


Department of Dermatology, Iwate Medical University School of Medicine, 1-1-1 Idaidori, Yahaba-cho, Shiwa-gun, Iwate Prefecture 028-3694, Japan. E-mail: ktakami@iwate-med.ac.jp; hamano@iwate-med.ac.jp
Accepted Jul 7, 2020; Epub ahead of print Jul 27, 2020
Acta Derm Venereol 2020; 100: adv00237.
Merkel cell carcinoma (MCC) is an aggressive and rare cutaneous cancer with poor survival outcomes. We report here 2 cases of metastatic MCC (mMCC) for which a combination of avelumab, an anti-programmed death-ligand 1 (PD-L1) inhibitor, and radiotherapy (RT) was effective. In both cases, metastatic lesions outside the irradiated area decreased in size and eventually disappeared, and an abscopal effect was obtained. We believe that a combination of RT and immune checkpoint inhibitor (ICI) administration should be actively considered for treatment of mMCC.
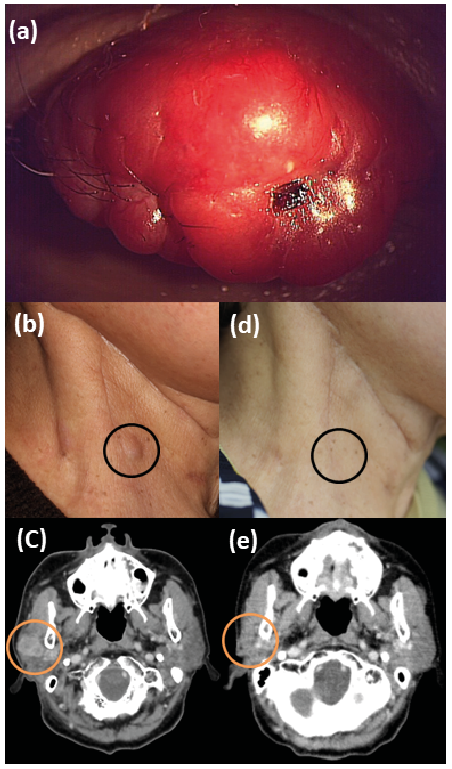
Case 1. A 70-year-old woman presented with a 1-month history of a red tumour on her right upper eyelid. Clinical examination revealed a 26-mm red-coloured hard mass (Fig. 1a), and an excisional biopsy revealed MCC. Therefore, wide local excision and biopsy of a sentinel lymph node (SLN) in the right side of the neck were performed. As the SLN was positive for metastasis, right cervical lymph node (LN) dissection and adjuvant RT (upper right eyelid: 50 Gy; right side of the neck: 60 Gy) were performed. Six months later, however, the patient developed subcutaneous metastasis in the right side of the neck (Fig. 1b) and LN metastasis in the right parotid gland (Fig. 1c). Subsequently she underwent RT (20 Gy) for the LN metastasis, and avelumab (10 mg/kg) was administered intravenously every 2 weeks. Eight weeks after the start of avelumab administration, the subcutaneous metastasis in the right cervical region, which had not been irradiated, gradually decreased in size and eventually disappeared (Fig. 1d). Computed tomography (CT) confirmed ablation of the metastatic LN (Fig. 1e). To date, avelumab has been continued. Within 24 h after the first administration, the patient developed a fever, which persisted until the time of the second administration; however, there was no fever after the third administration.
Fig. 1. A 70-year-old woman with metastatic Merkel cell carcinoma. (a) A 26-mm red tumour on the right upper eyelid. (b) Subcutaneous metastasis in the right side of the neck (black circle). (c) Lymph node (LN) metastasis of the right parotid gland (yellow circle). (d) Disappearance of subcutaneous metastasis in the right side of the neck (black circle). (e) Treatment of LN metastasis of the right parotid gland (yellow circle).
Case 2. An 86-year-old woman presented with a 1-month history of a red tumour on her nose. Clinical examination revealed a 10-mm red-coloured hard mass, and surgical excision was performed. An excisional biopsy revealed MCC. The patient was unwilling to undergo wide local excision. Fourteen months after the excisional biopsy, left cheek and bilateral LN metastases developed. The metastases to the left cheek and left cervical LN resulted in a large 50-mm subcutaneous tumour (Fig. S1a), which grew rapidly and became painful. CT revealed right cervical LN metastasis, and 2 swollen LNs, each measuring 17 mm were detected (Fig. S1c, d). Avelumab was administered intravenously (10 mg/kg). RT (45 Gy) was performed for the left cheek and left cervical metastatic lesions. After 6 weeks of treatment (i.e. at the end of irradiation and after the third administration of avelumab), the left cheek tumour and left cervical LN metastasis decreased significantly in size (Fig. S1b). The LN in the right cervical region, which had not been irradiated, became swollen, but decreased in size from 17 mm at the start of the treatment to 8 mm after treatment (Fig. S1e, f). No side-effects associated with the treatment were observed. To date, administration of avelumab has been continued.
mMCC is a rare and aggressive type of skin cancer with poor survival outcomes (1). Although mMCC is a chemosensitive disease, durable responses are rare (2). Retrospective studies of first-line chemotherapy for patients with mMCC have reported median progression-free survival periods of 3.1–4.6 months (3, 4), highlighting the need for improved treatment options. Compared with conventional chemotherapeutic drugs, PD-L1 inhibitors have been proven to be highly effective for treatment of mMCC. Kaufman et al. (5) have reported a multicentre phase 2 second-line trial (EMR 100070-003 trial) to determine the efficacy and safety of one such human PD-L1 inhibitor, avelumab, for which an overall response rate of 31.8% was observed at 6 months after the start of treatment in patients with chemotherapy-refractory MCC. On the other hand, another study has reported a higher response rate of 62.1% in 29 patients who received avelumab as a first-line treatment for 3 months (6).
In the present 2 cases, the tumours decreased rapidly in size, not only within the irradiated site, but also outside it, suggesting an abscopal effect, which is a phenomenon characterized by regression of untreated metastatic lesions following local RT for other lesions. Such an abscopal effect is believed to be mediated by immunological elements that may include immune cells, cytokines and tumour-associated antigens. When tumour cell apoptosis is induced by irradiation, release of tumour-associated antigens and induction of damage-associated molecular patterns (DAMPs) has been noted. In turn, these signals activate dendritic cells and induce cytotoxic T cells, resulting in an antitumor effect even at the non-irradiated site (7, 8). ICIs have recently been used to treat several types of carcinoma, such as malignant melanoma and lung cancer, and exert their antitumor effects by activating cytotoxic T cells. The abscopal effect is easier to induce by administering ICIs and performing RT, thereby enhancing both the antitumor effect and the local effect. Several studies have suggested that the abscopal effect is more likely to be induced with the combined use of RT and ICIs (9–11).
MCC is a tumour that appears amenable to the abscopal effect. Since MCC has high radiation sensitivity, the tumour cells are more prone to apoptosis than other carcinomas when exposed to RT. This may lead to cytotoxic T-cell activation via DAMPs and the production of various cytokines. Activated cytotoxic T cells and various cytokines exert antitumor immunity throughout the body, and it is considered that co-administration of ICI can enhance the efficacy of this process. Therefore, in patients with multiple metastases from MCC, an abscopal effect can be expected, and ICI administration combined with RT should be considered. Although radiation has been employed as local therapy for MCC up to now, it may be developed as systemic therapy through antitumor immunity when used in combination with ICI. However, the number of reports documenting an abscopal effect in mMCC is still limited (11–13). Bloom et al. (11) and Xu et al. (12) reported cases in which an abscopal effect occurred through a combination of ICI and RT. On the other hand, Cotteter et al. (13) reported a case in which an abscopal effect occurred only as a result of hypofractionated RT (12 Gy in 2 fractions) for cutaneous metastases in the lower limb. Bloom et al. (11) employed conventionally fractionated radiation (45 Gy in 25 fractions), whereas Xu et al. (12) used 8 Gy of irradiation in a single dose. In all of these cases, complete tumour regression was reported. All of the previous reports described complete regression of the tumour with no serious side-effects. Therefore, a combination of ICI and radiation therapy is a well-tolerated treatment. In order to establish effective combination therapy with ICI and RT, a number of issues still need to be clarified, such as the timing of combined use, the optimal total dose, and whether it should be fractionalized radiation or hypofractionated radiation. Therefore, studies of additional cases are required.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize