


1Department of Dermatology and Allergy, Section Paediatric Dermatology Outpatient Department, Charité – Universitätsmedizin Berlin, Charitéplatz 1, DE-10117 Berlin, 2Center for Dental and Craniofacial Sciences, Department of Orthodontics, Dentofacial Orthopedics and Pedodontics, Charité – Universitätsmedizin Berlin, CC3, Berlin, and 3Institute for Human Genetics, University Medical Center Freiburg, Freiburg, Germany. E-mail: karola.stieler@charite.de
A 4-year-old German girl was referred for specialized hair consultation due to short fine, blond sparse hair that had never necessitated a hair-cut and varied in length (max. 7 cm) (Fig. 1a). Assessment of her deciduous teeth appeared within normal age limits. Hair root examination and trichogram from the occipital region showed telogen effluvium at the rate of 70% (Fig. 1b). Possible causative factors were ruled out via complete blood count. A repeated trichogram and root examination after one year resulted in a 49% positive result for telogenic (clubbed) hair roots.
At 9-years of age, the patient presented for a follow-up visit with continued hair growth abnormalities. Conspicuously, only the central maxillary incisors had presented (Fig. 2a). The intraoral examination revealed complete primary dentition; the orthopantomogram (OPG) (Fig. 2b) indicated that only the permanent central maxillary incisors, first mandibular premolars and all second permanent molars were in the early developmental stages. Delayed dental development and oligodontia were the primary characteristics with this patient with twenty permanent teeth absent.
Due to the presence of multiple tooth agenesis (TA) to her permanent dentition, we hypothesized a possible link between the TA and the hair anomalies and initiated a genetic work up.
What is your diagnosis? See next page for answer!
Fig. 1. The girl at the age of 5 years with sparse, fine blond hair (a) with a characteristic telogen hair root pattern in the trichogram (b) with up to 70% telogen hairs (normal rate < 20%).
Fig. 2. Primary teeth at the age of 9 years 8 months with only 2 permanent teeth in situ* (A) showing in the orthopantomogram (OPG) at the age of 9 years, 2 months 8 permanent teeth (*) (oligodontia) (B).
Acta Derm Venereol 2020; 100: adv00223.
Diagnosis: Trichodental syndrome
The differential diagnoses of everlasting sparse not-growing hair comprise (i) Loose Anagen Hair and (ii) Short Anagen Syndrome (SAS). Loose anagen hair has an elevated rate of dystrophic hair roots in trichogram and was ruled out; whereas SAS can be confirmed by anamnesis and a typical clinical picture with short hair that never needed a haircut and a repeatedly elevated rate of telogenic hair roots. However, our patient additionally had tooth anomalies of the permanent denture thus raising the question of a connection between these two lead symptoms. Hereditary hair and teeth anomalies are typical signs of ectodermal dysplasias, leading us to the diagnosis of Trichodental syndrome.
Trichodental syndrome (OMIM: 601453), syn.: trichodental dysplasia, Kersey syndrome (1) is the association of hair anomalies with the developmental absence of teeth (1, 2). It is rarely observed and generally has an autosomal dominant trait, whereas our patient shows an autosomal recessive trait (see below). It can be associated with intellectual disability and microcephaly (2). Described patients show hair anomalies either as SAS or lustreless, slow-growing sparse and fine hair (3).
SAS is a congenital yet usually harmless condition that is easily diagnosed by medical history, clinical examination, a positive hair pull test, and trichogram (4, 5). Affected patients complain of fine short hair that does not grow long, negating the patient’s need for hair cutting. The typical patient has fine, blond, diffusely thinned hair, trichoptilosis, a positive hair pull test, and a characteristic trichogram. SAS shows a higher than 50% telogen hair rate in the trichogram hypothesized to be due to a shortened hair growth cycle with an active growth phase length of only few months instead of years (4). SAS tends to improve spontaneously after puberty and is rarely associated with other conditions, such as with our case.
Delayed dental age (6), tooth agenesis of several permanent teeth (6), bigeminism (tooth fusion) of inferior lateral incisors and canines (1), peg-shaped lateral incisors (3), and “generalized shell teeth” have been reported in the existing literature, in association with trichodental syndrome. In our patient, tooth morphologic deviations cannot yet be evaluated due to the patient’s dental age.
Analysis of the patient’s DNA for mutation was conducted by using multi-gene-panel sequencing by NGS revealed a compound heterozygous mutation in the gene WNT10A, one heterozygous nonsense mutation c.321C>A (p.Cys107*) in exon 2 and one heterozygous missense mutation c.682T>A (p.Phe228Ile) in exon 3. The mother carried the nonsense mutation p.Cys107* whereas the father carried the missense mutation p.Phe228Ile. It should be underlined that both mutations have been described in patients within the broad spectrum of ectodermal dysplasia (7, 8) including Schöpf-Schultz-Passarge Syndrome (9, 10) and are therefore considered a class 5 pathogenic variant according to the criteria ascribed by the American College of Medical Genetics and Genomics (ACMG) (11).
Tooth agenesis patterns related to WNT10A-gene mutations can vary from hypodontia (at least one congenitally absent tooth) to anodontia (all teeth congenitally absent) (12). According to the existing literature, more than half of patients with biallelic mutations have clinical symptoms of other ectodermal tissues (2, 13) in addition to tooth agenesis.
We conclude that this case of SAS, which is often underdiagnosed, was associated with anomalies exclusive only to the permanent teeth. To our knowledge, this phenomenon has yet to be reported previously in trichodental syndrome. Our identification of biallelic mutations (compound heterozygous) of the WNT10A gene in this case has also not been previously established in trichodental syndromes nor known to be the causative mutation associated with Odonto-Onycho-Dermal-Dysplasia or other ectodermal dysplasias such as Schöpf-Schultz-Passarge Syndrome and severe oligodontia (7).
Julia Küsel (Sequencing) and Andreas Zimmer (Bioinformatics).


 Click to show fullsize
Click to show fullsize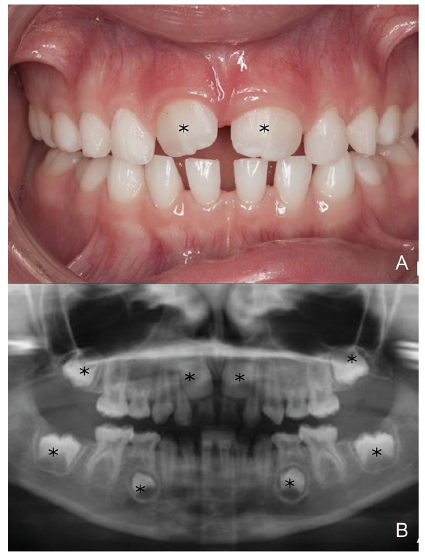 Click to show fullsize
Click to show fullsize