


1Department of Dermatology, University of Rzeszów, Rzeszów, and 2Department of Dermatology, Venereology and Allergology, Wroc?aw Medical University, Wroc?aw, Poland
Psoriasis is a chronic skin disease, that often develops below the age of 18. In an integrated approach to childhood psoriasis, the impact of psoriasis on family members merits consideration. In this study, the impact of childhood psoriasis on caregivers (61 mothers and 4 fathers) of 65 children (age range 5-17.5 years) was measured using Family Dermatology Life Quality Index (FDLQI). Childhood psoriasis exerted a substantial impact on the QoL of caregivers (mean FDLQI 13.62 ± 6.15 points). Caregivers rated routine household expenditure, time spent caring for the skin of the child, and emotional distress as the areas most impacted by psoriasis. The areas least affected were parent-child relationships, and caregivers’ social lives. The impact of other people’s reactions to the child’s disease was rated as more severe by caregivers of girls compared with those of boys (p = 0.004).
Key words: childhood psoriasis; quality of life; parents’ quality of life; family dermatology life quality index.
Accepted Jul 9, 2020; Epub ahead of print Jul 29, 2020
Acta Derm Venereol 2020; 100: adv00244.
Corr: Jacek C. Szepietowski, Department of Dermatology, Venereology and Allergology, Wroc?aw Medical University, Ul. Cha?ubi?skiego 1, PL-50-368 Wroc?aw, Poland. E-mail: jacek.szepietowski@umed.wroc.pl
Psoriasis is a chronic skin disease, which often develops in patients below the age of 18 years, and exerts a negative impact on the quality of life of both the child and their family members. In this study, the influence of childhood psoriasis on the caregivers of 65 children was measured using the Family Dermatology Life Quality Index (FDLQI). Childhood psoriasis exerted negative influence on caregivers’ QoL, with the greatest impact on routine household expenditure, the amount of time spent on looking after the child’s skin, and emotional distress. Impairment of the wellbeing of family members should be taken into consideration in an integrated approach to childhood psoriasis.
Psoriasis is a chronic inflammatory skin disease, in which one-third of cases develop before the age of 18 years (1). The disease has a significant impact on the wellbeing of affected children. Children with psoriasis often experience itching, social stigmatization and fatigue (2, 3). Psoriasis and atopic dermatitis (AD) are considered the chronic skin diseases with the greatest impact on quality of life (QoL) of children; the impact is comparable to that of many non-dermatological chronic childhood diseases, including asthma, renal disease, epilepsy and enuresis (4).
Chronic skin diseases not only affected the children directly, but also extend in an indirect fashion to their family members, partners and caregivers. Assessment of the QoL of individuals indirectly affected by a family member or partner with a skin condition represents a crucial component of the “Greater Patient” concept, introduced by Basra & Finlay in 2007 (5). The negative impact of a chronic childhood skin disease on the family members’ QoL has already been established in AD (6– 8). Several studies highlight the negative impact of psoriasis in adult patients on their relatives’ and partners’ QoL (9). Less is known about the effect of childhood psoriasis on the wellbeing of caregivers. Caring for a child with psoriasis may be time-consuming, affect physical well-being, lead to emotional distress and increase household expenditure. Recent studies indicate a high prevalence of depression (36%) and anxiety (36%) among parents of children with psoriasis (10).
The Family Dermatology Life Quality Index (FDLQI) has been reliably utilized in studies of the impact of childhood AD on parents’ wellbeing (8, 11). The aim of the current study was to investigate the impact of childhood psoriasis on the caregivers’ QoL using the FDLQI questionnaire, and to assess its correlation with clinical features.
The study was conducted among paediatric patients referred to the outpatient dermatology department in Wroc?aw over a period of 2 years (from January 2017 until December 2018). A total of 96 children with psoriasis were initially identified among new referrals or follow-up visits. The medical history of each child and their caregivers, including comorbidities, was obtained with a structured questionnaire. The diagnosis of psoriasis was made by a specialist dermatologist with particular expertise in paediatric dermatology, based on typical clinical presentation. Children with any chronic disease other other than psoriasis, that might impact the results, were excluded from the study. Thirty-one children with psoriasis were not included due to comorbidities (e.g. epilepsy, asthma, diabetes, mental retardation), parents’ refusal to participate or absence of the parent from the consultation. In total, 65 children with psoriasis and their caregivers agreed to participate and were included in the study. The severity of skin involvement was assessed by the same dermatologist (M.Z.) using Psoriasis Area and Severity Index (PASI) and percentage of body surface area (BSA) involved with skin lesions.
The relevant QoL questionnaires were completed both by parents and children during the consultation at the outpatient department following examination of the child. One caregiver of each child was asked to complete the validated Polish language version of the FDLQI questionnaire (12). These were predominantly mothers (61 cases, 93.8%). FDLQI is a dermatology-specific instrument designed to assess the impact of a dermatological condition on family members/partners (11). The questionnaire consists of 10 questions assessing various aspects of life, including emotional distress, physical well-being, personal relationships, dealing with the reactions of other people to a family member’s disease, social life, leisure activities, time spent caring for the relative/partner, everyday housework, job/study and household expenditure. Each question requires one response from 4 separate options: not at all/not relevant; a little; quite a lot; very much. The questionnaire refers to the impact of the relative’s cutaneous disease over the timeframe of the preceding month. Each question is scored from 0 to 3 points (0 points for the “not at all/not relevant” answer to 3 points for the “very much” answer) with a maximum FDLQI score of 30 points. Higher scores are associated with greater impairment of QoL.
The QoL of every child was assessed by means of Children’s Dermatology Life Quality index (CDLQI) or, in the case of adolescents aged 16 years and over, the Dermatology Life Quality Index (DLQI). The questionnaires were completed by the patients themselves or with the assistance of the parent, if necessary.
The study was approved by the Institutional Review Board. All study subjects (i.e. parents and children above 16 years) signed informed consent forms.
Statistical analysis
Statistical analysis was performed using Statistica® 12.0 Software for Windows. Data are presented as mean with standard deviation (SD) of the mean. Student’s t-test and Mann-Whitney U test were used for parametric and non-parametric analyses, respectively. Spearman’s correlation test was used for potential associations. p-value < 0.05 was considered to be statistically significant. Bonferroni correction for multiple comparisons was used where appropriate (p-value < 0.005 was considered statistically significant).
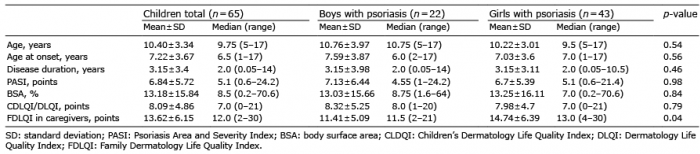
There were 43 girls (66.2%) and 22 boys (33.8%) included in the study. The age ranged from 5 to 17.5 years (mean ± standard deviation (SD) 10.4 ± 3.34 years). The mean age of onset was 7.22 ± 3.67 years (range 1–17 years) and the mean duration of the disease was 3.15 ± 3.4 years (range 2 weeks to 14 years). Mean PASI score was 6.84 ± 5.72 points (range 0.6–24.4 points) and mean BSA was 13.18 ± 5.72% (range 0.2–70.6%). Mean CDLQI (or DLQI in adolescents aged 16 years and over) was 8.09 ± 4.86 points (range 0–21 points). No differences were identified between boys and girls in terms of age, age of onset, disease duration, severity of skin involvement and impairment of the QoL. The clinical characteristics of children with psoriasis are summarized in Table I.
Table I. Characteristics of children with psoriasis
In the caregivers’ group, there were 61 mothers and 4 fathers (mean age 37.54 ± 6.84 years; age range 26–59 years). Six (9.23%) of the caregivers had psoriasis themselves. Other chronic conditions diagnosed in the caregivers included contact dermatitis (n = 2), rheumatoid arthritis (n = 1), asthma (n = 1), hypothyroidism (n = 1), vitiligo (n = 1), allergic rhinitis (n = 1), gastric ulcers (n = 1), chronic hepatitis C virus infection (n = 1), gout (n = 1) and multiple sclerosis (n = 1). The mean number of children in the family was 2.23 ± 0.96 (range 1–4). In 26 (40%) cases, the child included in the study was the only family member with psoriasis. Clinical characteristics of the caregivers are summarized in Table II.
Table II. Clinical characteristics of the caregivers (n = 65)
The FDLQI scores of the caregivers ranged from 2 to 30 points, with a mean value of 13.62 ± 6.15 points (median 12.0 points). No correlation was found between the FDLQI score and age of the patient, age of onset, disease duration and the severity as measured by PASI and BSA. The impairment of caregiver’s QoL expressed using the FDLQI score did not correlate with the impairment of the child’s QoL, either (detailed data not shown). The FDLQI score was not dependent on the caregiver’s age, personal history of psoriasis or total number of family members affected with psoriasis (Table III). The FDLQI scores obtained by the caregivers of girls with psoriasis were higher than the FDLQI scores obtained by the caregivers of boys with psoriasis (14.74 ± 6.39 vs 11.41 ± 5.09 points; p = 0.04), but did not reach statistical significance when Bonferroni correction for multiple comparisons was used.
Table III. Correlation between clinical features and Family Dermatology Life Quality Index score in caregivers (no statistically significant values were found)
The greatest impact of the child’s psoriasis was seen in the areas of caregiver’s routine household expenditure (2.08 ± 0.67 points), amount of time spent caring for the child’s skin (1.94 ± 0.73 points), and caregiver’s emotional distress (1.78 ± 0.96 points). Out of 10 FDLQI items, the areas least affected were personal relationships with the child and other people (0.72 ± 0.89 points), and social life (0.75 ± 0.85 points). Interestingly, the impact of other people’s reactions to their children’s cutaneous lesions was higher among parents of girls compared with parents of boys (1.58 ± 0.96 vs 0.82 ± 0.8 points; p = 0.004). The impact of childhood psoriasis on individual aspects of the caregivers’ QoL is summarized in Table IV.
Table IV. Impact of childhood psoriasis on individual items of the Family Dermatology Life Quality Index (FDLQI) questionnaire
The negative impact of psoriasis on paediatric and adult patients’ QoL is a well-known topic and has already been demonstrated in numerous studies (2, 3, 9, 13–16). The “Greater Patient” concept was proposed by Basra & Finlay (5) to draw attention to the secondary impact of skin diseases on the relatives, partners and/or caregivers of the affected patients. The importance of this concept is increasingly recognized, with a number of studies focusing on assessing the burden of cutaneous conditions among the patients and their family members/partners. In adult population, psoriasis has already been demonstrated to exert a negative impact on relatives, cohabitants and partners of affected patients (9, 17–19).
The impact of childhood psoriasis on parents/caregivers has been analysed in several studies, so far (10, 13, 20–23). Manzoni et al. (10) were among the first to demonstrate a high prevalence of depression and anxiety in caregivers of children with chronic skin diseases: psoriasis, AD and vitiligo. In the aforementioned study, 36% of caregivers of children with psoriasis demonstrated high levels of anxiety and depression according to the Hamilton Anxiety Scale and Beck Depression Inventory, respectively. Tollefson et al. (21) drew attention to the negative impact of childhood psoriasis on numerous aspects of the lives of the parents. Nevertheless, the authors did not utilize any validated QoL instrument. Instead, they conducted semi-structured interviews with the parents and presented results of these interviews in a narrative form. Tekin et al. (20), in a large multicentre study including 129 children with psoriasis, measured the influence of childhood psoriasis on the caregivers’ QoL using a validated Turkish language version of Dermatological Family Impact Scale. The authors demonstrated a significant impact of childhood psoriasis on caregivers’ QoL, in particular on the emotional distress. In addition, Dermatological Family Impact Scale score correlated with the impairment of the affected children’s QoL, measured using CDLQI, and severity of psoriasis, expressed using PASI. These results are also in accordance with the findings by Gånemo et al. (3), who investigated the impact of childhood psoriasis on QoL in 45 Swedish children and their parents using the Dermatitis Family Impact questionnaire with replacement of the word “eczema” by “psoriasis”.
The current study assessed the impact of childhood psoriasis on caregivers’ QoL using the FDLQI questionnaire. FDLQI is a dermatology-specific instrument developed by Basra, et al. in 2007 (11). It can be used to measure the impact of any skin disease on family members and/or caregivers, both in case of paediatric and adult patients. Although definite categorization of the FDLQI scores is missing, on the basis of similarity to the DLQI questionnaire it may be extrapolated that 0–1 points indicates “no effect on the caregiver’s life”, 2–5 points “small effect”, 6–10 points “moderate effect”, 11–20 points “very large effect” and 21–30 points “extremely large effect”. In the current study, the caregivers’ group consisted of 61 mothers and 4 fathers. Undoubtedly, the sex of the parent completing the questionnaire may raise controversy. In some cultures, there is a deeply embedded model of role division in the family, where mother spends more time taking care of the children and father is the main bread-winner. Current trends promote equal distribution of duties, but still cultural differences require consideration in studies focusing on childcare and QoL. Chernyshov (22) did not find any statistically significant differences in the way mothers and fathers assessed the impact of infantile AD on the affected children’s and their own QoL. The author concluded that the sex of the parent does not influence the results of studies regarding family impact of childhood AD. On the other hand, Marciniak et al. (8) compared the FDLQI scores of mothers and fathers of 46 children with AD and found significantly greater impairment of QoL in mothers than in fathers (17.1 ± 5.3 vs 14.7 ± 5.8 points; p < 0.001). However, we have not found similar studies regarding childhood psoriasis in the English language literature.
During our literature search, we identified one study, by Salman et al. (13), in which the FDLQI questionnaire was used to assess the impact of childhood psoriasis on the caregiver’s QoL. The authors included 58 Turkish children and adolescents with psoriasis (aged 7–18 years) and their primary caregivers, who were the mother, father and grandmother in 49, 8 and 1 cases, respectively. Despite the low median PASI score of the included children, the QoL of the primary caregivers was moderately impaired, with a median FDLQI score of 10 points (range 6.75–15.25 points). These findings suggest that psoriasis in patients under 18 years of age exerts a substantial impact on other family members, even when the severity of disease is relatively low. The current study included patients with more severe skin involvement (median PASI score of 5.1). The study by Salman et al. (13) was conducted in Turkey, whereas the present study was carried out in the Polish population. It is worth noting that the other available English language research concerning the impact of childhood psoriasis on the family (the aforementioned study by Tekin et al. (20)) was also conducted in Turkey. Therefore, cultural variations may influence the results of research related to childcare. It follows that that results from studies conducted in a certain country may not apply directly to other countries, in particular when there are significant differences in professed religion and valued family models.
This study has highlighted several important findings. First, childhood psoriasis exerts significant impact on caregivers’ QoL. The mean FDLQI score was 13.62 ± 6.15 points (median 12.0), which corresponds to “very large” effect on the caregiver’s life. The score was independent of the caregiver’s personal history of psoriasis, although the low number of cases with positive history (n = 6) affects analysis, and larger studies are thus required. Caregivers rated household expenditure, time spent caring for the child’s skin and emotional distress as the areas of the highest impact. Psoriasis in a child appears to have minimal impact on parent–child personal relationships and the social lives of parents. This may be an important factor influencing child’s well-being and ability to cope with the disease. In our analysis the impairment of caregivers’ QoL, expressed in FDLQI score, did not correlate with the duration or severity of childhood psoriasis, contrary to the findings reported by Salman et al. (13). Gånemo et al. (3) found significant correlation between the impairment of caregivers’ QoL and both PASI and CDLQI. However, neither the current study and nor that of Salman et al. (13) demonstrated a relationship between the caregiver’s and child’s QoL. We consider these to be important findings with potential future implications. Childhood psoriasis, even in cases of limited skin involvement and favourable wellbeing status of the child, may be a highly time-consuming and financially burdensome issue for caregivers, leading to substantial emotional distress. Therefore, psychological support must be offered to both the paediatric patients themselves, and to the family members who are indirectly affected.
An interesting observation was the difference observed between the sexes of children in the impact of childhood psoriasis on caregivers’ QoL. As described, there were no differences regarding age, disease duration or severity of psoriasis between boys and girls. In both boys and girls, the onset of psoriasis was approximately 7 years of age, which is in line with several previous studies and may presumably be related to the beginning of education at school (3, 23). Nevertheless, caregivers of girls (n = 43) tended to have higher FDLQI scores and score individual questions more severely than caregivers of boys (n = 22). Only one item of the questionnaire was found to reach statistical significance, and this area was that of other people’s reactions due to the child’s psoriasis (p = 0.004). Interestingly, similar observations were made by Chernyshov (24), who reported a more prominent impact on family QoL in girls with AD than in boys matched for age and disease severity. These findings may reflect a cultural emphasis on appearance that disproportionately affects women and girls compared with men, with an associated increased impact in those affected by visible skin pathology. Caregivers often hold themselves responsible for the condition of their children’s skin, and may experience a need to explain their children’s disease to others.
This research has some limitations. This is a single-centre study with a limited number of subjects included and no control group. The age of the children is also an important variable in studies on the QoL. As mentioned above, cultural and religious differences may also influence the results of studies regarding childcare. Therefore, larger, multi-centre controlled studies are required, grouped by age and sex, in order to reliably assess the impact of childhood psoriasis on family members in various populations. For these reasons, the current study may not apply to all paediatric psoriasis patients in different populations.
In summary, psoriasis may have a negative impact on the wellbeing of both affected children and their family members. These findings support the “Greater Patient” concept introduced by Basra & Finlay (5). Undoubtedly, childhood psoriasis requires an integrated approach with psychological support provided to both affected children and their caregivers.


 Click to show fullsize
Click to show fullsize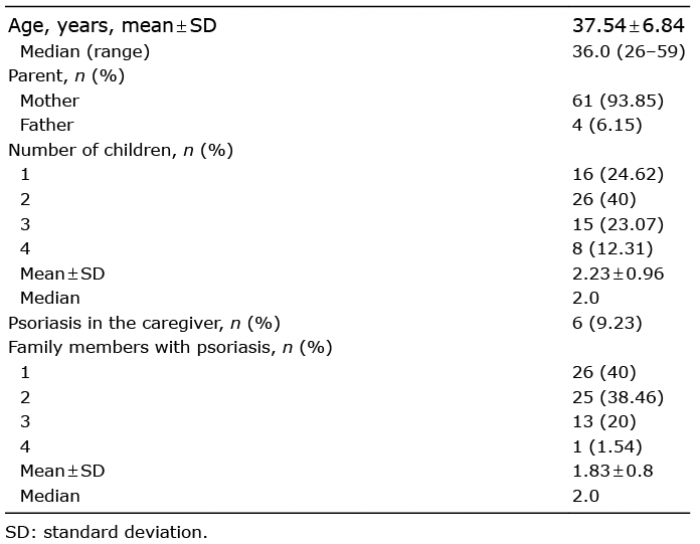 Click to show fullsize
Click to show fullsize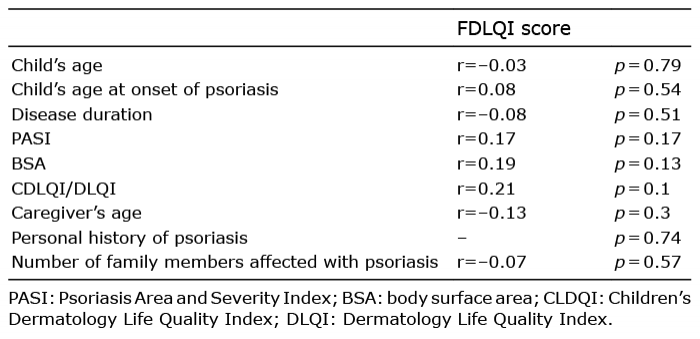 Click to show fullsize
Click to show fullsize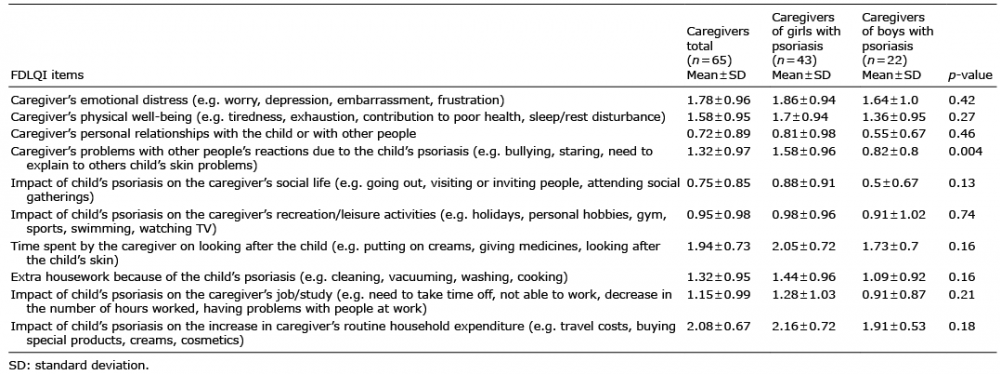 Click to show fullsize
Click to show fullsize