


1Department of Dermatology and Allergology, University of Ulm, DE-89073 Ulm, 2Department of Dermatology, Allergology and Venereology, and 3Lübeck Institute of Experimental Dermatology (LIED), University of Lübeck, Lübeck, Germany. E-mail: evelyne.tarnowietzki@uniklinik-ulm.de
Accepted Aug 21, 2020; Epub ahead of print Aug 27, 2020
Acta Derm Venereol 2020; 100: adv00301.
doi: 10.2340/00015555-3621
Anti-laminin 332 mucous membrane pemphigoid (MMP) is an autoimmune subepithelial blistering disorder predominantly involving the mucous membranes, which has a tendency to lead to scarring (1, 2). The disorder is caused by IgG autoantibodies against laminin 332 in the basal membrane zone of surface-close epithelia and the epidermis, and has been associated with an increased relative risk of cancer (3, 4). The most common associated malignancies are adenocarcinomas of the gastrointestinal tract, genital tract and the lungs (5). We report here a patient with anti-laminin 332 MMP presenting symblepharon due to conjunctival scarring and blisters on the extremities, who was soon afterwards diagnosed with non-small cell lung cancer, and therefore constituted a therapeutic challenge.
A 71-year-old man presented with a 3-month history of conjunctivitis. One month after the onset of this manifestation, cutaneous blistering occurred on his hands, knees and feet.
In addition, recurrent erosions affecting the mucous membrane of the nose were observed. Ocular examination revealed symblepharon formation along the inferior fornix on both eyes, and he had multiple serous- or haemorrhagic-filled blisters on the skin. Furthermore, the patient was an active smoker with 40 pack-years, and reported an unintended weight loss of 12 kg within 3 months.
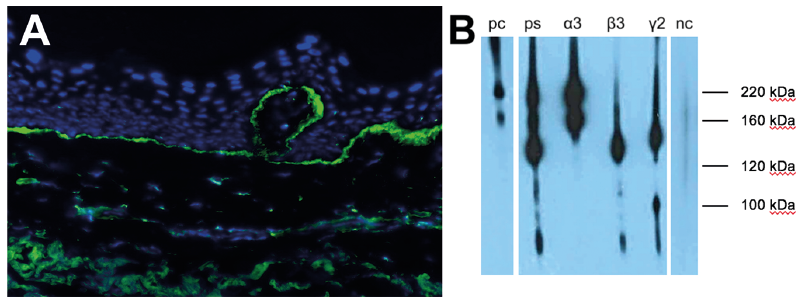
Skin biopsy revealed subepidermal separation and blister formation with a sparse lymphoplasmacytic infiltrate and linear alignment on the dermal–epidermal junction with anti-IgG and complement component 3 (C3) (Fig. 1A).
Initial indirect immunofluorescence staining (IF) revealed binding of IgG along the dermal side of salt-split human skin. On Western blotting, circulating IgG4 autoantibodies against the α3 and β3 chains of laminin 332 were detected (Fig. 1B).
Fig. 1. Direct immunofluoresecence (IF) and immunoblotting analysis. (A) Direct IF of perilesional skin biopsy shows linear binding of IgG (green). (Counterstaining with DAPI (4′,6-diamidin-2-phenylindol), original magnification ×40). (B) Immunoblotting of the patient’s serum (ps) with extracellular matrix of cultured human keratinocytes shows IgG antibodies against the 220-kDa and 160-kDa forms of the α3 chain and the 120-kDa β3 chain of laminin 332. Serum from a known anti-laminin 332 MMP patient is shown as positive control (pc), serum from a healthy volunteer as negative control (nc).
Abdominal ultrasound, chest X-ray, and subsequent computer tomography of the chest with biopsy of enlarged pulmonary lymph nodes led to a diagnosis of metastatic non-small-cell lung cancer with lymph node and adrenal metastases (pT3 pN3 cM1b).
The patient, who was at risk of rapidly developing irreversible blindness, was initially treated with once-daily doses of 2 mg prednisolone per kg bodyweight (i.e. a total of 140 mg/day), cyclophosphamide 50 mg/day and rituximab 1 g as the first of two doses originally scheduled to be administered in a two-weeks interval (the second dose was not applied), in addition to topical therapy. This therapy resulted in some improvement over the first week of treatment. After confirmation of the diagnosis of non-small-cell lung cancer, cyclophosphamide was discontinued due to its potentially cancer-promoting effect, and was replaced with an off-label treatment with the, often also, fast-acting intravenous immunoglobulin (IVIG). For personal reasons the patient declined palliative chemotherapy to treat his underlying lung cancer. Therefore, the paraneoplastic aetiology of anti-laminin 332 MMP and a possibly beneficial effect of tumour-burden reduction could not be proven in this case. Three cycles of IVIG therapy at 2 g/kg bodyweight (in the current case 140 g over 5 days) at intervals of 2 weeks resulted in almost complete resolution of the skin lesions and conjunctival erythema (Fig. 2). For personal reasons the patient also decided to stop any hospital treatment after the 3rd cycle of IVIG, in order to gain what he described as quality of life at home.
Fig. 2. Comparison of clinical findings before and after 6 weeks and 3 cycles of intravenous immunoglobulin therapy. (A) Ocular anti-epiligrin cicatricial pemphigoid with symblepharon formation along the inferior fornix of the left eye, in comparison with (B) less conjunctival injection and partial resolution of the symblepharon. (C) Multiple confluent haemorrhagic blisters on the left knee, in comparison with (D) residual hyperpigmentation as a sign of restitution.
The pathophysiology and underlying mechanism of why IgG autoantibodies target laminin 332 is little understood. Laminin 332 is known to be expressed in extracellular matrix of various malignancies and could be responsible for motility, adhesion and metastasis of tumour cells (6). However, within the complex immunological microenvironment of the tumour, immune cells may elicit a secondary immune response that leads to antibody production against laminin 332 of the tumour and, secondarily, to the basal membrane zone of the skin and mucosa tissues, leading to discontinuation of the dermal–epidermal junction (7, 8).
S3 guidelines for the management of MMP are currently being prepared and will replace the recommendations of an international panel of experts from 2002 (1) Treatment of MMP with ocular involvement is usually based on the long-term use of systemic corticosteroids combined with dapsone, or in progressive eye disease, with azathioprine or mycophenolate mofetil, and in severe cases with cyclophosphamide (7). In refractory cases, rituximab or IVIG are applied (8). In the current case, when we initially diagnosed a rapidly-progressing “high-risk” MMP, it was necessary to start with an effective treatment regimen including cyclophosphamide. However, as the non-small-cell lung cancer was diagnosed shortly afterwards, it was necessary to discontinue the initiated therapy using potentially malignancy-promoting immunosuppressive drugs, such as cyclophosphamide. After revealing the diagnosis of non-small-cell lung cancer and the absence of recovery of the skin lesions, therapy was switched to immunomodifying IVIG not associated with promoting malignancies or metastases. The patient presented with partial resolution of conjunctival inflammation and complete remission of cutaneous blisters (Fig. 2). IVIG has been shown previously to be effective in severe MMP in various case series (8, 9).
The case of anti-laminin 332 MMP reported here, diagnosed at almost the same time as the underlying non-small-cell lung cancer, constitutes a therapeutic challenge, because it requires fast-acting and efficient therapy to avoid irreversible side-effects, such as the loss of eyesight, resulting in a severe reduction in the patient’s quality of life. However, the choice of the immunosuppressive therapy is challenging, because the progress of the underlying malignant disease, due to immunosuppression, needs to be prevented. In the current case, the combination of high-dose prednisolone, rituximab and IVIG gave a promising response. However, long-term follow-up was not possible as the patient declined further treatment.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize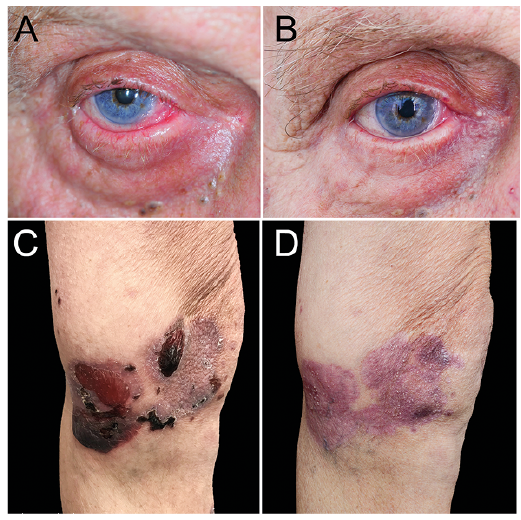 Click to show fullsize
Click to show fullsize