


1Skin Cancer Centrum, Theme Cancer, A6:01, Karolinska University Hospital, and 2Department of Oncology-Pathology, Karolinska Institute, Stockholm, Sweden
#These authors contributed equally to this work.
Radiotherapy is often used to treat lentigo maligna. However, the long-term efficacy and safety of radio-therapy approaches have not been thoroughly evaluat-ed. We aimed to evaluate the long-term efficacy and safety of ultrasoft X-ray/Grenz ray treatment in the patients. A total of 161 lesions from 159 patients received treatment with Grenz ray between 2005 and 2007. Follow-up of recurrence was performed 10 years after the final treatment. In the study setting, the cure rates were 97% for primary therapy with Grenz ray alone and 100% when Grenz ray was combined with partial or radical excision. The treatment is well tolerated, simple to perform, and has an excellent cosmetic outcome, with 94% of patients pleased with the results. Grenz ray is painless, effective, and safe for use when surgery is not feasible. Thus, Grenz ray can be considered as a standard treatment option for lentigo maligna.
Key words: Grenz ray; lentigo maligna; lentigo maligna melanoma; radiotherapy.
Accepted Sep 7, 2020; Epub ahead of print Sep 14, 2020
Acta Derm Venereol 2020; 100: adv00282.
doi: 10.2340/00015555-3631
Corr: Ada Girnita, Skin Cancer Centrum, Theme Cancer, A6:01, Eugeniavägen 3, Karolinska University Hospital and Department of Oncology-Pathology, Akademiska Stråket 1, Karolinska Institute, SE-171 77 Stockholm, Sweden. E-mail: Ada.Girnita@ki.se
Radiotherapy with ultrasoft X-ray/Grenz ray is used to treat lentigo maligna melanoma, but the long-term efficacy and safety of this treatment has not been evaluated. This study assessed 161 lesions treated between 2005 and 2007. After 10–12 years of treatment, the treated areas were examined for recurrence. In the study setting, the cure rate achieved in primary therapy was 97% and increased to 100% when combined with partial or radical excision. The treatment is effective, and safe for use when surgery is not feasible, and has an excellent cosmetically outcome. As such, it should be considered as a standard treatment option for lentigo maligna melanoma.
Lentigo maligna (LM) accounts for 83% of cases of melanoma in situ in the USA, and the incidence rate is increasing compared with that of other melanoma subtypes (1–3). In Sweden, LM is 3 times more common than superficial spreading melanoma (SSM) (4, 5).
Grenz rays (soft X-rays) have been used successfully in treating LM and LM melanoma (LMM) in Europe. How-ever, the use of this approach has not been thoroughly evaluated (6, 7).
The aim of this study was to determine the risk of long-term recurrence and patient-reported cosmetic outcomes in patients with LM or LMM who received treatment with GR alone or GR plus partial or radical surgery from 2005 to 2007.
Patients and study design
This study is based on the cohort reported by Hedblad et al. (8), comprising 593 patients with LM or early LMM, treated with GR between 1990 and 2009 at the Department of Dermatology, Karolinska University Hospital, Stockholm, Sweden. To minimize potential differences due to clinical evaluation, all patients were examined by the same group of dermatologists within one year. To minimize variations in the 10-year follow-up interval, the study selected a group of 159 patients receiving the last GR treatment no earlier than 2005 and no later than 2007.
The inclusion criteria were: verified LM or early LMM; micro-invasive or in horizontal growth phase; less than 0.4-mm invasion depth, regardless of adnexal atypical melanocytic extension; and treatment period between 2005 and 2007 at the Department of Dermatology, Karolinska University Hospital, Stockholm, Sweden.
The exclusion criteria were: patients who died during the study period; patients unwilling or unable to participate; and patients living outside Stockholm. One patient was also excluded because they had received additional GR treatment after 2007.
The patients who met these criteria were further divided into 3 groups according to the given treatment. Group 1 received GR as primary single therapy; Group 2 underwent surgery followed by adjuvant GR due to positive margins; and Group 3 received surgery with negative margins followed by prophylactic adjuvant GR. Specifically, the prescribed doses were: 120 Gy for surgically removed LM/LMM or lesions with no proliferation along adnexal structures; 140 Gy for lesions with proliferation along adnexal structures up to or equal 0.6 mm; 150 Gy for proliferation between 0.6 and 0.8 mm. In all cases, the prescribed dose was divided into 6 sessions (2 sessions per week for 3 consecutive weeks).
For follow-up, the area with previously diagnosed LM/LMM was examined for recurrence by ocular inspection, magnification lamp, and dermatoscopy. If recurrence was suspected, a biopsy was taken for histological analysis. Cosmetic results, including atrophy, telangiectasia, hypopigmentation, and hyperpigmentation, were assessed via a patient questionnaire and by comparison with medical journal-documented images acquired prior to GR treatment. If atrophy was related to the surgical or biopsy procedures, the patient was not included in the analysis. During the design of the current study, there were no standardized approaches available for measuring cosmetic outcomes after GR treatment in randomized controlled trials. In order to evaluate patient-reported cosmetic outcomes, the patients were asked their opinion on overall aspects of the treated area compared with the rest of their face using a 3-grade scale questionnaire (very pleased, pleased, or not pleased).
This follow-up study was approved by the Regional Ethical Review Board of Stockholm (approval no.: 2017/1511-31/2) and was performed according to the principles of the Declaration of Helsinki. All patients provided informed consent for participation.
Statistical analysis
Differences in cosmetic outcomes of patients treated with GR, partial excision and GR, or radical surgery and GR, were tested using Pearson’s χ2 tests and 1-way analysis of variance (ANOVA), Fisher’s exact tests, and Wilcoxon rank-sum tests. Pearson’s χ2 tests and Fisher’s exact tests were used to determine whether there were significant differences between the expected and observed frequencies in one or more categories. Fisher exact tests were used when the numbers were small and if the values of any of the cells in the contingency table were < 5. Differences in continuous variables were tested by 1-way ANOVA or Wilcoxon rank-sum tests; the latter was used if the assumption of normal distribution was not met. The level of significance was set as α=0.05. Disease-free survival was calculated using the Kaplan–Meier method. All statistical analyses were performed using SAS version 9.3 (SAS Institute, Inc., Cary, NC, USA).
Patients
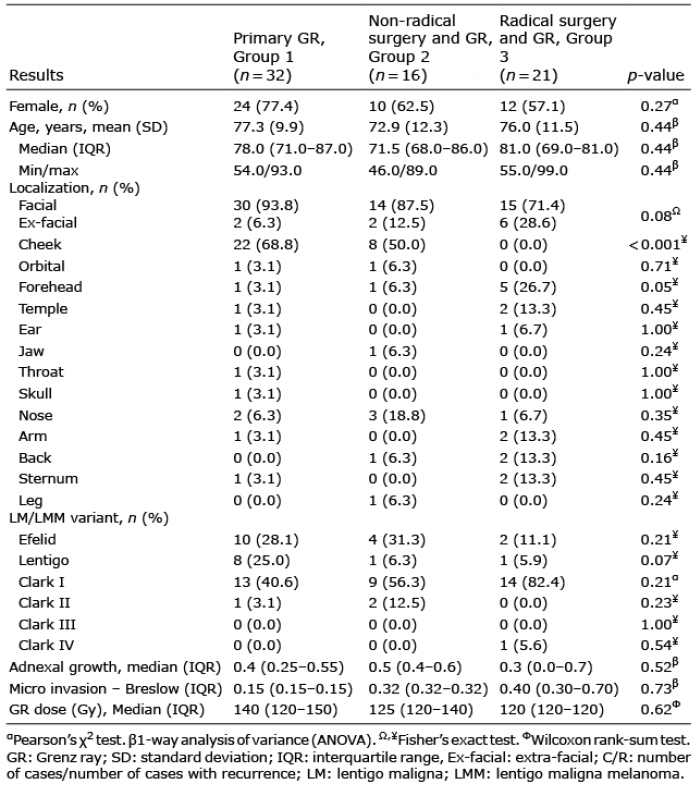
From 159 patients originally included, 62 (39%) had died by the time of the 10-year follow-up; 3 due to metastatic melanoma. Nonetheless, all medical records were evaluated for recurrence of LM. Twenty-nine patients (18%) could not attend follow-up due to geographical distance or poor health status associated with advanced age or comorbidities. The final cohort included 70 lesions from 69 patients clinically evaluated at 10-year follow-up after GR treatment. Of these patients, 70% were women, and the mean age during GR treatment was 64.5 years (range 38–88 years). Table I shows the demographic features, lesion localization, and treatment type for the patients included in the current study. The majority of treated lesions (83%) were facial, and the most common site was the cheek (50–68.8%; n = 30), followed by the forehead (10%; n = 7).
Six patients received additional GR treatment before the 5-year follow-up, as reported previously by Hedblad et al. (8), owing to local recurrence or persistent lesions. At the time of this study, all of these patients showed complete clearance.
Table I. Demographic, clinical, histopathology, and anatomical distributions of patients in this study
Recurrence
GR was curative and showed complete clearance after 10 years in 97% of patients with LM/LMM. Two cases of recurrence were observed; both women with cheek LM, who were treated with GR without prior surgery.
The first patient had an ephelid stadium LM with 0.2-mm adnexal extension treated elsewhere with laser and cryotherapy prior to GR in our unit in 2007. Follow-up was discontinued after the patient moved to another county. According to the medical records, the patient had histologically confirmed relapse 6 months after GR and was treated with surgery twice. After another 8 years, the clinician suspected recurrence of LM and referred the patient to our hospital. At the time of the current study, a 1-mm light brown macula with grey dots was visible in the GR area, and a tangential biopsy confirmed recurrence of LMM with adnexal extension (0.7 mm) (Fig. 1). The patient underwent another GR treatment and again enrolled in our follow-up programme.
The second patient had 2 separate lesions on the same cheek. The first LM had an adnexal extension of 0.5 mm and was treated with partial surgery in 2003, followed by 2 sessions of GR at an interval of one year owing to relapse on the edge of the GR treated area. The second LM was initially treated with GR. The LM that recurred was the first one. The recurrent lesion had a 0.4-mm adnexal extension and was treated with one fractionated GR; the relapse was noticed again at the edge of the GR treatment area during follow-up.
Nine of 68 patients (13%) had another melanoma or LM/LMM. There were no cases of non-melanoma skin cancer identified in the areas treated with GR.
Fig. 1. Lentigo maligna recurrence. Clinical 10-year follow-up; 1-mm light-brown macula 2.5 cm from the surgical scar. (A) Dermatoscopy with light-brown pigmentation arranged in lines; (B) histological recurrence with melanocytic atypia (Hematoxylin eosin staining).
Cosmetic results
Overall, most patients (64 of 68) were very pleased with the results of GR treatment, although cosmetic side-effects were noted (Table II). Briefly, telangiectasia was present in 16 subjects (50%) in Group 1, 7 (43.8%) in Group 2, and 12 (57.1%) in Group 3. Hypopigmentation was prevalent, with over 80% of patients affected in all 3 groups (Fig. 2); this condition was observed in 27 subjects (84.4%) in Group 1, 15 (93.8%) in Group 2, and 18 (85.7%) in Group 3. In addition, hyperpigmentation was present in 22 subjects (68.8%) in Group 1, 9 (56.3%) in Group 2, and 6 (28.6%) in Group 3. Atrophy was present in 10 subjects (31.3%) in Group 1, 5 (31.3%) in Group 2, and 7 (33.3%) in Group 3. Notably, hyperpigmentation was most common in subjects who received GR only (68.8%), and atrophy was the least common cosmetic side-effect in 30% of subjects (Table II).
Table II. Cosmetic results
Fig. 2. Box-plot of the treatment groups according to the radiation dose. Primary Grenz ray (GR), non-radical surgery and GR, and radical surgery and GR were evaluated.
Hyperpigmentation was significantly higher in patients receiving primary GR than in those receiving partial or complete excision (p = 0.01). Our findings also suggest a correlation between GR dose and the occurrence of hyper-pigmentation. Four patients with hyperpigmentation showed only basal epidermal hyperpigmentation with immunohistochemistry staining negative for melan-A (Fig. 3).
Fig. 3. A 77-year-old woman with hyperpigmentation. (A) Ten-year follow-up with hyperpigmen-tation. (B) Basal hyperpigmentation was observed histologically, but no recurrence was detected, and melanocytes were normal (Hematoxylin eosin staining).
Deceased patients
Three patients in the cohort died due to melanoma metastasis. The first patient was a 91-year-old woman with LM on her right cheek. The original tumour was an LM without invasion, treated elsewhere with curettage and cryosurgery. The tumour recurred, and the patient underwent surgery (radical excision); histology confirmed the non-invasive nature of the tumour. The patient received GR treatment in 2007 and was free from recurrence during the 5-year follow-up. Six years after GR treatment, the patient developed a metastatic lesion in the right maxillary sinus. New skin samples from the previously treated area did not confirm local recurrence. The patient received conventional radiotherapy for the metastatic lesion in 2013, but died in January 2018 due to complications of the disease.
The other 2 deceased patients had thicker SSM else-where on the body, which most likely contributed to metastasis and death.
The incidence rates of LM and LMM have increased in the past 20 years world wide (3). The lesions associated with LM and LMM typically have indefinable borders, resulting in a high rate of recurrence (8).
The treatment of choice for LM/LMM is surgical excision, which also allows complete histological analysis and removes the deep periadnexal melanocytes and the invasive component. Unexpected invasion foci have been reported in 16–50% of excised LM lesions (9, 10). The recommended surgical margin of 5–10 mm can be difficult to achieve when the LM/LMM is situated close to critical anatomical structures (8, 11). The recurrence rate has been reported as approximately 6–9% (7). In a 5-year follow-up, Zalaudek et al. (12) reported a 6.8% recurrence rate for LM after surgical excision, compared with a recurrence rate of 31.3% for LM treated with other methods. This high recurrence rate is often associated with subclinical atypical junction melanocytic hyperplasia beyond visible margins and difficulties in identifying such atypical isolated melanocytes in sun-damaged skin (8, 13, 14).
Mohs micrographic surgery is associated with a low recurrence rate of 0.5–5% (7, 15, 16). Melanocytic lesions are more difficult to visualize in haematoxylin-eosin-stained frozen sections, because melanocytes may be altered during the freezing process (17). Moreover, keratinocytes may appear vacuolated, thereby mimicking melanocytes, and inflammatory cells can cover invasive areas (17, 18). Immunohistochemical staining is not performed using frozen sections (2). Instead, confocal microscopy is often used to define LM/LMM margins before staged surgery (19–23).
Cryotherapy is also used to treat LM when surgery is inappropriate; however, standard treatment protocols have not yet been developed, and the recurrence rate can be as high as 34% (1, 2, 12). Imiquimod 5% cream is an immune response stimulator that enhances both the innate and acquired immune pathways (particularly T helper cell type 1-mediated immune responses). It has also been used in the treatment of LM with positive margins, resulting in clearance rates of 77–82% (24–26). The treatment schedule for imiquimod 5% cream consists of at least 60 applications during the whole treatment, which can be inconvenient for elderly patients (26). However, data regarding long-term follow-up and evidence of recurrence are limited (27). An ongoing, mainly Australian-based, phase III study is investigating the effectiveness of using either radiotherapy (RT) or imiquimod (ImiQ) to treat LM when surgery is not possible, is refused, or fails (28).
Photodynamic therapy (PDT) in association with fractional ablative CO2-laser to enhance absorption is also emerging as a therapeutic strategy in LM. In a recent study by Räsänen et. al (29), the LM area was pretreated with fractional ablative laser before PDT treatment 3 times with 2 weeks’ interval. Four weeks after treatment LM is excised surgically using 5-mm margins. The efficacy of PDT was assessed after surgical excision, by histopathological examination and immunohistochemical staining. The complete histopathological clearance rate was 7 out of 10 LMs (70%).
Since 1954, radiation therapy (RT), particularly GR treatment, has been used as a non-invasive treatment, exhibiting clearance rates comparable to those of conservative surgery (7, 30, 31). GRs are a type of superficial RT (typically 10–20 kV) and only penetrate the epidermal/dermal interface (no deeper than 2 mm). Thus, GR has been used as a definitive or adjuvant treatment after finding positive margins following excision of LM/LMM (7, 30). The GR doses penetrating the skin decreased exponentially with distance; thus, LM that histologically presents a depth of extension of more than 0.8 mm should not be treated with GR (8, 29). Moreover, when using a machine with 10 kV voltage (D ½=0.5 mm), high doses (150–160 Gy) are recommended in areas with hyperplastic adnexal structures, such as the nose and bearded areas, to avoid relapse.
In Europe, ionizing radiation, particularly soft X-rays (10–20 kV, D ½=1 mm), has been used as an adjuvant or primary treatment for LM, resulting in recurrence rates of 0–14% (14, 30, 32). Two previous series were reported; the first by Hedblad & Mallbris (8) showed a mean recurrence time of 18.8 months and a cure rate of 83–90%, whereas the second by Farshad et al. (32) showed a mean recurrence time of 45.6 months and a cure rate of 93%.
To the best of our knowledge, this is one of the longest follow-up studies of patients receiving GR (up to 10 years). In the current study, the cure rate achieved in primary therapy with GR was 97%; this was increased to 100% when combined with partial or radical excision (Table III). The treatment was well tolerated, simple to perform, and had excellent cosmetic outcomes, with 94% of patients indicating that they were pleased with the results.
Side-effects, including acute dermatitis and necrosis appearing shortly after treatment, are common, and last approximately 2–4 weeks. Hyper- and hypopigmentation, skin atrophy, and telangiectasia usually appear 6 months after radiation (8). In the current study, hyperpigmentation was associated with higher doses of radiation in primary therapy.
There were some limitations to this study. For example, confocal microscopy was not performed during follow-up. Thus, additional studies are required to confirm these findings using confocal microscopy.
In conclusion, GR is a painless, effective and safe method for treatment of LM/LMM when surgery is not feasible and can be considered as a standard treatment option.
Table III. Kaplan–Meier disease-free survival
The paper was funded entirely by AGs grants from the Swedish Cancer Society, Edvard Welanders Stiftelse, Cancer Society in Stockholm and the King Gustaf V Jubilee Fund. None of grants agencies has influenced the outcome of this paper. We thank the statistical team at LIME Karolinska Institute and the pathology and medical photography teams at Karolinska University Hospital.


 Click to show fullsize
Click to show fullsize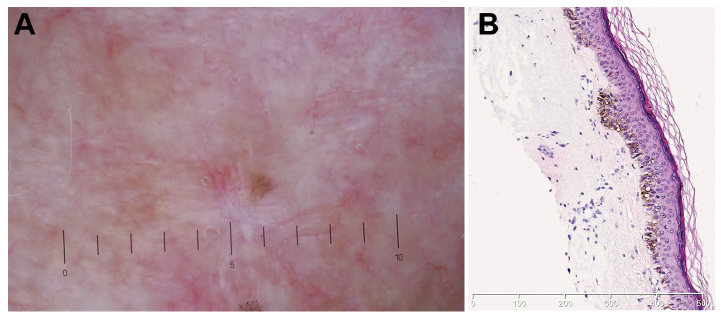 Click to show fullsize
Click to show fullsize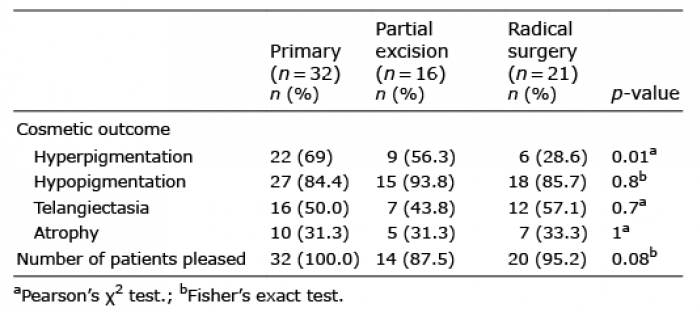 Click to show fullsize
Click to show fullsize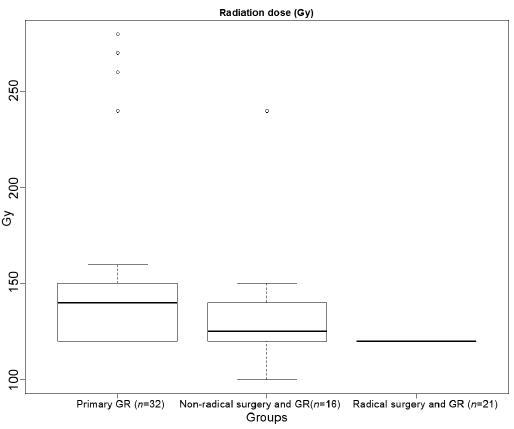 Click to show fullsize
Click to show fullsize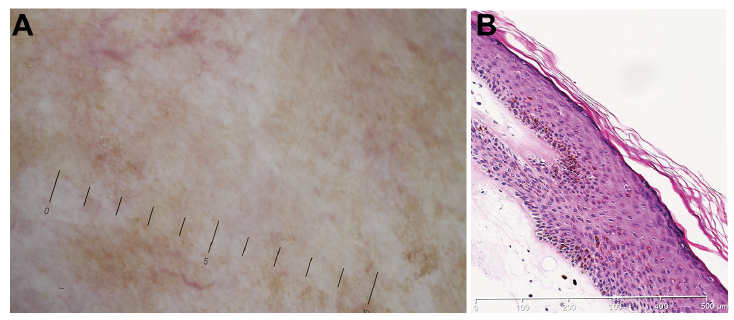 Click to show fullsize
Click to show fullsize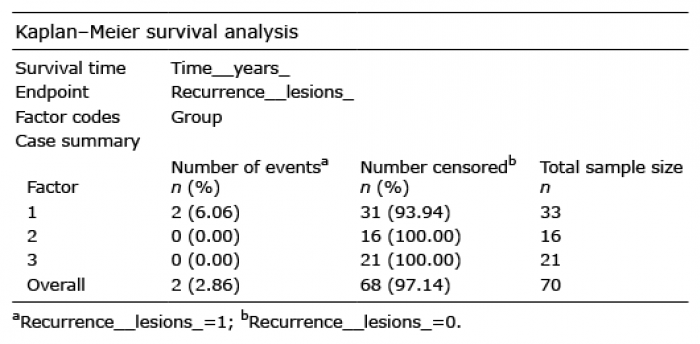 Click to show fullsize
Click to show fullsize