


1Department of Clinical and Experimental Medicine, Faculty of Health Sciences, Linköping University, Linköping, 2Dermatology and Venereology Unit, Department of Medicine, Karolinska Institutet, Solna, 3Division of Biostatistics, Institute for Environmental Medicine, Karolinska Institutet, Stockholm, 4Division of Dermatology and Venereology, Region Jönköping County, Jönköping, and 5Department of Dermatology, Lund University, Skåne University Hospital, Malmö, Sweden
#These authors contributed equally to this work and are shared last authors.
Evidence about the association of bullous pemphigoid and the risk of cancer is conflicting. Patients diagnosed with bullous pemphigoid (n = 5,739) between 2005 and 2016 were matched with a control cohort from the general population (n = 17,168) to estimate their overall and specific risk of cancer. The risk of squamous cell cancer of the skin (cSCC) was increased in patients with bullous pemphigoid (hazard ratio (HR) 1.3; 95% confidence interval (CI) 1.1–1.6). The risk of lymphoma within one year after bullous pemphigoid diagnosis was also increased (HR 3.1; 95% CI 1.3–7.6). While overall cancer risk prior to diagnosis of bullous pemphigoid was similar in cases and controls (prevalence odds ratio (POR) 1.0; 95% CI 0.9–1.0), the risk of male genital cancer within one year prior to diagnosis of bullous pemphigoid was lower in cases (POR 0.4; 95% CI 0.2–0.8). Clinicians must be aware of the increased risk of cSCC and lymphoma in patients with bullous pemphigoid.
Key words: cancer; epidemiology; bullous pemphigoid; autoimmune diseases; malignancy; skin diseases.
Accepted Aug 21, 2020; Epub ahead of print Aug 27, 2020
Acta Derm Venereol 2020; 100: adv00289.
doi: 10.2340/00015555-3622
Corr: Zeyad Albadri, Division of Dermatology and Department of Clinical and Experimental Medicine, Faculty of Health Sciences, Linköping University, SE-581 83 Linköping, Sweden. E-mail: zeyad.albadri@rjl.se
Bullous pemphigoid is an autoimmune skin disorder that has a huge impact on patients’ lives. It has been associated with an increased risk of cancer. To evaluate the significance of this association, data from 5,739 patients in Sweden with bullous pemphigoid were reviewed and compared with data from a control group with no previous diagnoses of bullous pemphigoid. The results show that the risk of squamous cell cancer of the skin is increased in patients with bullous pemphigoid. Patients were also more often diagnosed with lymphoma within one year after diagnosis of bullous pemphigoid. However, no increased overall cancer risk was found in patients with bullous pemphigoid.
Bullous pemphigoid (BP) is the most common autoimmune blistering disease. It mainly affects elderly people, and is characterized by autoantibodies against hemidesmosomal proteins within the dermoepidermal junction (BP180 and BP 230), resulting in subepidermal blistering (1). No proven cause has been found for BP; however, a number of different trigger factors have been described, such as medications, ultraviolet (UV) radiation and other skin disorders, such as psoriasis and lichen planus (2, 3). More than 50 drugs have been reported to trigger the onset of BP (4). A French and Finnish study revealed an increased risk of BP in patients treated with dipeptidyl peptidase-4 (DPP-4) inhibitors (5, 6). Several case reports and a recent meta-analysis confirmed the association between DDP-4 inhibitors and BP (7–10). In addition to environmental factors, genetic factors probably play a role in BP (11–13).
The annual incidence of BP has been estimated to range from 0.2 to 2.2 new cases/100,000 in different populations worldwide (14–17). A recent study from our group showed an annual incidence of BP of 7/100,000 in Sweden, which is one of the highest incidence rates in Europe (18). A current study from England shows increasing incidence numbers and high mortality among patients with BP (19), underlining the need for further studies on the association between BP and cancer.
Previous studies have shown conflicting results regarding the association of BP with malignancies. Several case reports and studies have shown a significantly increased risk of cancer in patients with BP (20–22). A cross-sectional study from Japan including 115 patients with BP reported a significantly increased risk of developing cancer after diagnosis of BP (21). On the other hand, other studies could not confirm an association between BP and increased risk of cancer (23–25). A population-based cohort study from Singapore of 359 patients with BP did not find a higher risk of cancer compared with controls (26). A Swedish study from 1990 reviewed 497 cases of BP without finding a correlation between BP and cancer (27), and a recent study from Taiwan did not show that cancer is a risk factor for BP (28).
The cancer risk among patients with BP compared with the general population has not been analysed previously in a large nationwide population-based study. The aim of this study was to evaluate the risk of cancer in patients before and after BP diagnosis.
Study population
This nationwide cohort study was conducted to examine overall and specific cancer risks in a population-based cohort of patients diagnosed with BP in Sweden. The study included all patients (aged 20 years and above) diagnosed by a dermatologist with BP using the International Classification of Diseases 10th Revision (ICD-10: L12.0, L12.0A, L12.0B, L12.0W, L12.8 and L12.9) listed in the Swedish National Patient Register (NPR) for the first time between 2005 and 2016. Patients under the age of 20 years were excluded, since BP is extremely rare in this age group. A total of 5,739 patients were identified with BP in the NPR (Table I). In Sweden, direct immunofluorescence (DIF), supported by clinical and histopathological findings, are considered the gold standard for diagnosis of BP. Diagnosis of BP in the NPR has been validated recently by our group, through a standardized review of medical records. The validation revealed a high positive predictive value of 92% (18, 29).
From Statistics Sweden a matched control cohort from the general population was generated (n = 17,168), i.e. 3 control subjects were matched to each BP patient, based on age, sex and county of residence at the date of the first diagnosis of BP for the case (Table I). The control subjects had no prior diagnosis of BP; otherwise their health status was representative of that of the general population.
Record linkage was permitted for both the BP cohort and the control cohort with the NPR, the Swedish National Cancer Register and the Swedish Cause of Death Register by means of each individual’s unique personal identification number (PIN). Electronic linkage to these nationwide databases resulted in complete follow-up.
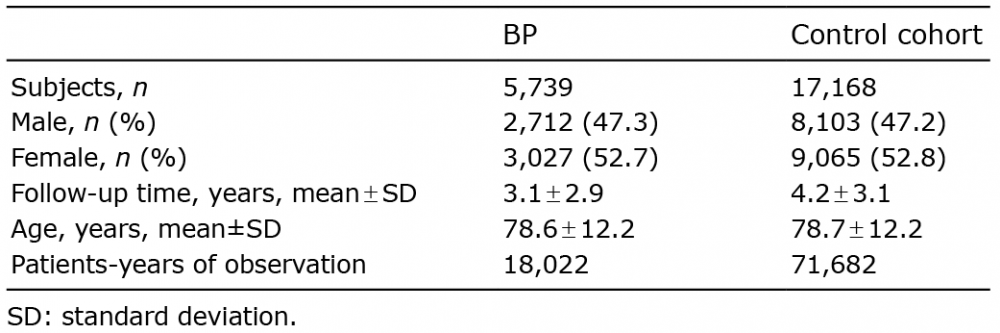
Table I. Demographic data for patients diagnosed with bullous pemphigoid (BP) and control cohort
Swedish National Patient Register
The Swedish NPR was launched by the National Board of Health and Welfare in 1964 and has virtually complete coverage of all inpatient care, both public and private. The NPR contains information about patient characteristics, such as PIN, sex, age and county of residence, administrative data, hospital identification and medical data (1 main and up to 7 secondary diagnosis). From 1997 diagnoses were coded in the NPR according to the ICD-10 revision. Inpatient coverage is close to 100% and 87% for outpatients (30). Since 2001, outpatient reporting became mandatory in the NPR. Primary care is not covered in the NPR (31).
Swedish Cancer Register
The Swedish Cancer Register (SCR) was founded in 1958 by the Swedish National Board of Health and Welfare and covers the entire Swedish population. The Swedish Cancer Register is considered to be of high quality, as almost 99% of cancer cases are morphologically confirmed (32). Data include information on tumour characteristics (site of tumour, histological type, basis and date of diagnosis) and follow-up data (date and cause of death and date of migration). Most cases of newly diagnosed cancers are registered by more than one source (clinicians, pathologists, cytologists) and reporting is compulsory, with a high reporting rate of 96% (33). Information about previously non-diagnosed cancers from death certificates is not included in the register. To be able to calculate person-years at risk the patient data-set was also linked to the Swedish Cause of Death Register, a register containing cause of death and the date for all deceased Swedish residents since 1961 (34).
Identification of cancer cases
During follow-up in this study, the ICD-7 was used to classify all incident cancers. All major cancer types (ICD-7 codes 140- 204.1) were included. ICD-7 code 191 included invasive and non-invasive squamous cell carcinomas of the skin (cSCC), but not basal cell carcinomas. Chronic lymphocytic leukaemia (ICD-7 code 204.1) was included among the lymphomas. Cancer types that did not belong to any of the above major types were placed in a group named “Other cancers” (Table II).
Table II. Hazard ratios (HRs) for specific cancer types over time in a cohort of 5,739 patients diagnosed with bullous pemphigoid (BP) compared with a matched control cohort (n = 17,168)
Statistical analysis
Hazard ratios (HRs) were calculated using multivariable Cox proportional hazards regression models. To control for confounding, the models include all matching variables by adjusting for age and sex, and stratifying by county of residence. Age was dichotomized into a group older than 80 years and those that were younger (as the reference group). HRs (representing the relative instantaneous risk of being diagnosed with cancer in the cohort of patients with BP compared with the control cohort during the follow-up time) and 95% confidence intervals (CIs) were calculated for the overall cancer risk and for the risk of all major cancer types. For the overall cancer risk analyses, all patients with a cancer diagnosis before baseline (BP diagnosis date) were excluded. For the specific cancer risk analyses, patients diagnosed with the same type of cancer before BP diagnosis were excluded from the cancer subgroup analysis. The person-years at risk were calculated from the date of the first BP diagnosis for each individual until the date of the first cancer diagnosis for each specific cancer, date of death or the end of the observation period (31 December 2016), whichever occurred first. Univariable logistic regression was used to examine the prevalence of cancer prior to diagnosis of BP, generating prevalence odds ratios (PORs) with 95% CIs. Standard errors were calculated using the cluster robust sandwich estimator in order to take within-patient correlation into account. The data were analysed using the statistical package STATA® software, version 15.1 (STATA Corp LLC, Texas, USA). Differences were considered significant at the 5% level.
Characteristics of patients with bullous pemphigoid and controls
The study identified 5,739 individuals, (3,027 female patients; 52.7%), diagnosed with BP in the NPR during 2005 to 2016. The mean ± standard deviation (SD) age at the time of BP diagnosis was 78.6 ± 12.2 years. The majority of the patients with BP were diagnosed in outpatient specialized clinics (83.2%, n = 4,773).
The total observation time was 18,022 person-years, with a mean ± SD follow-up of 3.1 ± 2.9 years among patients with BP (Table I). During follow-up, 38% of the controls (n = 6,604 out of 17,168) and 56% of the patients with BP (n = 3,218 out of 5,739) died. This resulted in an approximately one year longer mean follow-up time for the control cohort than for the patients with BP.
Overall and specific cancer risks
Among specific cancer types, patients with BP had a higher risk of being diagnosed with cSCC (HR 1.3; 95% CI 1.1–1.6). On the other hand, patients with BP had a lower risk of male genital cancer (HR 0.6; 95% CI 0.4–0.9) (Table II).
No significantly increased overall cancer risk (HR 1.0; 95% CI 0.9–1.1) for patients with BP was found in this study (Table II). A total of 307 incident cancers occurred in the BP cohort during the 11-year study period.
Cancers prior to diagnosis of bullous pemphigoid
A lower risk of male genital cancer was seen within one year prior to diagnosis of BP in the BP cohort (POR 0.4; 95% CI 0.2–0.8).
A total of 1,298 previous diagnoses of cancer were found among the patients with BP, giving a POR of 1.0 (95% CI 0.9–1.0) compared with the control cohort (Table III). The mean ± SD time between a previous diagnosis of cancer and BP diagnosis was 8.3 ± 6.6 years. Ten percent (n = 130) of the cancer cases were diagnosed during the year preceding diagnosis of BP (Table III).
Table III. Prevalence odds ratios (PORs) and 95% confidence intervals (95% CI) of cancer prior to bullous pemphigoid (BP) diagnosis
Cancer after diagnosis of bullous pemphigoid
An elevated risk of lymphomas was seen among patients with BP during the first year of follow-up (HR 3.1; 95% CI 1.3–7.6). However, the type of lymphoma (primary cutaneous or systemic or cell type of origin) could not be determined from the registry. After the first-year follow-up a higher risk of cSCC (HR 1.5; 95% CI 1.2–2.0) and a lower risk of male genital cancer were observed in the BP cohort (HR 0.5; 95% CI 0.3–0.8, Table IV).
During the first year of observation after diagnosis of BP 102 incident cancers occurred in the BP cohort (HR 1.1; 95% CI 0.9–1.4) (Table IV). Following the first year of observation after BP diagnosis, an additional 205 cancers were diagnosed in the BP cohort (HR 0.9 (95% CI 0.8–1.1).
Table IV. Overall cancer risk and risk of specific cancer types during and after the first year after bullous pemphigoid (BP) diagnosis in patients compared with a matched control cohort
This one of the largest cohort studies studying the association of cancer and BP. A major advantage of this study is the high validity for diagnosis of BP in the Swedish NPR (29). Data obtained from this study showed no increased overall risk of cancer among patients with BP; however, risk estimates for cSCC, male genital cancer and lymphomas differed from the control cohort.
Patients with BP had a higher risk of developing cSCC after the first year of follow-up. To the best of our knowledge this is the first study to demonstrate an increased risk of cSCC in patients with BP. It is not clear why cSCCs were higher for patients with BP, but this may be partly explained by increased frequency of health check-ups at dermatology clinics and surveillance for patients with BP. It cannot be excluded that immunosuppressive treatment started after BP diagnosis may play a role in developing cSCC (35). Other potential underlying mechanisms for this association between BP and cSCC might be UV radiation and autoimmunity. UV exposure is a well-known risk factor for skin cancer (36, 37) and, at the same time, a key factor in BP, leading to an unspecific epidermal injury and attraction of autoantibodies (38, 39). Autoimmunity itself may be a risk factor for developing cSCC in patients with BP (40). However, further studies are needed to gain a deeper insight into the mechanisms explaining the association between cSCC and BP.
This study revealed that the overall risk of male genital cancer (which includes prostate cancer, testicular cancer, and other unspecified male genital cancers) and the risk more than one year before and more than one year after diagnosis of BP was lower in patients compared with controls. To our knowledge, these findings have not been reported previously. These results are difficult to explain, and it is challenging to speculate that BP might be protective for male genital cancer. Interestingly, downregulation of bullous pemphigoid antigen (BPAG1) has been shown in prostatic cancer (41), and a loss of BPAG1 in invasive breast cancer cells (42). Further research is needed to confirm the present results and whether immunological cross-reactivity between epidermal and epithelial antigens, such as BPAG1, or other genetically or environmental factors are involved in protecting from male genital cancers.
Among all cancer types, the highest increased cancer risk was observed for lymphomas in BP patients during the first year of follow-up. The association between BP and lymphoma has been described in previous case reports (43–45). Possible mechanisms have been suggested for the increased lymphoma risk in patients with BP. One study proposed that antibodies to cancer-specific antigens might cross-react with the basement membrane leading to BP (43). Other authors suggested that infections or radiation might act as carcinogenic factors and, at the same time, cause basement membrane damage, explaining the association between lymphomas and BP (46–48). On the other hand, a German study revealed that it is unlikely that BP triggered haematological malignancies, especially in the period preceding the diagnosis of BP (49). However, increased risk of lymphoma has not been revealed in other population-based studies on BP, which, on the other hand, found different cancer types to be associated with BP. A 10-year population-based cohort study in Taiwan showed a higher incidence of brain and other nervous system cancers in patients with BP (28). A British national record linkage study revealed that patients with BP are at greater risk of kidney cancer than are controls (50). The current study did not confirm these results. Geographical and methodological differences between these studies, as well as genetic or environmental factors, might account for the different results.
Whether the overall cancer incidence for patients with BP is higher than for the general population is not known. Previous studies have investigated this relationship, revealing conflicting data about the association of BP with overall cancer risk. A small British case-control study revealed an increased risk of cancer, based on 15 subjects with cancer among a cohort of 84 patients with BP (34). In Poland, a population study of 110 patients with BP found that 11% of subjects in the BP group had increased risk of malignancy (20). A larger study has been carried out in Japan, including a total of 1,113 patients with BP, which found a significantly increased risk of cancer in patients with BP. The authors concluded that cancer screening is essential in all patients with BP (21). Another Japanese study, including 204 patients with BP, validated these results (23). In contrast to the above findings and, in line with the present study, several studies found no evidence of increased overall risk of cancer in patients with BP. A cohort study in Singapore, of 359 patients with BP, found no significant increase in the incidence of cancer compared with the matched general population (26). A large English population cohort study of 4,720 patients with BP in 2014 found no overall association between cancer and BP (50). These results are supported by a 2017 systemic review and meta-analysis (51).
Study limitations
The present study has some limitations. It cannot be excluded that unmeasured confounders lie behind the increased cancer risk found. However, to control for confounding, cases were matched with controls regarding age, sex and county of residence. Since a previous history of cancer may be a risk factor for subsequent cancers, especially skin cancer, all patients with a cancer diagnosis before baseline were excluded. The registry-based data in the current study does not include clinical and immunological characteristics of the patients, and administrative data are subject to coding errors. The NPR was validated recently, revealing a high PPV for BP diagnosis. However, it cannot be completely excluded that patients with only a single diagnosis of BP in the NPR are not true cases, leading to an overestimation of cases of BP. Ascertainment bias should be considered when interpreting these findings. Patients with an index diagnosis, such as BP, are more likely to be diagnosed with another disease than are patients without an index diagnosis. This bias could lead to an increase in the rate of cSCC and lymphoma among patients with BP. Despite the high quality of the NPR, it does not include data from primary healthcare centres. However, most patients with BP are diagnosed and treated as outpatients in dermatology clinics in Sweden. The BP patients’ follow-up time was shorter than in the control cohort. This difference might skew the results in the current study. The shorter mean follow-up time is due to the higher mortality among patients with BP compared with the general population.
In conclusion, this study showed that patients with BP do not have an increased overall risk of cancer, but are at increased risk of developing cSCC and lymphoma. Further studies are needed to confirm these findings. However, the present results highlight the importance of early detection of cSCC and lymphoma in these patients, especially during the first year after diagnosis of BP.
This study was funded by Karolinska Institutet, the Welander-Finsen Foundation and Sigurd and Elsa Goljes Foundation.
The Regional Ethical Review Board in Stockholm, Sweden has approved this study.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize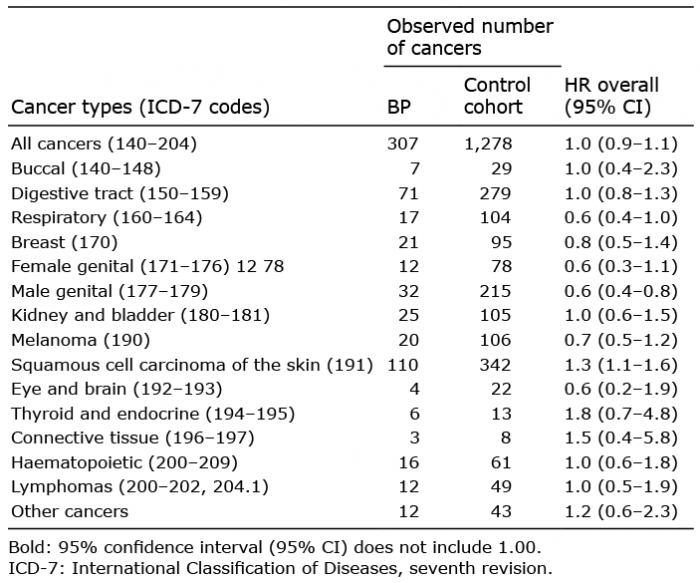 Click to show fullsize
Click to show fullsize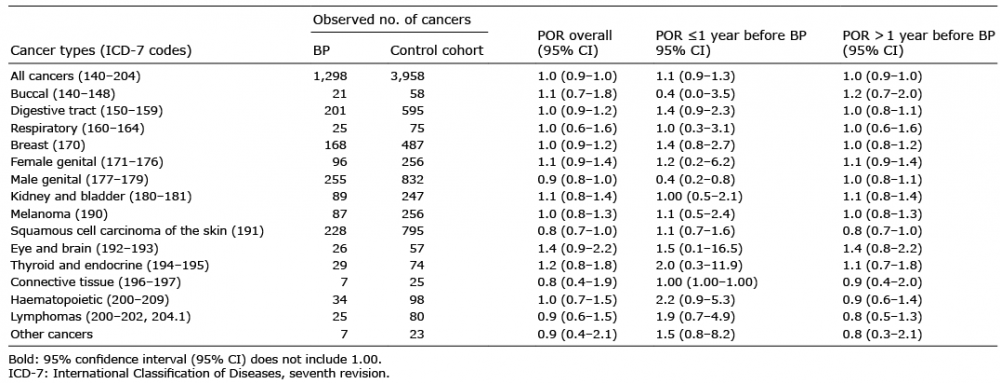 Click to show fullsize
Click to show fullsize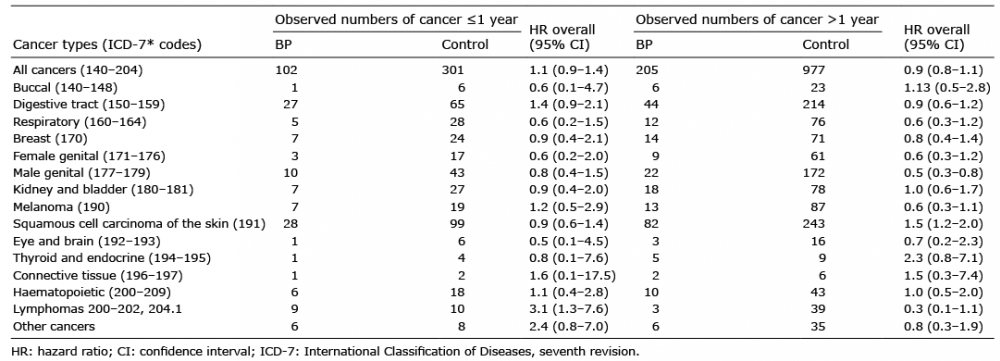 Click to show fullsize
Click to show fullsize