


1Empano, Peter Bangs Vej 7A, DK-2000 Frederiksberg, Denmark, 2Department of Clinical Research, University of Southern Denmark and Odense University Hospital, 3Department of Dermatology and Allergy Centre, Odense University Hospital, Odense, Denmark, and 4Svettmottagningen, Stockholm, Sweden. E-mail: Johannes.kristensen@dadlnet.dk
Accepted Jul 7, 2020; Epub ahead of print Jul 29, 2020
Acta Derm Venereol 2020; 100: adv00240.
In a recent systematic review (1) we found 7 controlled studies of anxiety and depression in primary hyperhidrosis (PH). Figures for psychiatric comorbidity varied substantially, from zero to almost 50%, depending on the selection of patients and measuring tools. This prompted us to perform an observational study of the prevalence of anxiety and depression in Swedish patients with hyperhidrosis. A measurement of body image was included, since a decrease in body image has been linked to anxiety and depression, and it was expected that body image would be decreased in PH (2). The aim of the study was to determine the correlation coefficient between body image, anxiety and depression.
The study was performed in the first week of July 2019, and included all Swedish patients (n = 98) attending the Hidros Denmark clinic in Copenhagen during that week for planned treatment with botulinum toxin. None of the patients were excluded. Three patients had to be omitted due to problems in the coding process leaving 95 patients (response rate 100%). A thorough physical examination was performed. Before attending, patients had been asked to complete a general health pro forma. On arrival at the clinic they completed the Body Image State Scale (BISS) (2) and the Hospital Anxiety and Depression Scale (HADS) (3) as part of the routine examination. The patients were asked to complete the questionnaires online after providing oral and written consent. Danish law did not require this study to be evaluated by the local ethics committee, as it was classified as quality assurance. Danish law is valid for Swedish patients attending a treatment facility in Denmark. All data were processed anonymously using Excel and Stata. Demographic characteristics and details were recorded for each patient. Psychiatric and somatic diagnoses and medications were also recorded.
The HADS is a self-assessment Likert scale questionnaire that identifies anxious and depressive symptoms in the previous week. The questionnaire contains 7 questions on depression and 7 on anxiety. Higher values indicate a greater level of depression or anxiety (3). It was intended to use the HADS total scale, as well as the single scales for anxiety and depression. The total scale (HADS-T or Distress-scale) is considered more sensitive. The HADS has been validated in the Swedish population, from which we obtained normative values (4).
The BISS is designed to indicate the patients’ perception of their body image at the time of questioning. It is a Likert scale questionnaire with 6 blocks of 9 questions. The higher score the better the person’s body image at present. This scale has been validated with American college students, but not with Swedish patients. It was chosen for use in this study, as it would be suited to use before and after treatment and for correlation calculations. A license was obtained (3).
Statistical evaluation
For each scale means and standard deviations were calculated for the total sample and stratified by group. Furthermore, the results from our sample were compared with reference material using a 2-sample t-test, both total and stratified by sex. The normality of the measurements was ascertained by quantile-quantile plots. p-values < 0.05 were considered statistically significant.
A total of 98 patients completed the questionnaires (3 patients were excluded due to problems with anonymous coding) leaving 95 patients (34 men (36%) and 61 women (64%)). Mean age 32 ± 10.9 years, body mass index 25.4 ± 5.2 kg/m2, Hyperhidrosis Disease Severity Scale 3.7 ± 0.44 (very high), Dermatology Life Quality Index 15.8 ± 6.6 (very low quality of life), number of areas treated 2.86 ± 1.45 (mostly hands, feet and axillae). Nine patients were taking psychotropic drugs, 8 were diagnosed with depression, and 3 were diagnosed with anxiety.
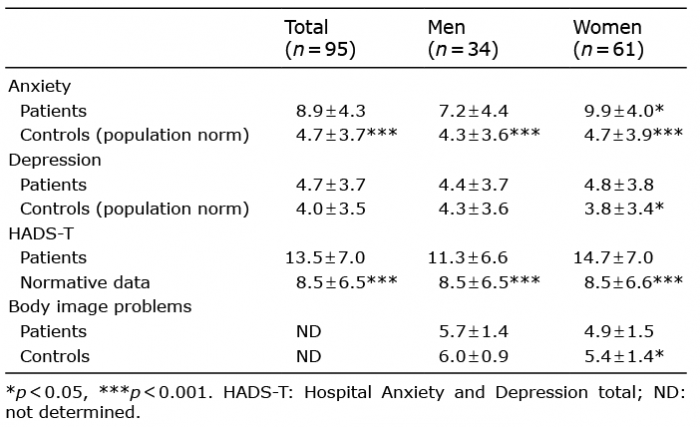
Patients were more anxious than the general population (score 8.9 ± 4.3 vs 4.7 ± 3.7 p < 0.001), but for depression the difference was less pronounced (score 4.7 ± 3.7 vs 4.0 ± 3.5 (not significant)). Women were significantly more anxious than men, score 9.9 ± 4.0 vs 7.2 ± 4.4, p < 0.05). In depression, there was no sex difference, but female patients were significantly more depressed than Swedish women in the general population (Table I). In (3) Zigmond and Snaith argue that scores in HADS below 8 are normal, while values above 11 signifies psychiatric problems. The single scale estimation then classified 41% of the patients as having manifest psychiatric disease.
Table I. Hospital Anxiety and Depression scale (HADS) results
The HADS-Total results are shown. A highly significant difference from normative values was seen for both sexes. Forty-three patients scored above the recommended >/=13 cut-off for HADS total (10 males and 33 females; 45%). This is close to the single scale estimation. Results of body image scores are presented. Women have a significantly decreased body image. The most significant correlation coefficients are shown in Table II. Anxiety correlated significantly highly with depression. HADS total correlates highly significantly with body image (Fig. 1).
Table II. Correlation coefficients (compared with Fig. 1)
Fig. 1. Correlation plot between total Hospital Anxiety and Depression Scale (HADS) and body image (BI).
Previous studies have established that anxiety and depression are frequent followers of PH, but the results show heterogeneity, probably due to variability in patient groups, clinical definitions and metric tools (1). Thus, it was decided to perform a study on a uniform patient material seen in July 2019. The aim was to measure the amount of psychiatric comorbidity and how body image values correlated with anxiety and depression in the patients.
Some investigators prefer the HADS total score as a general measure of “emotional distress” (5), as it seems to be more reliable than the subscales and correlates stronger with Becks Depression Inventory (BDI) and with Spielberger’s State Trait Inventory (STAI). Forty-five percent of the patients scored on or above the threshold for manifest psychiatric problems. Women usually score higher on HADS anxiety than men, while sex differences were not significant in this study, or in most other studies of HADS depression (6). Bragança et al. found 49.6% anxious patients among their 197 patients with PH, whilst depression frequency was within normal range (7). The results can be compared with results from other skin diseases (8). In this paper, describing patients from many European countries, it was found that anxiety and depression is frequent in dermatology. The authors found HADS values in psoriasis (with the 11+/= cut-off) of 13.8% for depression and 22.7% for anxiety. No dermatological diagnosis scored as high for anxiety as the patients with PH in the present work and in the study by Bragança et al. (7).
A strong correlation was found between body image and anxiety, as well as depression. A strong correlation was also found between HADS-T and body image. This fact could generate ideas, but taken alone, it is not proof of a causative role.
Study limitations
Nine of the patients were taking psychotropic drugs for anxiety or depression, which could be a confounder. It was not possible to follow the current patients as a cohort and obtain values before and after treatment, as the clinic closed.
Conclusion
Anxiety is frequent in PH. Further studies on the relationship between anxiety, depression and body image in PH are warranted. Measurement should be performed before and after treatment.


 Click to show fullsize
Click to show fullsize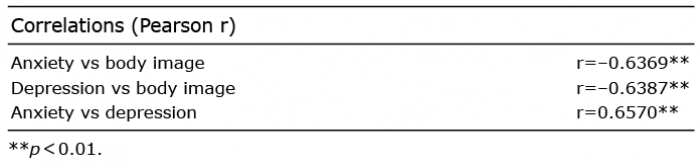 Click to show fullsize
Click to show fullsize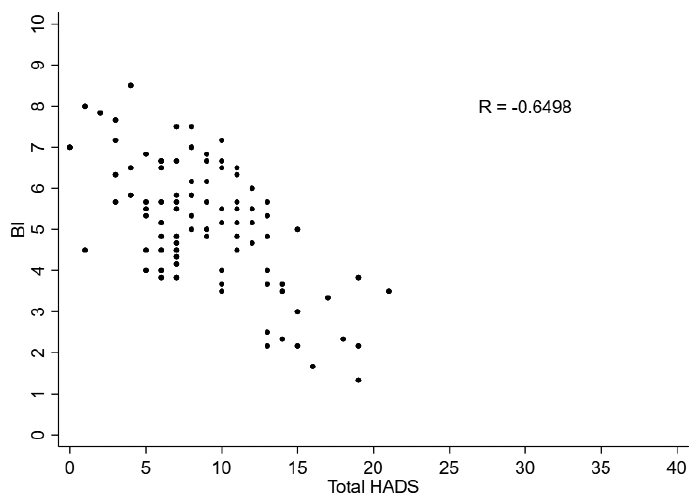 Click to show fullsize
Click to show fullsize