


1Shanghai Skin Disease Hospital, Tongji University School of Medicine, 1278 Baode Road, Jing’an District, Shanghai 200443 and 2Institute of Psoriasis, Tongji University School of Medicine, Shanghai, China. *E-mails: xuemei_yi@aliyun.com and dingyangfeng@hotmail.com
#These authors contributed equally to this work.
Accepted Aug 12, 2020: Epub ahead of print Aug 12, 2020
Acta Derm Venereol 2020; 100: adv00251.
Pustular psoriasis of pregnancy (PPP) is a challenging condition, which can have a serious effect on the life of a pregnant woman and her baby (1, 2). PPP is considered to be a rare form of generalized pustular psoriasis (1), which usually occurs in the third trimester and is characterized by desquamation, coalescent pustules, and systemic symptoms. Early recognition and treatment of PPP are of the utmost importance. Thus far, no standard treatment strategy has been developed for PPP, and the current treatment options are based on available case reports (3). We report here a case of a 37-year-old pregnant women with recurrent severe PPP who was treated successfully with secukinumab.
A 37-year-old patient at 26+1 weeks of her fourth pregnancy was referred to our clinic in June 2019 due to the sudden appearance of eruptive pustular lesions on her body 3 days previously. The patient presented with high fever (maximum temperature 39.1°C) accompanied by malaise, pain, itching, nausea, vomiting, chills and arthralgia. She also had oedematous red plaques with confluent pustules. The lesions were located predominately on her abdomen (Fig. 1a), groin, limbs (Fig. 1b), bilateral inner thighs and axillae. She had been diagnosed with psoriasis vulgaris at the age of 23 years. During her first pregnancy (age 24 years), pustular psoriasis occurred on a small area of her body in the 24th week. The symptoms were not severe, and she was treated successfully with topical corticosteroids. She gave birth to a healthy girl weighing 2,700 g. During her second pregnancy, which resulted in the delivery of a healthy boy, no rash appeared. During her third pregnancy (age 27 years), she developed PPP at the 12th week of pregnancy, with symptoms similar to the ones observed in the current pregnancy. Due to the potential negative impact on the developing foetus, she decided to have an abortion. Between pregnancies, the skin lesions showed mild plaque, which were visible on her skin, were controlled with topical corticosteroids. Her family history revealed no evidence of psoriasis or other skin diseases.
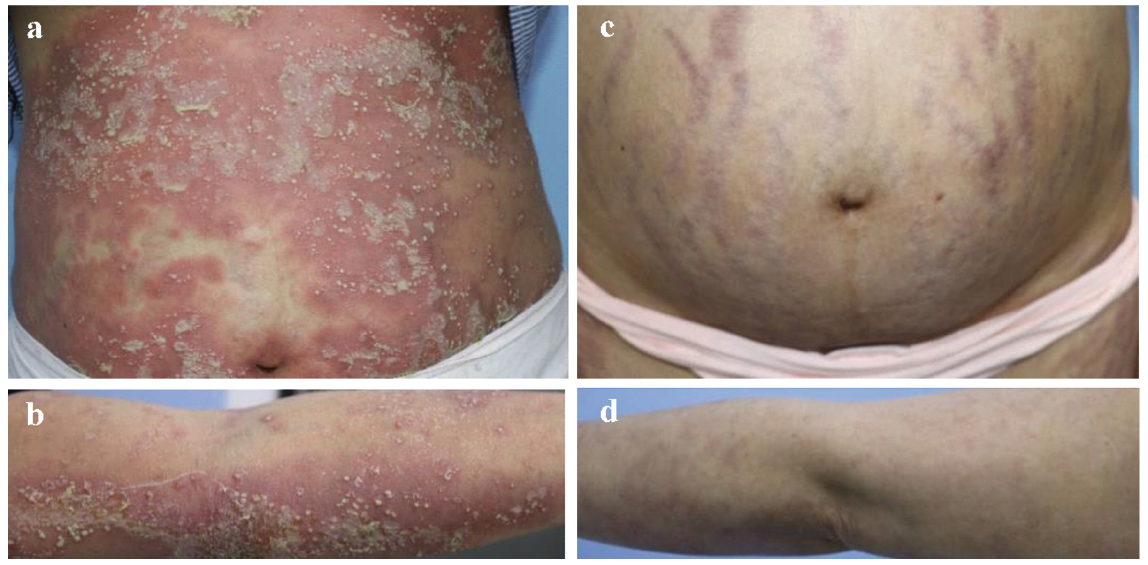
Fig. 1. Clinical photographs of the patient at 26+1 weeks of pregnancy showing oedematous red plaques with pustules (a) on the abdominal area and (b) on the limbs. (c, d) At 7 days after first administration of secukinumab, the erythema and oedema had improved (c: abdomen, d: limbs).
Blood tests showed a white blood cell count of 13×109/l (normal values 3.97–9.15×109/l), ery-throcyte count 4.16×1012/l (normal 4.09–5.74×1012/l), haemoglobin 129 g/l (normal 130–175 g/l), protein 53.8 g/l (normal 66–87 g/l), albumin 25.5 g/l (normal 39.7-49.4 g/l), C-reactive protein (CRP) 200.7 mg/l (normal 0–8mg/l), erythrocyte sedimentation rate (ESR) 28 mm/h (normal 0-20 mm/h), serum potassium level 3.13 mmol/l (normal 3.5–5.6 mmol/l), sodium 135 mmol/l (normal 136–145 mmol/l) and chloride 95.2 mmol/l (normal 96–110 mmol/l). Her renal, liver, and thyroid functions were normal, and her calcium levels were within the normal range. Tests for antinuclear antibodies, gestational pemphigoid auto-antibodies, tuberculosis, syphilis, hepatitis B, hepatitis C, and HIV were all negative. No bacteria were evident on microbial cultures of the pustular fluid and blood.
On admission to hospital, the patient received symptomatic treatment, including intravenous albumin and oral potassium chloride supplementation. She also received systematic treatment with cefuroxime. After completing all the tests, at 26+4 weeks of pregnancy, she provided informed consent for treatment with subcutaneous secukinumab at a dose of 300 mg. Four days later, some new small lesions appeared. After 7 days, her skin cleared completely. Considering the severity of her symptoms, a further 150 mg secukinumab was injected subcutaneously on days 7 and 14 after the first injection. During this period, the foetus and placenta were regularly monitored, revealing no evidence of any placental insufficiency. At week 39 of pregnancy, she gave birth to a healthy boy weighing 3,100 g via caesarean section. During the last follow-up (5 months after the start of treatment), no skin lesions were observed.
Previous studies have suggested that systemic corticosteroids may be effective in the management of PPP (4). First-line therapy for severe PPP usually consists of prednisone or prednisolone (doses ranging from 30 to 60–80 mg/day) (1). However, it has been reported that high doses of systemic corticosteroids may lead to complications, such as gestational diabetes, hypertension, and macrosomia (5). In addition, suspending corticosteroids after delivery may be challenging. In 2012, the medical board of the US National Psoriasis Foundation recommended cyclosporine as a suitable and safe first-line therapy for PPP during pregnancy (1). Moreover, some studies have suggested that tumour necrosis factor-alpha inhibitor (TNFi) may be effective for severe PPP. Infliximab and adalimumab have been shown to improve health conditions in patients with resistant PPP (6, 7). However, these drugs may increase the risk of pustular psoriasis (8). More recently, a new TNFi, certolizumab pegol, was tested for the prevention of active transfer across the placenta during pregnancy. The results suggested that the drug could be safely used during pregnancy and lactation (9); however, certolizumab has not yet been approved for the treatment of psoriasis in China.
The pathophysiology of general pustular psoriasis involves IL-17A, which has a critical role in pustule formation. Secukinumab is the first anti-IL-17 antibody that has been approved by the US Food and Drug Administration (FDA) for the treatment of moderate-to-severe psoriasis and psoriatic arthritis. Secukinumab has also been shown to be effective in the treatment of patients with PPP (10, 11). However, Chhabra et al. (11) reported that late use of secukinumab could not prevent intrauterine foetal death. Moreover, Kinoshita et al. (10) initiated secukinumab treatment after delivery; therefore, the effects on the foetus could not be observed.
The current patient received secukinumab as the first-choice treatment. Although some new small lesions were observed after 4 days, the skin lesions faded gradually, and complete remission was observed within 7 days after first administration of the drug. To the best of our knowledge, this is the first report on the successful use of secukinumab treatment in a patient with PPP resulting in successful delivery of a healthy infant.
In conclusion, in this case, treatment with secukinumab successfully reduced the skin lesions and placental inflammation. However, secukinumab has been shown to induce paradoxical pustular psoriasis, and ixekizumab (another anti-IL-17A biologic medication) has been shown to cause palmoplantar pustular psoriasis (9, 12). In addition, after treatment with brodalumab, patients have been shown to develop generalized pustular psoriasis (13). Further research is therefore needed to determine the efficacy and safety of these drugs in the treatment of severe PPP.
The Shanghai Health and Family Planning Commission (201840365) supported this study.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize