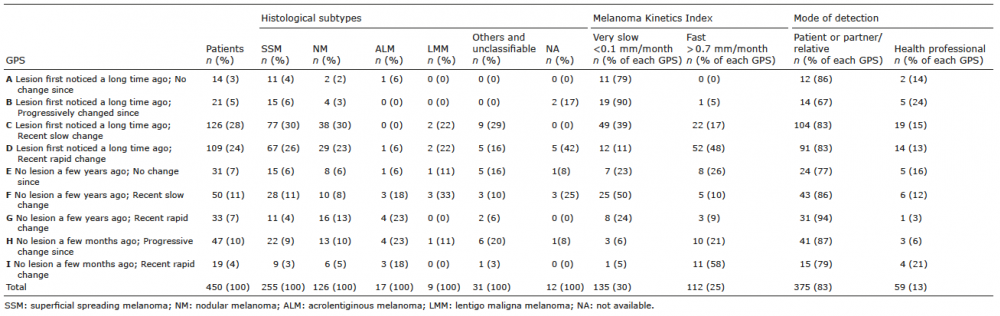 Click to show fullsize
Click to show fullsize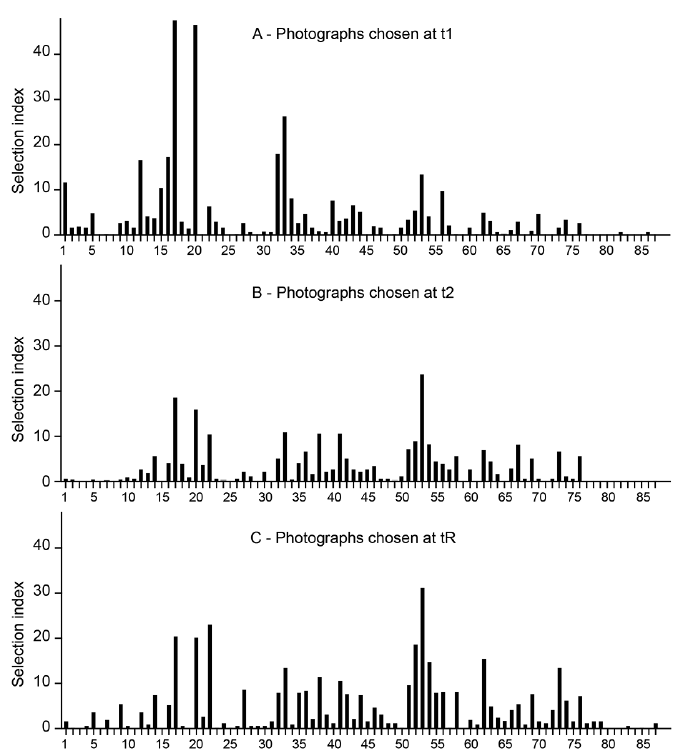 Click to show fullsize
Click to show fullsize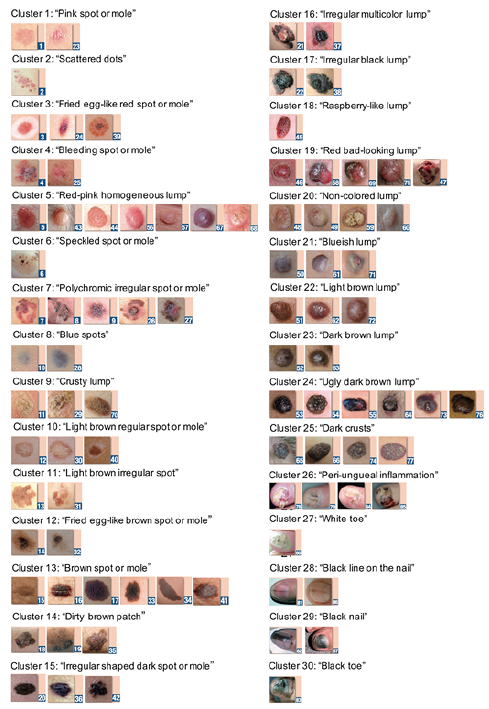 Click to show fullsize
Click to show fullsize